Topic
Longevity Medicine
NAD+, senolytics, rapamycin, hormone optimization, and evidence-based longevity interventions. Beyond anti-aging marketing — what the science actually supports.
Explore by Topic
NAD+ Therapy
Nicotinamide adenine dinucleotide IV infusions and precursors for cellular energy restoration.
Senolytics
Selective elimination of senescent cells to reduce chronic inflammation and aging.
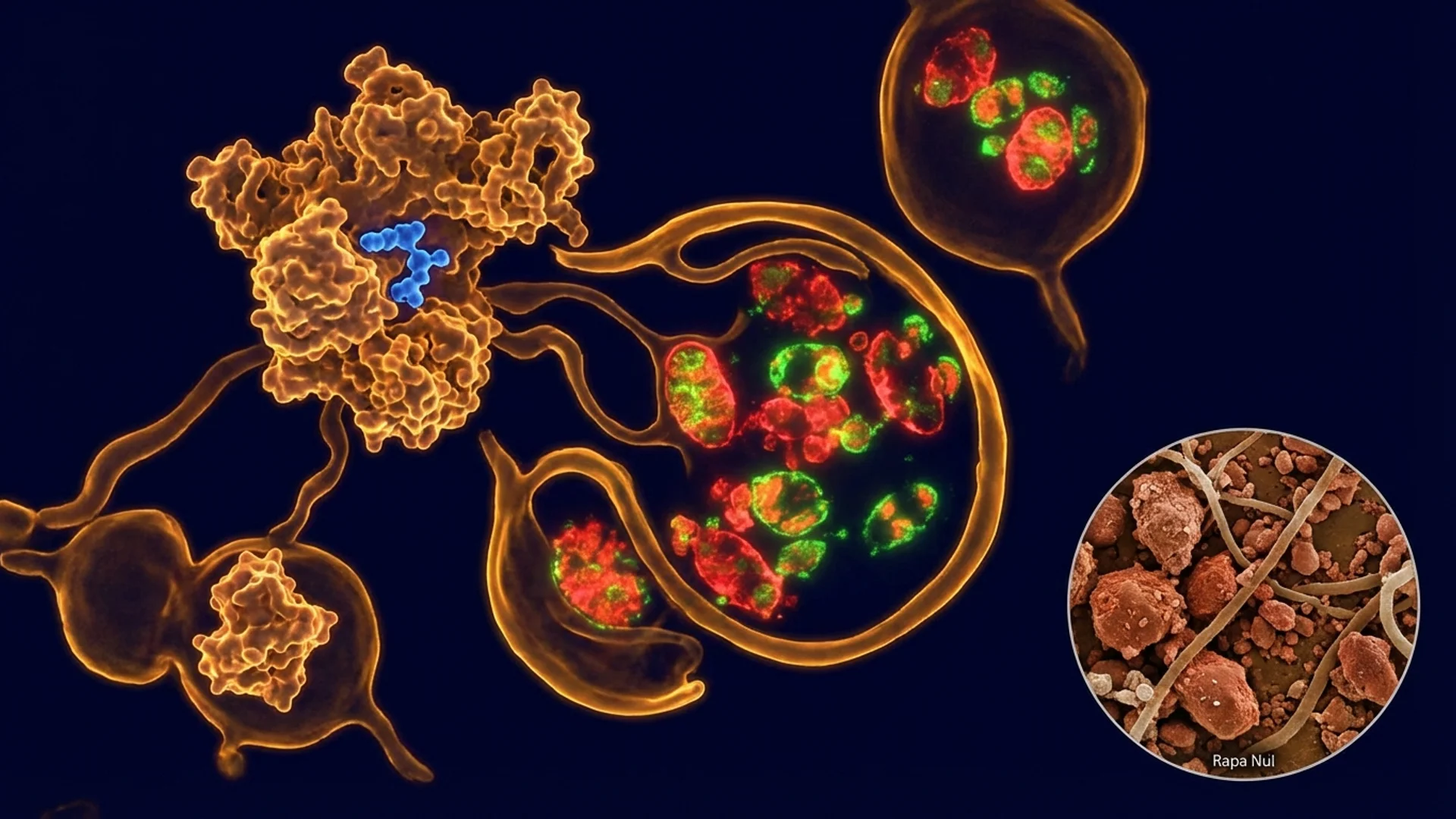
Rapamycin
mTOR inhibition for lifespan extension — the most replicated result in aging research.
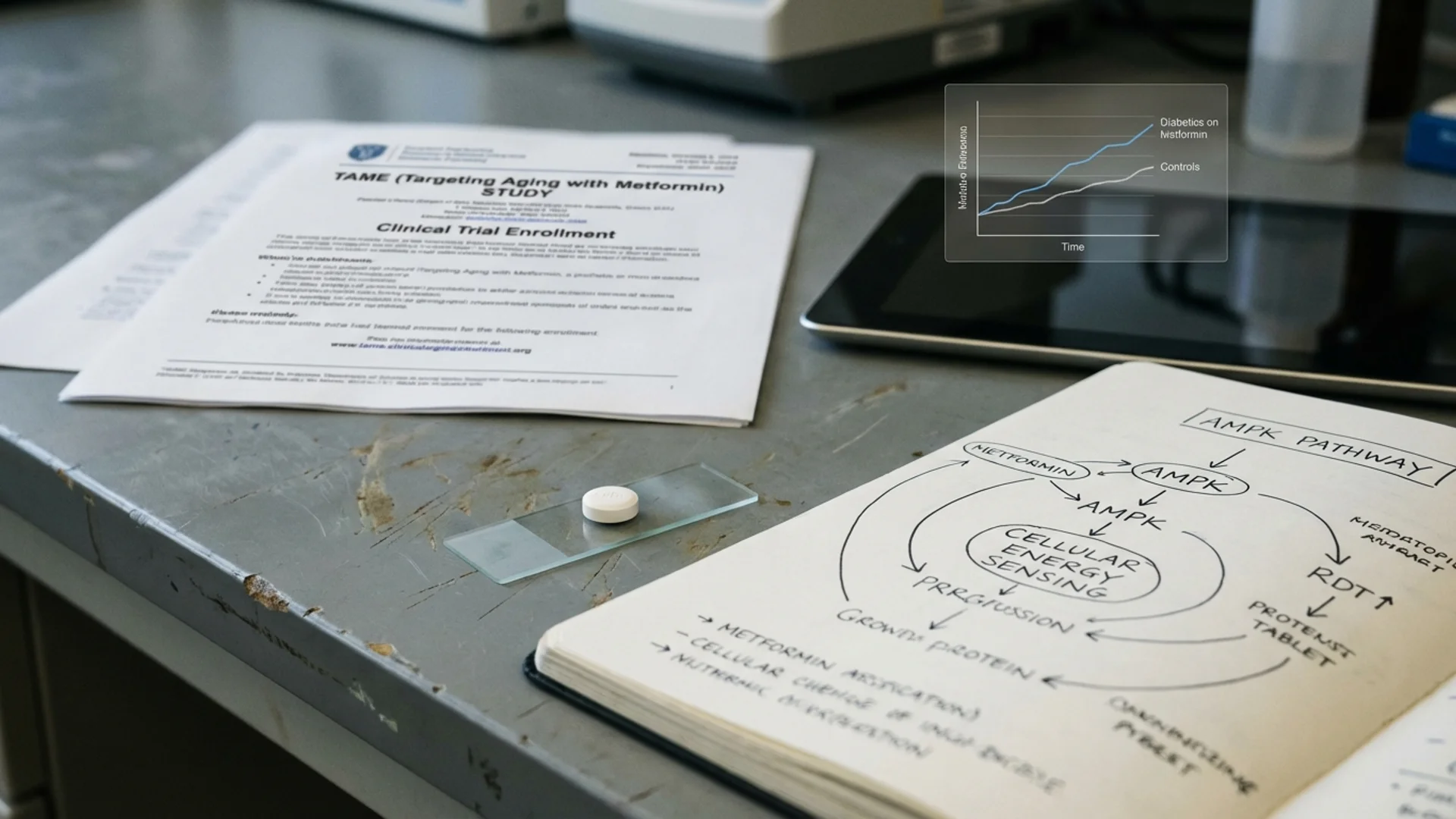
Metformin
AMPK activation and the TAME trial — diabetes drug as longevity intervention.
Hormone Optimization
Testosterone, thyroid, growth hormone, and estrogen optimization for healthspan.
Mitochondrial Health
Mitochondrial dysfunction, biogenesis, and strategies for cellular energy.
Sleep Science
Sleep architecture, circadian biology, and evidence-based optimization.
Cold & Heat Exposure
Cryotherapy, sauna, and hormetic stressors for resilience and longevity.
Biological Age Testing
Epigenetic clocks, telomere testing, and tracking your rate of aging.
Free Guide
The Longevity Self-Assessment
Download the complete physician's guide. Evidence-based, no hype.
All Articles
49 articles
Chronic Fatigue Syndrome: A Physician's Complete Guide
A physician's complete guide to chronic fatigue syndrome. Mitochondrial dysfunction, immune dysregulation, diagnostic criteria, and the stepwise treatment approach we use at Klinik St. Georg.

Organic Acids Test (OAT): What It Reveals
Complete guide to the Organic Acids Test. What the 70+ markers mean, what OAT reveals about mitochondrial function, neurotransmitters, and gut health, and when to order it.

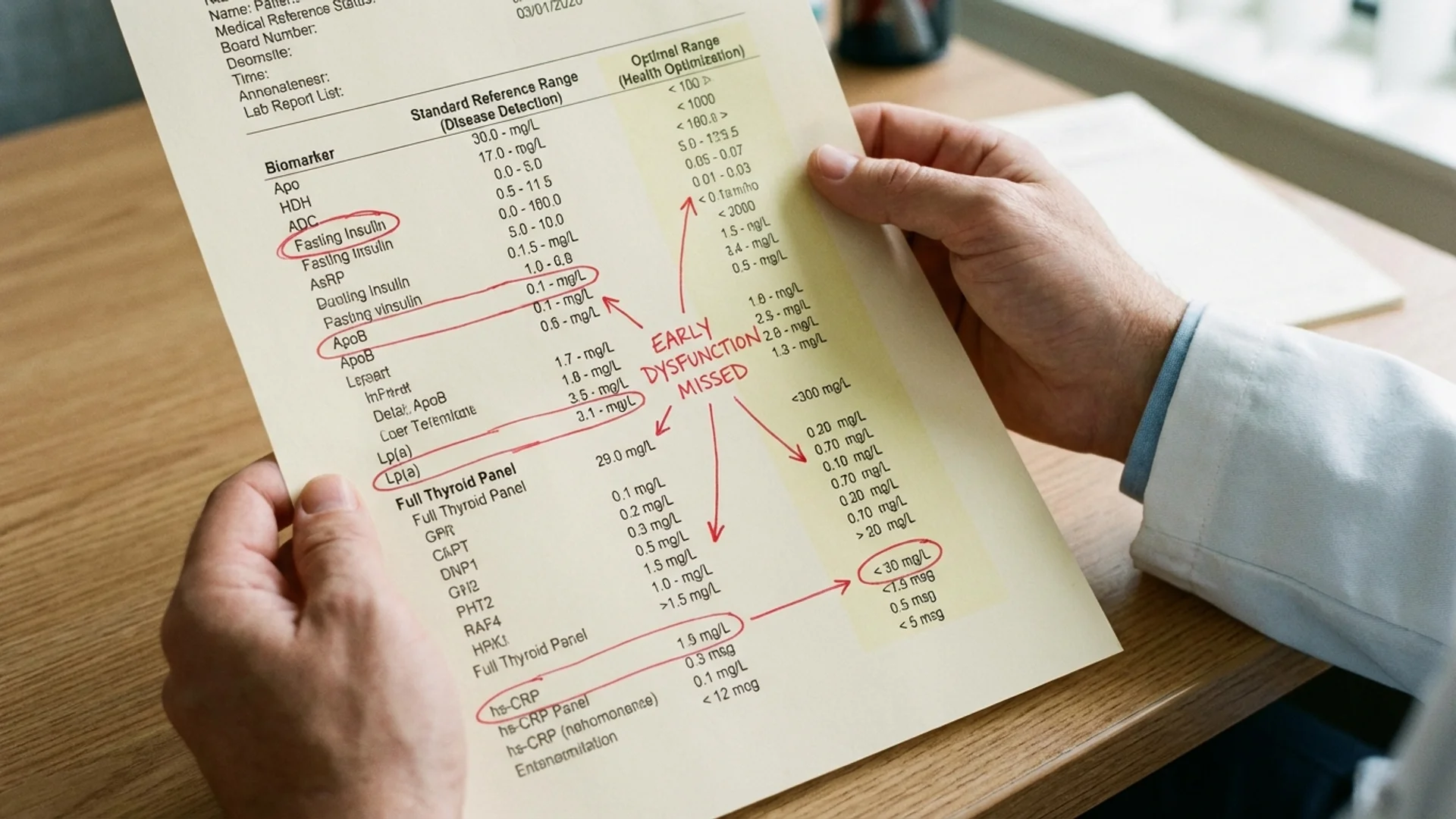
Optimal vs Normal Lab Ranges: Why Your Doctor Says You're Fine
Why standard lab reference ranges miss early disease. Optimal ranges for TSH, ferritin, vitamin D, B12, fasting insulin, hsCRP, and why functional medicine testing matters.
Autophagy: How Your Body Recycles Damaged Cells
How to activate autophagy through fasting, exercise, and targeted interventions. The science of cellular self-cleaning, its role in aging, and what actually works.
Cold Showers vs. Ice Baths: What Brown Fat Research Actually Shows
Physician analysis of cold showers versus ice baths for brown fat activation, fat loss, and metabolic health. Temperatures, durations, and what the thermogenesis data says.
Contrast Therapy Protocol: Should You Sauna or Cold Plunge First?
Physician-guided contrast therapy protocol combining sauna and cold plunge. Optimal order, timing, temperatures, and what the cardiovascular evidence shows.
How to Increase Deep Sleep Naturally: A Physician's Protocol
Evidence-based protocol to increase deep sleep and slow-wave sleep. Temperature, light, exercise timing, supplements, and what actually works according to sleep research.
Fisetin: The Senolytic Flavonoid You Should Know About
Fisetin senolytic dosing, Mayo Clinic research, mechanism of action, combination with quercetin, and honest evidence grading from a physician who uses senolytics in clinical practice.
Intermittent Fasting for Longevity: What the Evidence Supports
Evidence-based review of intermittent fasting for longevity. Autophagy activation, metabolic health, biological age, and what I recommend in clinical practice.

Metformin Dosage for Longevity: What Non-Diabetics Need to Know
Evidence-based metformin dosing for anti-aging in non-diabetics. The TAME trial, MILES study dosages, titration protocols, and what physicians actually prescribe off-label.
Metformin Side Effects for Anti-Aging Users: What to Watch For
Complete guide to metformin side effects in non-diabetics using it for longevity. B12 depletion, GI issues, exercise blunting, muscle loss risk, and mitigation strategies.
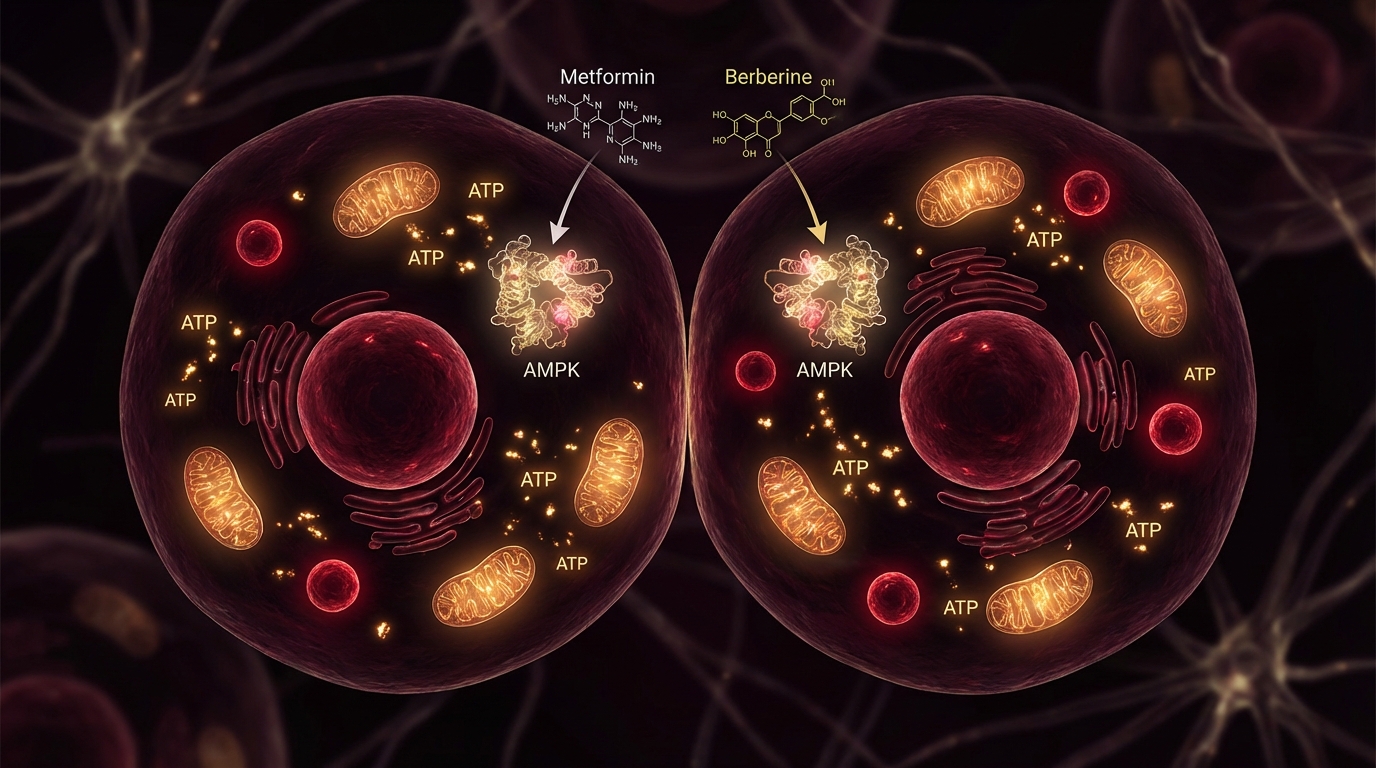
Metformin vs. Berberine: AMPK Activators Compared
Head-to-head comparison of metformin and berberine for longevity, AMPK activation, blood sugar, and exercise compatibility. Evidence, dosing, and which to choose.
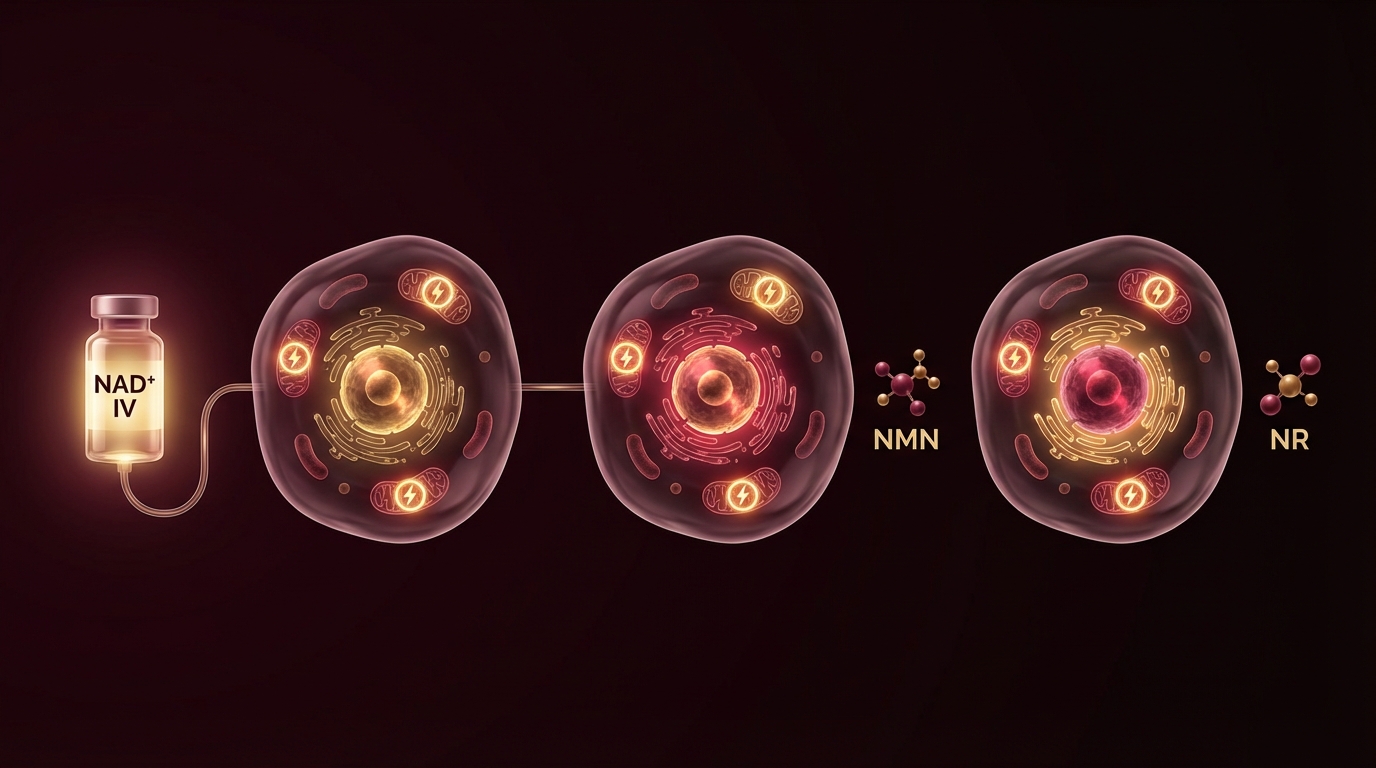
NAD+ IV vs NMN vs NR: Which NAD Precursor Is Best?
NAD+ IV, NMN, and NR compared by a physician. Bioavailability, evidence, cost, and who benefits from which approach based on clinical experience.
Rapamycin vs Metformin for Longevity: A Head-to-Head Comparison
A physician's honest comparison of rapamycin and metformin for longevity. mTOR inhibition vs AMPK activation, evidence quality, dosing, and who should use which.
How Often Should You Sauna? What the Longevity Evidence Shows
Physician analysis of sauna frequency for longevity based on the Finnish cohort studies. How often, how long, what temperature, and who should avoid it.
How Much Deep Sleep and REM Do You Need? Sleep Architecture Explained
Physician guide to sleep stages, deep sleep and REM targets by age, and what your sleep tracker data actually means for longevity and cognitive health.
Best Supplements for Deep Sleep: Evidence Ranked
Physician-ranked guide to sleep supplements. Magnesium glycinate, glycine, apigenin, L-theanine, and ashwagandha compared by evidence quality for deep sleep enhancement.
VO2 Max: The Strongest Predictor of How Long You Live
VO2 max predicts all-cause mortality more powerfully than smoking, diabetes, or hypertension. How to test it, what your number means, and how to improve it.
Zone 2 Training: The Foundation of Cardiovascular Longevity
Why Zone 2 cardio is the single most important exercise modality for longevity. Mitochondrial biogenesis, fat oxidation, VO2 max, and practical programming.
Testosterone After 40: What Every Man Should Know
Evidence-based guide to testosterone optimization after 40. Testing, natural decline, the optimization ladder from lifestyle to TRT, risks, benefits, and monitoring — from a physician who treats it daily.
Photobiomodulation for Brain Fog: Mitochondrial Rescue
How photobiomodulation targets mitochondrial dysfunction to clear brain fog. Mechanism, clinical evidence, and practical application for chronic illness patients.
DSIP Dosage and Protocol for Sleep
Evidence-based DSIP dosing guide for sleep. Subcutaneous protocols, timing, cycling, and realistic expectations from Dr. Julian Douwes.

DSIP vs Melatonin: Which Sleep Peptide?
DSIP vs melatonin comparison by Dr. Julian Douwes. Sleep architecture modulation vs circadian timing — mechanisms, evidence levels, and when to use each.
Epithalon Dosage: Telomere Protocol and Cycling
Evidence-based Epithalon dosing guide. Injection protocols, 10-20 day cycling, annual scheduling, and telomere monitoring from Dr. Julian Douwes.
Epithalon vs NMN: Anti-Aging Mechanisms Compared
Epithalon vs NMN comparison by Dr. Julian Douwes. Telomere lengthening vs NAD+ replenishment — different aging hallmarks, different evidence, and when to use each.
Berberine vs Metformin: AMPK Activation Compared
Head-to-head comparison of berberine and metformin for glucose control, lipids, and longevity. Both activate AMPK — but how do they really compare?
CoQ10: Ubiquinol vs Ubiquinone — What Actually Matters
Evidence-based guide to CoQ10 supplementation. Ubiquinol vs ubiquinone, absorption differences, statin interactions, mitochondrial function, and what I recommend in clinical practice.
CoQ10 for Statin Users: Why Your Cholesterol Medication Depletes CoQ10
Physician guide to CoQ10 depletion from statins. Why it happens, symptoms of statin-induced CoQ10 deficiency, optimal dosing with ubiquinol, and what the evidence shows.

Magnesium Glycinate vs. L-Threonate: Which Form for Sleep, Anxiety, and Brain Health?
Physician comparison of magnesium glycinate vs magnesium L-threonate. Which form for sleep, which for cognition, absorption differences, dosing, and evidence quality.

When to Take Magnesium: Morning vs. Night, With or Without Food
Physician guide to magnesium supplement timing. When to take glycinate, threonate, citrate, and other forms for maximum absorption and effect. Morning vs night, food interactions.
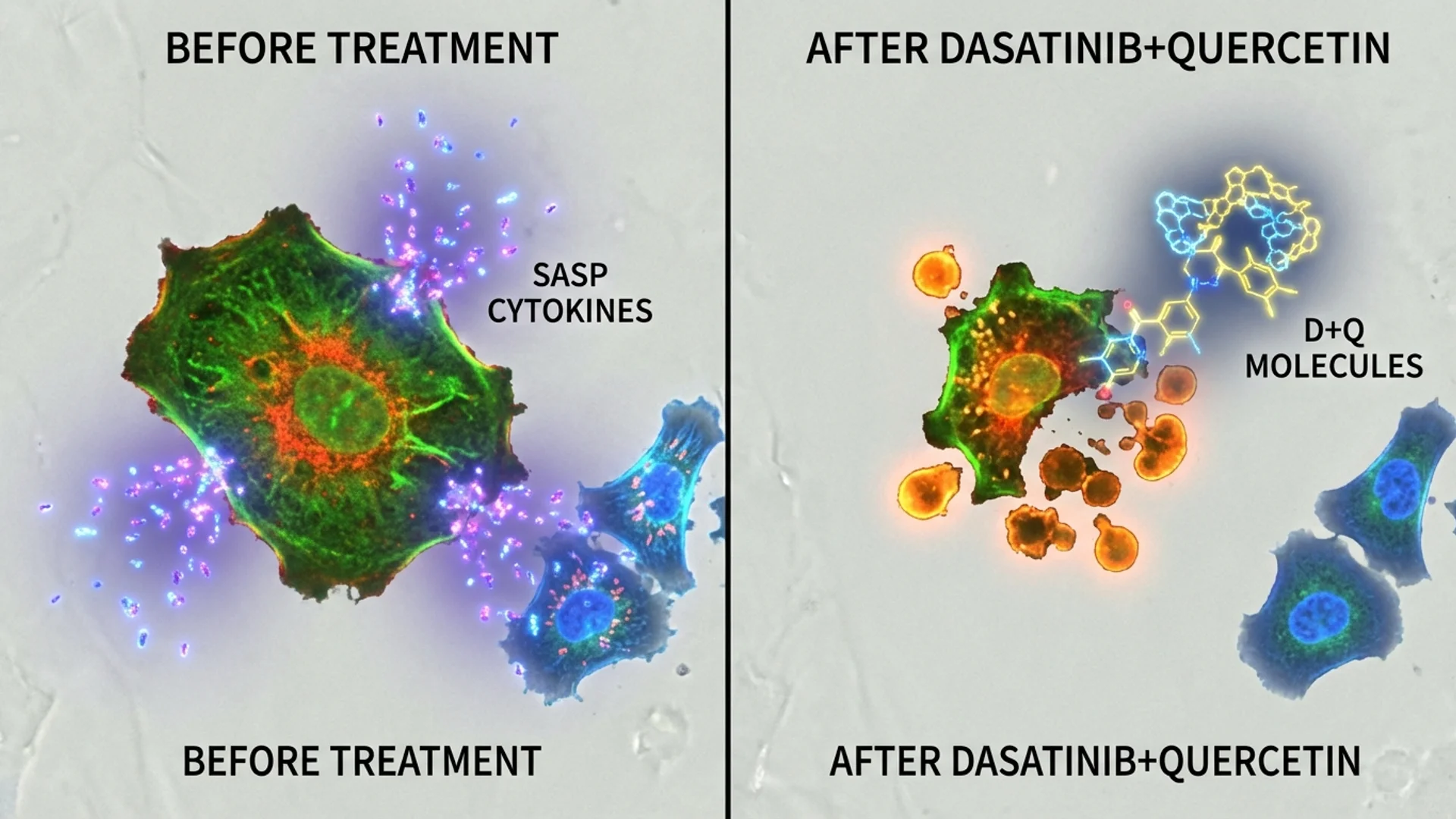
Quercetin as a Senolytic: Protocol, Dosage, and What the Research Shows
Physician guide to quercetin senolytic protocols. Quercetin + dasatinib evidence, quercetin + fisetin alternatives, dosing schedules, and the science of clearing senescent cells.
Blood Panels Decoded: Beyond the Standard CBC
What your standard blood work measures, what it misses, and which additional markers provide the most clinical value. By Dr. Julian Douwes.
Biological Age Testing
Epigenetic clocks, pace of aging, and how to measure how fast you are actually aging. What the tests mean and their limitations.
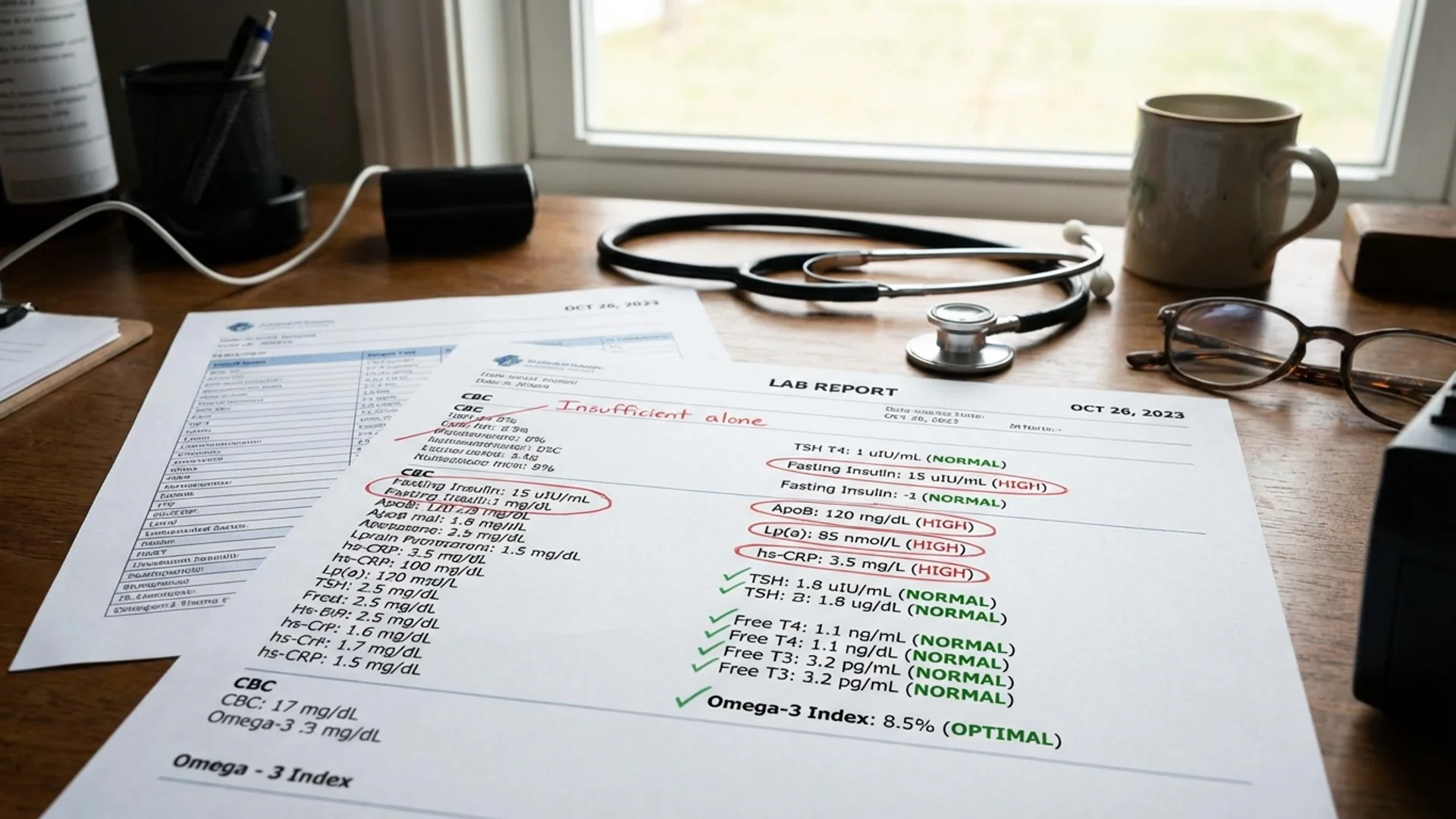
The Longevity Blood Panel
What blood markers to test for longevity optimization, why standard panels are insufficient, and how to interpret results in context.

Cold and Heat Exposure for Longevity
Cold plunge and sauna protocols for healthspan. What the evidence shows about deliberate temperature stress and aging.

Hormone Optimization for Men
Testosterone, DHEA, thyroid, and growth hormone in aging men. Evidence-based approach to male hormonal health and longevity.

Hormone Optimization for Women
Estrogen, progesterone, thyroid, and DHEA in aging women. Evidence-based approach to female hormonal health across perimenopause and beyond.

IHHT: Intermittent Hypoxia-Hyperoxia Training
How IHHT simulates altitude training to improve mitochondrial function. Evidence, protocols, and clinical applications.
Metformin for Longevity
Can a diabetes drug slow aging? The TAME trial, mechanistic rationale, and honest assessment of metformin as a longevity intervention.
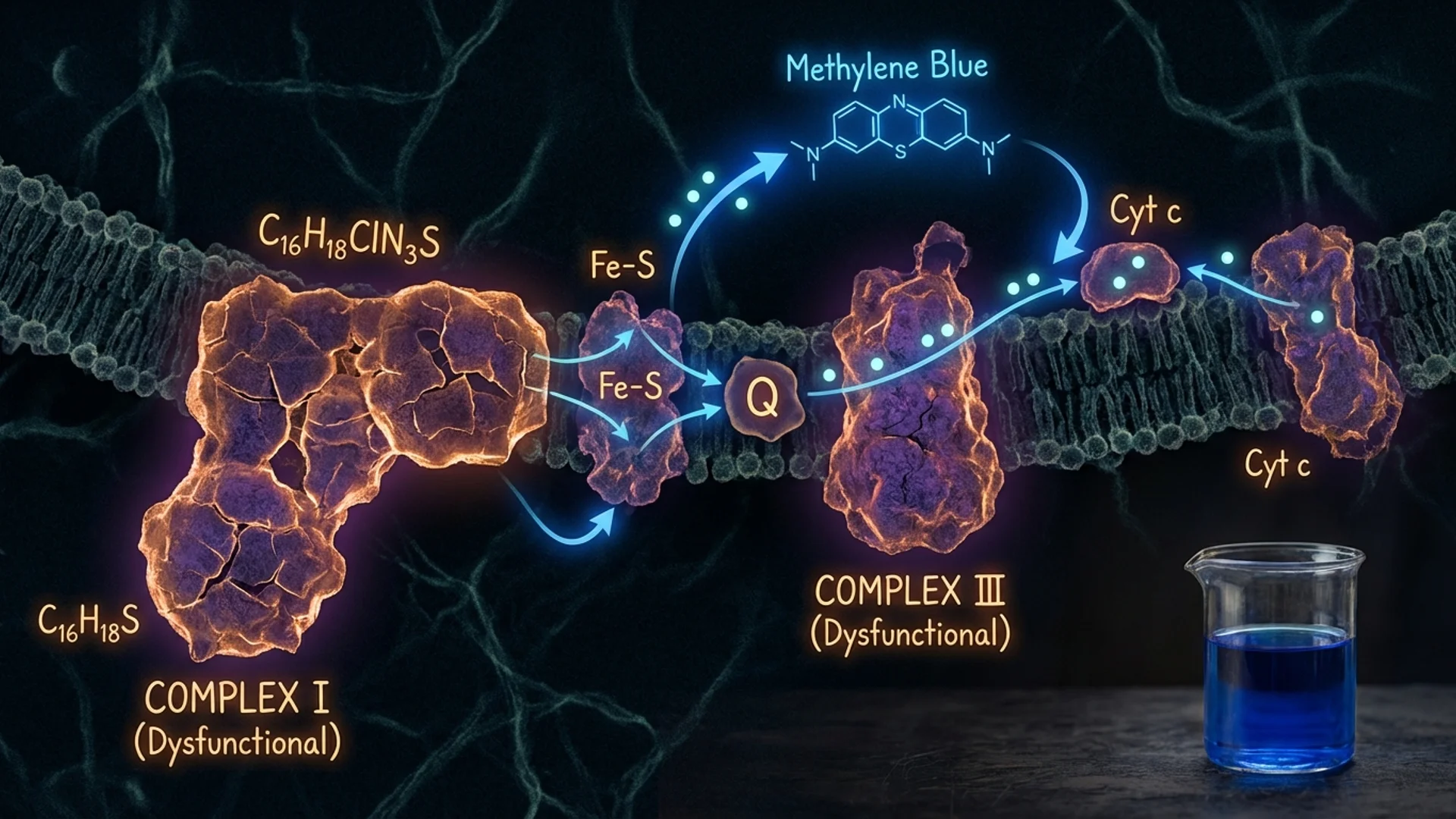
Methylene Blue: Mitochondrial and Antimicrobial
What methylene blue does at the mitochondrial level, its antimicrobial properties, and a conservative assessment of its longevity potential.
Mitochondrial Medicine: The Energy Crisis
Why mitochondrial dysfunction underlies fatigue, cognitive decline, and aging. Testing, treatment, and what actually improves mitochondrial function.
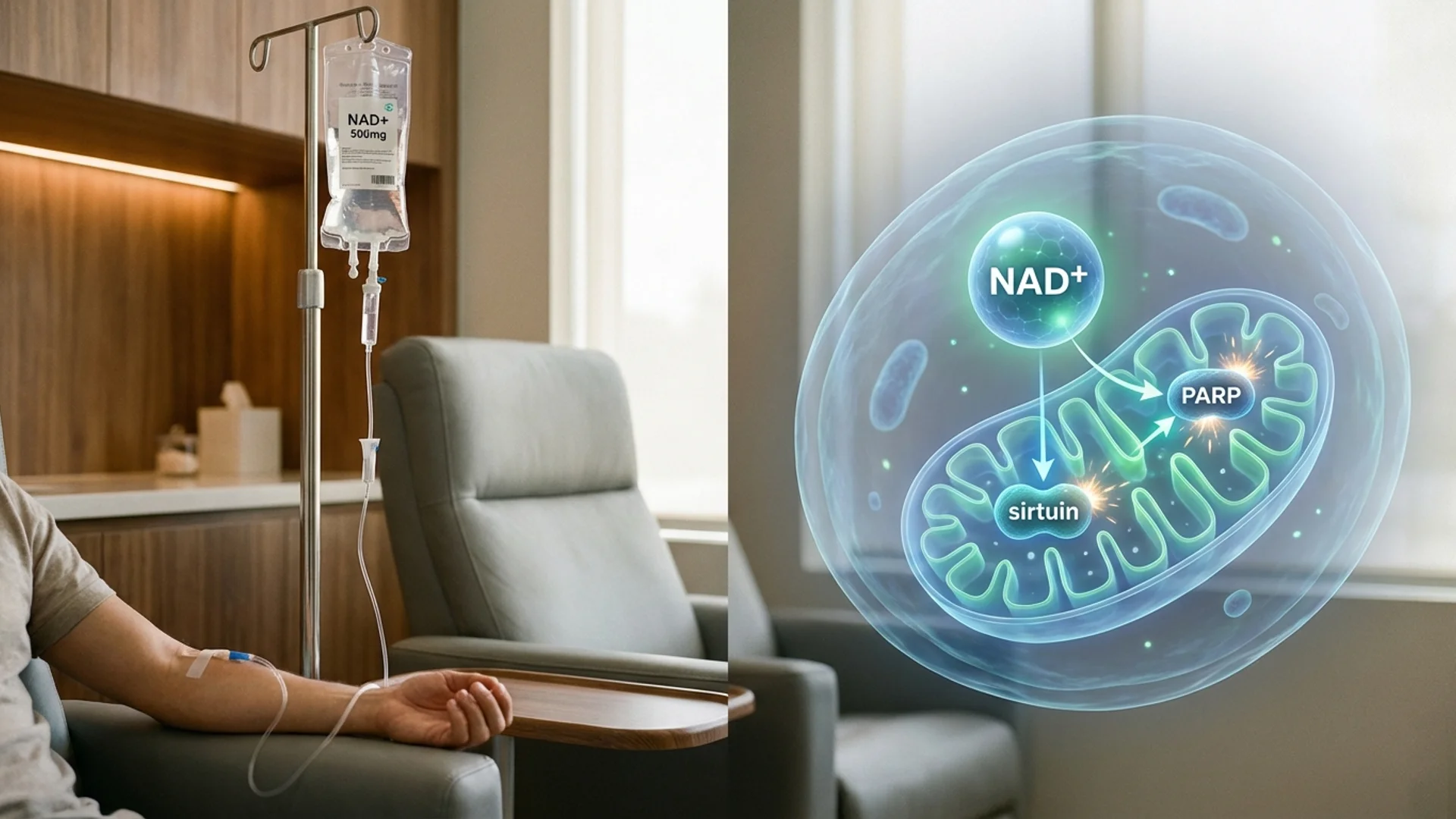
NAD+ IV Therapy: Cellular Energy and Aging
How NAD+ IV therapy supports mitochondrial function and cellular repair. Evidence, clinical experience, and what patients should know.
Rapamycin and mTOR: Longevity's Most Debated Drug
How rapamycin inhibits mTOR to potentially slow aging. Evidence from animal studies, emerging human data, risks, and honest assessment.
Senolytics: Clearing Senescent Cells
How senolytic therapies target zombie cells that drive aging. Dasatinib, quercetin, fisetin -- evidence, protocols, and honest limitations.
Sleep Architecture and Longevity
How sleep stages affect aging, recovery, and healthspan. Optimization strategies grounded in evidence and clinical experience.

Building Your Longevity Stack
Evidence-tiered approach to longevity supplements. What works, what might work, and what to skip -- from a physician's perspective.
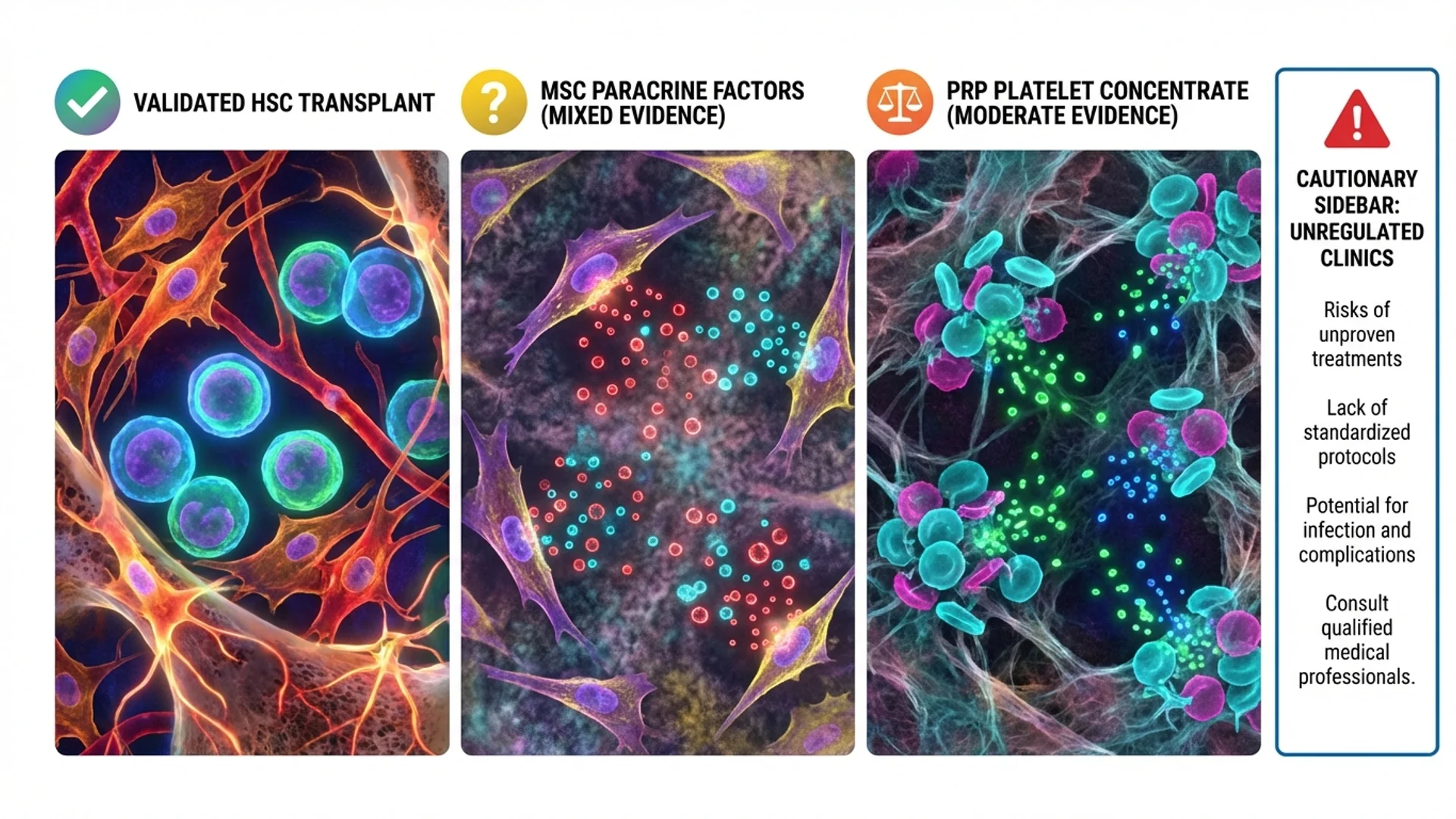
Stem Cell Therapy: What Works, What Doesn't
An honest assessment of stem cell therapy for longevity and regeneration. Separating science from marketing in the stem cell industry.
Telomere Health: Length, Telomerase, Epithalon
What telomere length means for aging, whether you can influence it, and the honest truth about telomerase activators and Epithalon.

Sleep Optimization Protocol
Evidence-based strategies for improving sleep quality -- environment, timing, supplements, and habits. By Dr. Julian Douwes.
Complete Guide
Longevity Medicine: Beyond Anti-Aging
In-depth reference by Dr. Julian Douwes
Longevity Medicine: Beyond Anti-Aging
There is a version of longevity medicine that exists primarily on social media — a world of ice baths, supplement hauls, and promises of living to 150. Then there is the version that exists in clinical practice, which is quieter, more nuanced, and far more interesting.
I want to talk about the second version.
Longevity medicine, as I practice it, is not about chasing immortality or reversing the clock. It is about understanding why we age, identifying which of those processes are modifiable, and intervening where the evidence supports doing so. The goal is not to add years to life at any cost. The goal is to extend the period of life during which a person functions well — physically, cognitively, and metabolically. This is what we mean by healthspan.
What Longevity Medicine Actually Is
The field has matured considerably over the past decade. What was once a fringe pursuit dominated by anti-aging clinics selling growth hormone has evolved into a discipline grounded in molecular biology, genomics, and metabolic science.
At its core, longevity medicine asks a deceptively simple question: can we slow, halt, or selectively reverse the biological processes that drive age-related decline?
The honest answer is that we can influence some of these processes meaningfully, others modestly, and some not yet at all. The nuance matters, because patients who walk into my office often arrive with expectations shaped by headlines rather than data.
Here is what I tell my patients on the first visit: longevity medicine is not a single intervention. It is a framework. It integrates diagnostics, lifestyle modification, targeted supplementation, hormonal optimization, and — in selected cases — pharmacological or procedural interventions. The most effective longevity programs I have designed are not the ones with the most exotic therapies. They are the ones built on a thorough understanding of each patient’s individual biology.
The Hallmarks of Aging
In 2013, a landmark paper in Cell identified nine hallmarks of aging [1]. These have since been expanded to 12, and they provide the intellectual scaffolding for modern longevity medicine. Understanding them is not academic. Each hallmark represents a potential intervention point.
1. Genomic Instability
DNA damage accumulates over a lifetime. Our repair mechanisms are remarkably effective, but they are not perfect. Over decades, unrepaired damage contributes to cellular dysfunction and cancer risk. What we can do: reduce exposure to known genotoxic agents, support DNA repair pathways through adequate NAD+ levels, and monitor for early signs of genomic instability through advanced diagnostics.
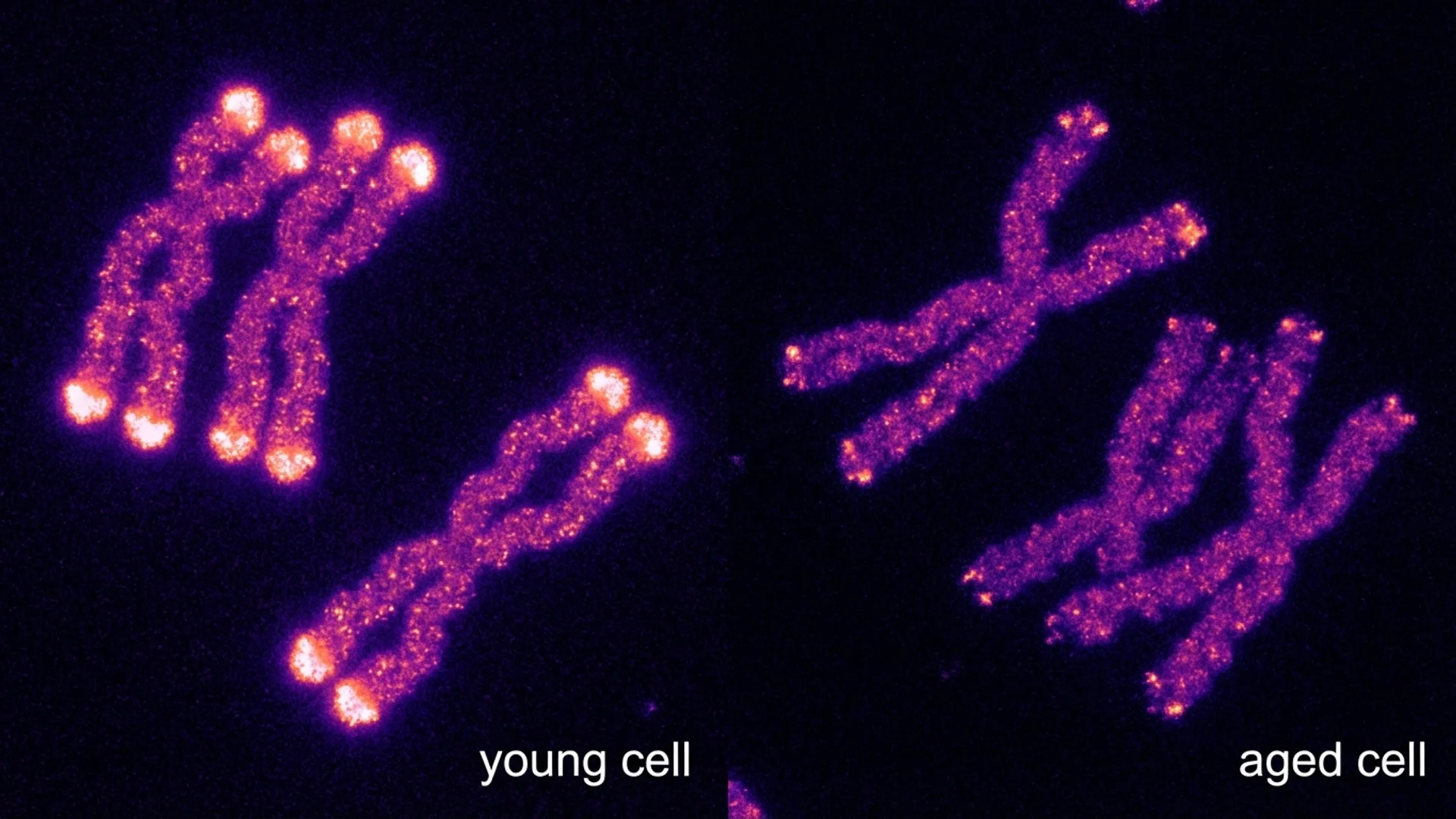
2. Telomere Attrition
Telomeres — the protective caps on chromosomes — shorten with each cell division. When they become critically short, cells enter senescence or die. Telomere length is measurable and correlates with biological age, though the relationship is not as straightforward as early reporting suggested. I discuss this in detail in my article on telomere health.
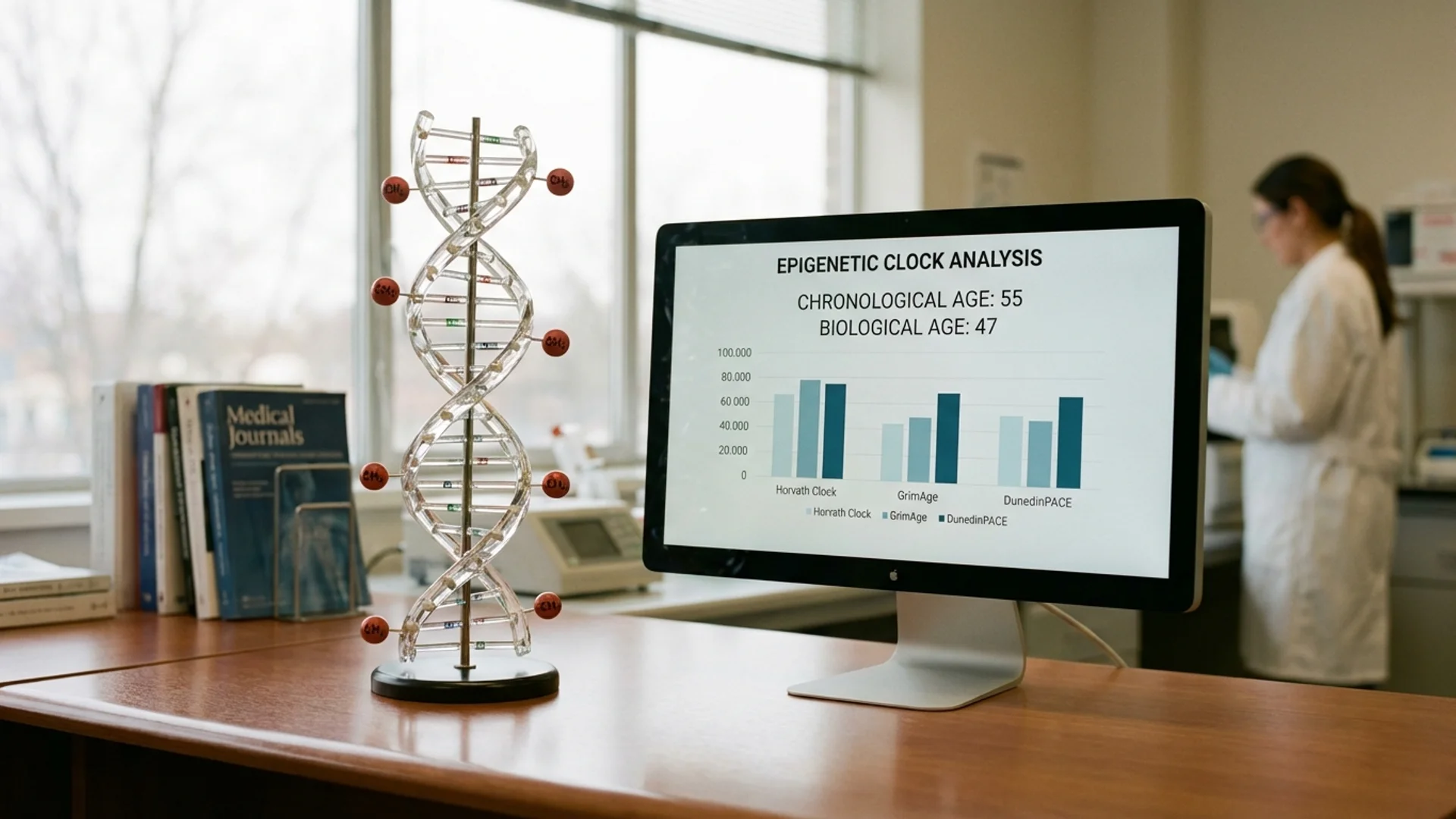
3. Epigenetic Alterations
Gene expression patterns change with age, and not always favorably. Epigenetic clocks, pioneered by Steve Horvath and others, can now estimate biological age with remarkable precision. These clocks have become one of my primary tools for assessing where a patient stands and whether interventions are working. More on this in biological age testing.
4. Loss of Proteostasis
The cellular machinery responsible for protein folding and degradation deteriorates with age. Misfolded proteins accumulate, contributing to neurodegenerative diseases and general cellular dysfunction. Autophagy — the cell’s recycling system — declines. Fasting, exercise, and certain pharmacological agents (rapamycin among them) can upregulate autophagy, though the optimal protocols remain an area of active research.
5. Deregulated Nutrient Sensing
Four key nutrient-sensing pathways — mTOR, AMPK, sirtuins, and insulin/IGF-1 signaling — become dysregulated with age. This is the mechanistic basis for why caloric restriction and fasting extend lifespan in animal models. It is also why interventions like rapamycin and metformin have generated so much interest. I cover both in dedicated articles.
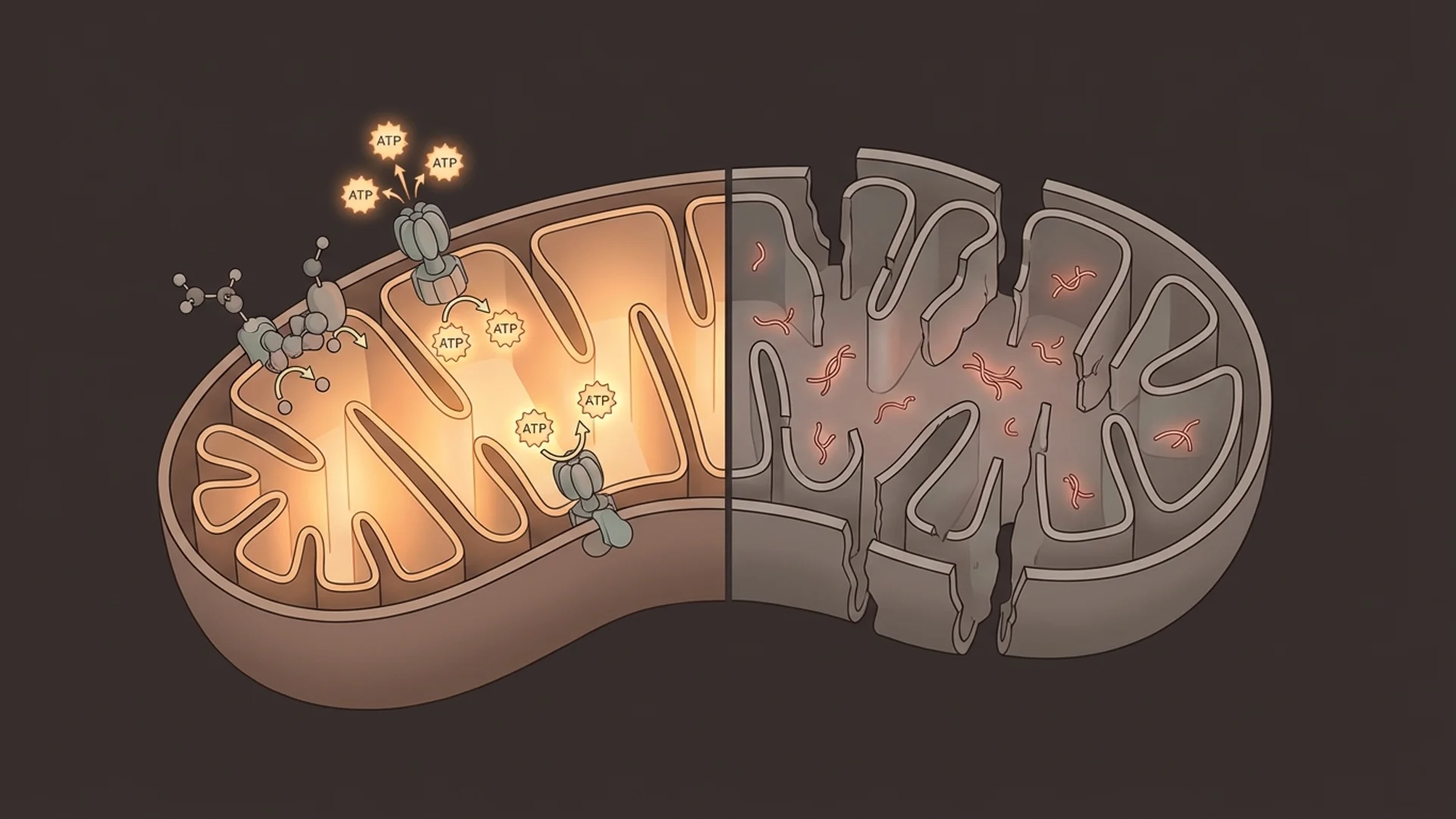
6. Mitochondrial Dysfunction
Mitochondria produce the energy that drives virtually every cellular process. As they age, they become less efficient, produce more reactive oxygen species, and contribute to systemic inflammation. In my clinical experience, mitochondrial dysfunction is one of the most underdiagnosed contributors to fatigue, cognitive decline, and metabolic disease. It is also one of the most treatable. See my detailed discussion on mitochondrial medicine.
7. Cellular Senescence
Senescent cells — sometimes called “zombie cells” — have stopped dividing but refuse to die. They accumulate with age and secrete inflammatory factors that damage neighboring tissue. The senolytic hypothesis — that selectively clearing these cells could slow aging — is one of the most exciting areas in the field. The evidence, primarily from animal models, is compelling. Human data is emerging. I discuss this honestly in senolytics.
8. Stem Cell Exhaustion
Our regenerative capacity declines with age as stem cell populations shrink and lose function. Stem cell therapy is one of the most overhyped areas in medicine, and also one of the most genuinely promising. The challenge is separating the clinics making unsupported claims from the research that may eventually transform how we treat aging. I address this in stem cell therapy.
9. Altered Intercellular Communication
Aging changes how cells communicate with each other. Chronic low-grade inflammation — sometimes called “inflammaging” — disrupts signaling throughout the body. Many longevity interventions ultimately aim to reduce this inflammatory burden through various mechanisms.
10. Disabled Macroautophagy
The decline in autophagy with age means cells accumulate damaged organelles and proteins. Supporting autophagy through fasting, exercise, and potentially pharmacological agents is a legitimate strategy, though the optimal approach varies by individual.
11. Chronic Inflammation
Inflammaging is both a hallmark and a driver of other hallmarks. It creates a feedback loop that accelerates aging across multiple systems. Identifying and addressing the sources of chronic inflammation — whether metabolic, infectious, or environmental — is foundational to any serious longevity program.
12. Dysbiosis
The gut microbiome changes with age, and these changes appear to influence systemic aging processes. This is an area where our understanding is still developing rapidly, but the evidence connecting gut health to immune function, inflammation, and even cognitive decline is increasingly difficult to ignore.
A Physician’s Perspective: What Actually Works
After treating patients with longevity-focused programs for over a decade, I want to be transparent about what I have seen work and what I remain uncertain about.
The Foundations (Strong Evidence, High Impact)
The interventions with the strongest evidence and the greatest impact on healthspan are, perhaps disappointingly, not exotic:
Exercise remains the single most effective longevity intervention we have. The data is overwhelming. Both cardiovascular training and resistance training independently reduce all-cause mortality. The dose-response curve suggests that even modest increases in physical activity yield significant benefits, with diminishing returns at very high volumes [2].
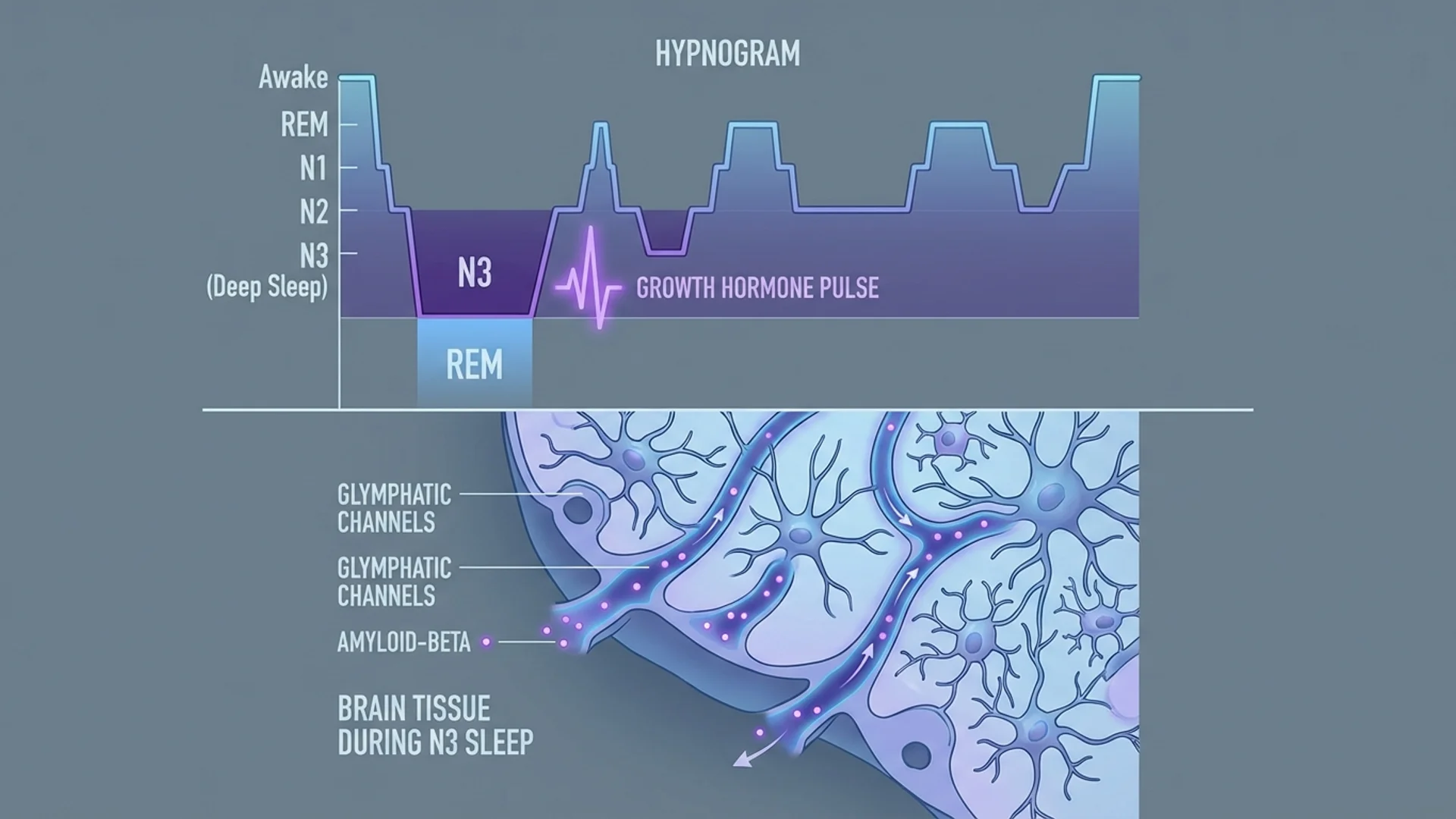
Sleep optimization is second. Poor sleep accelerates every hallmark of aging I have described. Seven to nine hours of quality sleep, with adequate time in deep and REM stages, is non-negotiable. I discuss sleep architecture and optimization strategies in a dedicated article.
Metabolic health — maintaining insulin sensitivity, healthy body composition, and stable blood glucose — underpins everything else. You cannot supplement your way out of metabolic dysfunction.
Nutrition matters, though the specifics are more contested than most people realize. What I tell my patients: eat whole foods, adequate protein (1.2-1.6 g/kg for most adults), sufficient fiber, and minimize ultra-processed food. The specific dietary framework matters less than consistency.
The Second Tier (Moderate Evidence, Meaningful Impact)
Hormonal optimization can be transformative for patients with documented deficiencies. Testosterone replacement in men with genuine hypogonadism, thyroid optimization, DHEA support — these are evidence-based interventions when applied appropriately. The key word is “optimization,” not “maximization.” I cover men’s and women’s hormonal health in separate articles.
NAD+ support, whether through IV infusion or oral precursors, has a strong mechanistic rationale and growing clinical evidence. In my practice, I have observed consistent improvements in energy, cognitive clarity, and exercise recovery. The controlled trial data in humans is still maturing. See NAD+ IV therapy.
Targeted supplementation — vitamin D, omega-3 fatty acids, magnesium, creatine — has reasonable evidence supporting its use in specific contexts. I discuss evidence tiers for common longevity supplements in building your longevity stack.
The Frontier (Emerging Evidence, Promising but Uncertain)
Rapamycin at low, intermittent doses has remarkable preclinical data for lifespan extension. Human longevity data is limited. I use it selectively and discuss the evidence and risks in rapamycin and mTOR.
Senolytics are potentially transformative. The animal data is striking. Human trials are underway. I want to be direct: we do not yet know the optimal dosing, timing, or patient selection for senolytic therapy in humans. This deserves continued research.
Metformin for longevity in non-diabetic individuals is the subject of the TAME trial, one of the most important longevity studies currently running. The mechanistic rationale is sound. The epidemiological data is suggestive. The definitive answer is not yet available.
Peptide therapies, stem cell treatments, and methylene blue each have intriguing data but require careful, honest evaluation. I address each in dedicated articles.
How I Approach Longevity in Practice
When a patient comes to me for longevity optimization, the process begins with comprehensive diagnostics. I am not interested in guessing. I want data.
A thorough longevity assessment includes:
- Advanced blood work beyond standard panels — inflammatory markers, metabolic markers, hormonal profiles, micronutrient status, and organ function. See the longevity blood panel.
- Biological age testing using epigenetic clocks and other validated biomarkers.
- Mitochondrial function assessment through organic acid testing and other functional markers.
- Body composition analysis with attention to visceral fat, muscle mass, and bone density.
- Cardiovascular risk assessment including advanced lipid panels and, where indicated, coronary calcium scoring.
- Cognitive baseline testing for patients concerned about neurodegeneration.
Based on this data, I design individualized programs. No two patients receive the same protocol, because no two patients have the same biology.
What This Series Covers
The articles in this longevity series represent my attempt to give patients and physicians an honest assessment of where the field stands. For each topic, I distinguish between what the evidence shows, what clinical observation suggests, and what remains uncertain.
I do not promise miracles. I do not use the word “cure.” What I offer is a physician’s perspective, grounded in both published research and years of clinical practice, on how to age better.
The articles that follow cover specific interventions, diagnostics, and protocols in detail. Start with whichever topic is most relevant to your situation, or read them sequentially for a comprehensive understanding of modern longevity medicine.
References
- Lopez-Otin C, et al. The Hallmarks of Aging. Cell. 2013;153(6):1194-1217.
- Ekelund U, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality. BMJ. 2019;366:l4570.
This content is educational and does not constitute medical advice. Longevity interventions should be discussed with a qualified physician who can assess your individual health status and risk factors.