Diagnostics
Lab testing, blood panels, immune profiling, and functional medicine diagnostics. What your doctor isn't testing — and why it matters.
By topic.
Blood Panels
Comprehensive blood work beyond standard panels — what to order and how to interpret results.
Immune Testing
Lymphocyte subsets, NK cell function, cytokine panels, and functional immune profiling.
Hormone Testing
Comprehensive hormone panels — thyroid, sex hormones, adrenal, growth hormone axis.
Lyme Disease Testing
ELISA, Western Blot, ELISpot, and advanced Lyme diagnostics — why standard tests miss chronic Lyme.
Microbiome Testing
Stool analysis, SIBO testing, and gut microbiome profiling for targeted treatment.
Heavy Metal Testing
Provoked and unprovoked heavy metal testing, chelation considerations, and environmental toxin assessment.
Functional Medicine Labs
Organic acids, methylation panels, oxidative stress markers, and specialty diagnostics.
The Complete Lab Test Reference Guide
Download the complete physician's guide. Evidence-based, no hype.
Articles
31 articles Supplements
Supplements Alpha-Lipoic Acid: Neuropathy, Heavy Metal Detox, and Mitochondrial Repair
Dr. Douwes reviews alpha-lipoic acid dosing, R-ALA vs racemic forms, clinical uses for neuropathy, heavy metal chelation support, and mitochondrial longevity.
 Protocols
Protocols Heavy Metal Chelation Therapy: A Physician's Clinical Protocol
Dr. Julian Douwes explains heavy metal chelation therapy — which agents to use, when to use them, how to prepare, and how to monitor safely in clinical practice.
 Diagnostics
Diagnostics Your First Consultation: What We Assess and Why
What happens during your first consultation at Klinik St. Georg. The labs we order, the intake process, how we build your treatment plan, and realistic timelines.
 Diagnostics
Diagnostics Western Blot vs ELISA: Lyme Testing Accuracy Compared
Head-to-head comparison of Western Blot and ELISA for Lyme disease. Sensitivity at each stage, what the bands mean, the two-tier protocol, and why the system misses patients.
 Diagnostics
Diagnostics Labs Your Doctor Won't Order (But Should)
Essential functional medicine labs most doctors skip. hs-CRP, fasting insulin, homocysteine, full thyroid, ApoB, and more — what to request and why it matters.
 Diagnostics
Diagnostics Chelation Therapy Side Effects and Safety
Complete guide to chelation therapy side effects. Common reactions, serious risks, mineral depletion, monitoring requirements, and how to minimize adverse effects.
 Infectiology
Infectiology Mold Testing: Urine Mycotoxins vs ERMI vs Air Testing
Comparing mold testing methods — urine mycotoxin testing for body burden, ERMI for environmental exposure, and air sampling limitations. Which test you actually need.
 Diagnostics
Diagnostics Organic Acids Test (OAT): What It Reveals
Complete guide to the Organic Acids Test. What the 70+ markers mean, what OAT reveals about mitochondrial function, neurotransmitters, and gut health, and when to order it.
 Diagnostics
Diagnostics CD57 Test in Lyme Disease: Useful or Unreliable?
The CD57 test in Lyme disease — what it measures, Dr. Stricker's original hypothesis, conflicting study results, and how clinicians actually use it in practice.
 Diagnostics
Diagnostics iSpot Lyme T-Cell Test: A Better Way to Detect Borrelia?
How the iSpot Lyme (ELISpot) T-cell test works, its advantages over antibody testing, 84% sensitivity data, limitations, and when it adds clinical value.
 Diagnostics
Diagnostics Functional vs Conventional Lab Ranges: Why Yours Differ
Why functional medicine blood test ranges differ from conventional lab ranges. TSH, vitamin D, ferritin, fasting glucose — what 'normal' really means and why it matters.
 Diagnostics
Diagnostics GI-MAP vs Standard Stool Culture: Which Test to Choose
Comparing GI-MAP qPCR stool testing with standard stool culture. Detection rates, pathogen coverage, clinical utility, and when each test is the right choice.
 Neuromodulation
Neuromodulation Neuropsychological Testing for Brain Fog: When and Why
When to get neuropsychological testing for brain fog. What the evaluation measures, how it differs from standard neurology exams, and what the results mean for treatment.
 Supplements
Supplements Magnesium Deficiency Symptoms: The Warning Signs Most People Miss
Physician guide to magnesium deficiency symptoms including muscle cramps, insomnia, anxiety, heart palpitations, and fatigue. Testing, causes, and how to correct it.
 Diagnostics
Diagnostics Heavy Metal Testing: Blood vs Urine vs Provoked
Comparing heavy metal testing methods. When blood testing, unprovoked urine, and provoked (post-chelation) urine are appropriate, and the controversy around each.
 Diagnostics
Diagnostics Lyme Disease, Gut Dysbiosis, and Leaky Gut
How Lyme disease disrupts the gut microbiome. Antibiotic-driven dysbiosis, Borrelia's effect on intestinal permeability, the Hopkins microbiome findings, and recovery strategies.
 Diagnostics
Diagnostics Low NK Cell Function: What It Means and What to Do
Understanding low natural killer cell function in chronic illness. What NK cells do, why function drops, how to test, and evidence-based strategies to restore immune surveillance.
 Diagnostics
Diagnostics Lymphocyte Subset Panel: Reading Your Immune Profile
How to read a lymphocyte subset panel. What CD4, CD8, CD19, and CD56 cells do, what abnormal ratios mean in chronic illness, and when this test changes your treatment.
 Diagnostics
Diagnostics How to Read Your Microbiome Test Results
Practical guide to interpreting gut microbiome test results. Dysbiosis markers, keystone species, diversity metrics, and what your results actually mean for treatment.
 Diagnostics
Diagnostics Heavy Metal Toxicity Symptoms by Metal Type
How mercury, lead, arsenic, cadmium, and aluminum affect the body differently. Symptom profiles by metal type, why they overlap with chronic illness, and when to test.
 Diagnostics
Diagnostics Lyme Disease False Negatives: Why Standard Tests Miss Chronic Lyme
Why Lyme disease tests come back negative in patients with active infection. ELISA sensitivity gaps, antibody window, seronegative Lyme, and what to do when tests miss.
 Diagnostics
Diagnostics Optimal vs Normal Lab Ranges: Why Your Doctor Says You're Fine
Why standard lab reference ranges miss early disease. Optimal ranges for TSH, ferritin, vitamin D, B12, fasting insulin, hsCRP, and why functional medicine testing matters.
 Diagnostics
Diagnostics Lyme Testing: Why Standard ELISA Fails
Why standard Lyme disease tests miss infections, and which advanced tests provide accurate results. ELISpot, CD57, and beyond.
 Diagnostics
Diagnostics Microbiome Testing: Stool Analysis Interpreted
What microbiome stool tests measure, how to interpret results, and which tests provide actionable clinical information. By Dr. Julian Douwes.
 Longevity
Longevity The Longevity Blood Panel
What blood markers to test for longevity optimization, why standard panels are insufficient, and how to interpret results in context.
 Diagnostics
Diagnostics Heavy Metal Testing and Toxicology Screening
How to test for heavy metals accurately, what the results mean, and when provocation testing is warranted. By Dr. Julian Douwes.
 Diagnostics
Diagnostics Immune Profiling: Lymphocyte Subsets and Cytokines
What immune profiling reveals about your health that standard blood work cannot. Lymphocyte subsets, NK cells, and cytokine panels explained.
 Diagnostics
Diagnostics Blood Panels Decoded: Beyond the Standard CBC
What your standard blood work measures, what it misses, and which additional markers provide the most clinical value. By Dr. Julian Douwes.
 Diagnostics
Diagnostics The Complete Thyroid Panel: What to Test and Why
TSH alone is not enough. A complete thyroid panel includes free T3, free T4, reverse T3, TPO and TG antibodies. How to interpret results and screen for Hashimoto's.
 Diagnostics
Diagnostics Functional Medicine Labs: OAT, DUTCH, GI-MAP
A clinical guide to organic acids testing, DUTCH hormone testing, and GI-MAP stool analysis -- what they measure and when to use them.
 Diagnostics
Diagnostics Hormone Panels: What to Test and When
Which hormones to test, when to test them, and how to interpret results using optimal ranges rather than just reference ranges.
Functional Diagnostics: What Your Doctor Isn't Testing
In-depth reference by Dr. Julian Douwes
Functional Diagnostics: What Your Doctor Is Not Testing
By Dr. Julian Douwes, M.D. — Chief Medical Officer, Klinik St. Georg
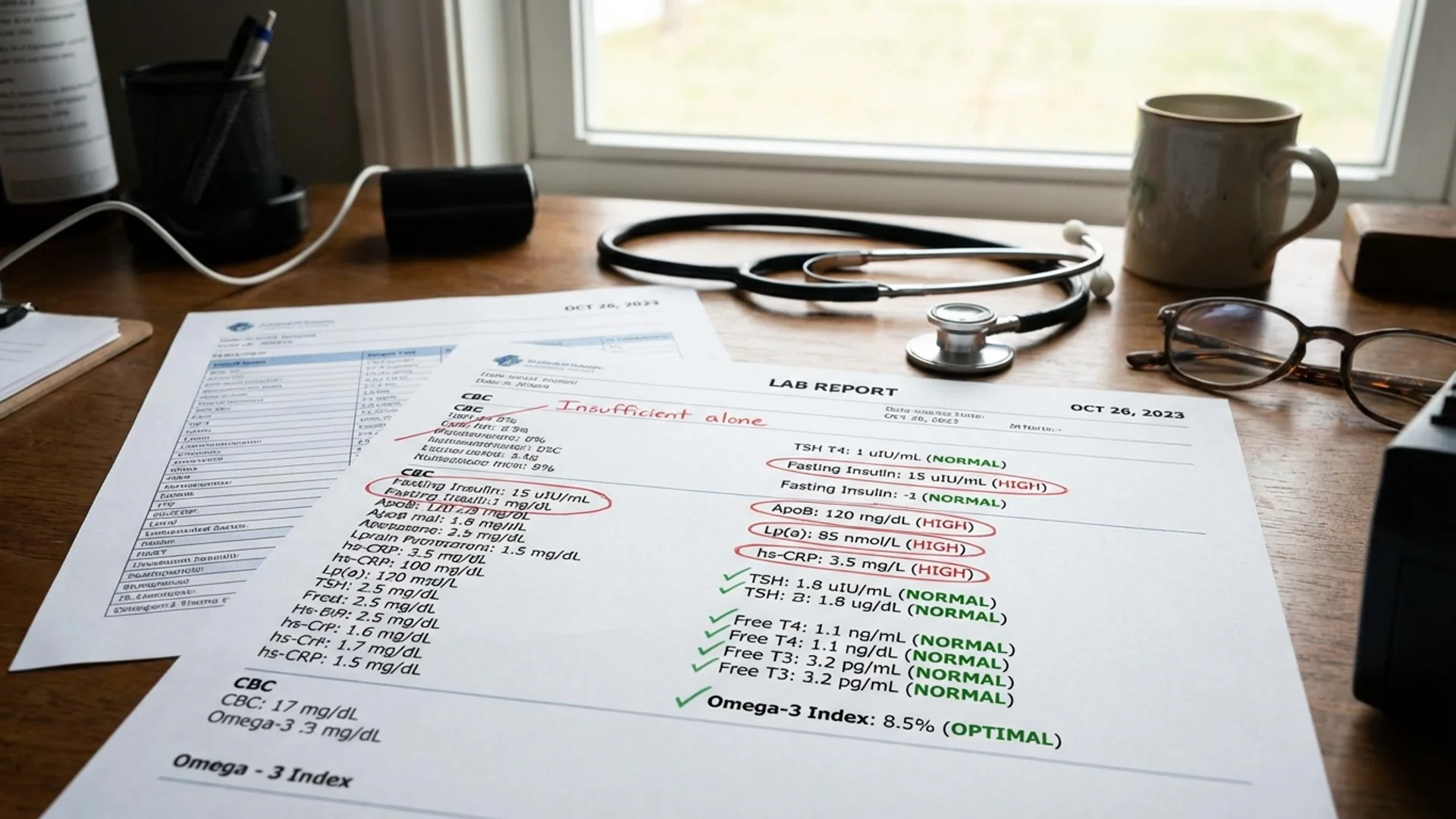
I have a consistent experience in my practice: patients arrive at Klinik St. Georg carrying folders of laboratory results from previous physicians, and those results are often described as “normal.” The patient clearly is not normal — they are fatigued, in pain, cognitively impaired, or struggling with recurrent infections — but their lab work says everything is fine.
The problem is rarely that the previous labs were done incorrectly. The problem is that the wrong tests were ordered. Standard diagnostic panels are designed to detect established disease. They are not designed to identify the functional imbalances, subclinical deficiencies, and early pathological changes that precede disease diagnosis by months or years.
This is what functional diagnostics addresses: the gap between “your labs are normal” and “I still feel terrible.”
The Limitations of Standard Testing
A standard health screening in most medical systems includes a complete blood count (CBC), basic metabolic panel, lipid panel, fasting glucose, and perhaps a thyroid screening (TSH alone). These tests are valuable for what they measure. The issue is what they leave out.
What a Standard CBC Misses
A CBC tells you how many white blood cells you have. It does not tell you which subtypes are present or how well they are functioning. A patient can have a normal total white blood cell count while having profoundly abnormal lymphocyte subset distribution — depleted NK cells, exhausted T cells, elevated activated B cells. This information is clinically critical for patients with chronic infections, autoimmune disease, or cancer, and it requires a lymphocyte subset panel to assess.
What Standard Thyroid Screening Misses
TSH alone is the standard thyroid screening test. But TSH can be normal while free T3 is low, reverse T3 is elevated, and thyroid antibodies are present. A full thyroid panel — TSH, free T4, free T3, reverse T3, anti-TPO antibodies, anti-thyroglobulin antibodies — provides a complete picture. Many patients with “normal thyroid function” based on TSH alone have subclinical thyroid dysfunction that explains their fatigue, weight gain, and cognitive complaints.
What Standard Metabolic Panels Miss
Fasting glucose is measured routinely. Fasting insulin is not — yet fasting insulin elevates years before glucose becomes abnormal. By the time fasting glucose is outside the reference range, insulin resistance has typically been present for five to 10 years. Measuring insulin alongside glucose identifies metabolic dysfunction at its earliest, most treatable stage.
Similarly, homocysteine, high-sensitivity CRP, and fibrinogen are not part of standard metabolic panels but provide critical information about methylation status, systemic inflammation, and cardiovascular risk, respectively.
The Functional Diagnostics Framework
The approach I use at Klinik St. Georg follows a systematic logic:
1. Comprehensive Blood Chemistry
Beyond the standard panel, I routinely assess:
- Full thyroid panel (TSH, fT3, fT4, rT3, anti-TPO, anti-TG)
- Fasting insulin alongside glucose (calculating HOMA-IR for insulin resistance)
- Inflammatory markers (hs-CRP, homocysteine, ferritin, fibrinogen)
- Nutrient status (vitamin D, B12, folate, zinc, selenium, magnesium RBC, iron studies with ferritin and transferrin saturation)
- Lipid subfraction analysis (not just total cholesterol and LDL, but particle size, oxidized LDL, Lp(a))
- Liver function beyond ALT/AST (GGT, alkaline phosphatase, bilirubin fractions)
2. Immune Profiling
For patients with chronic infections, autoimmune conditions, or unexplained immune dysfunction:
- Lymphocyte subset panel (CD4, CD8, CD4/CD8 ratio, NK cells, B cells, regulatory T cells)
- NK cell functional assay (cytotoxicity, not just counts)
- Cytokine panel (TNF-alpha, IL-6, IL-10, IFN-gamma)
- Immunoglobulin levels (IgG, IgA, IgM, IgG subclasses)
- CD57+ NK cells (in the context of suspected Lyme disease)
3. Gut and Microbiome Assessment
- Comprehensive stool analysis (GI-MAP or equivalent) — pathogens, commensal balance, inflammatory markers, digestive function
- Intestinal permeability markers (zonulin, LPS-binding protein)
- Fecal calprotectin (intestinal inflammation)
- Secretory IgA (mucosal immune function)
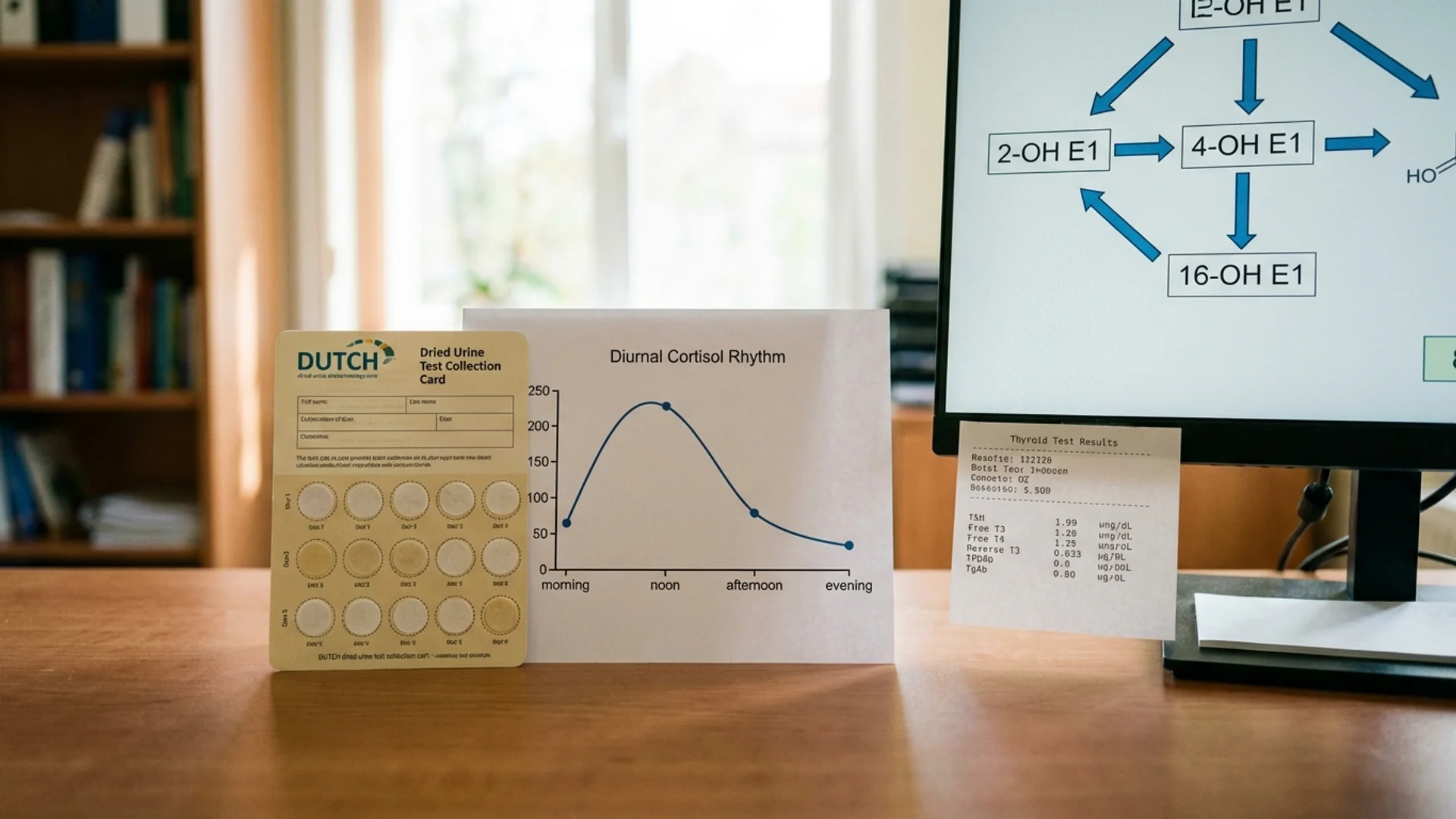
4. Hormonal Assessment
- Full sex hormone panel (testosterone, free testosterone, estradiol, progesterone, DHEA-S, SHBG)
- Cortisol rhythm (preferably salivary cortisol at four time points, or DUTCH test for cortisol metabolites)
- Thyroid (full panel as above)
- Growth hormone axis (IGF-1, IGFBP-3)
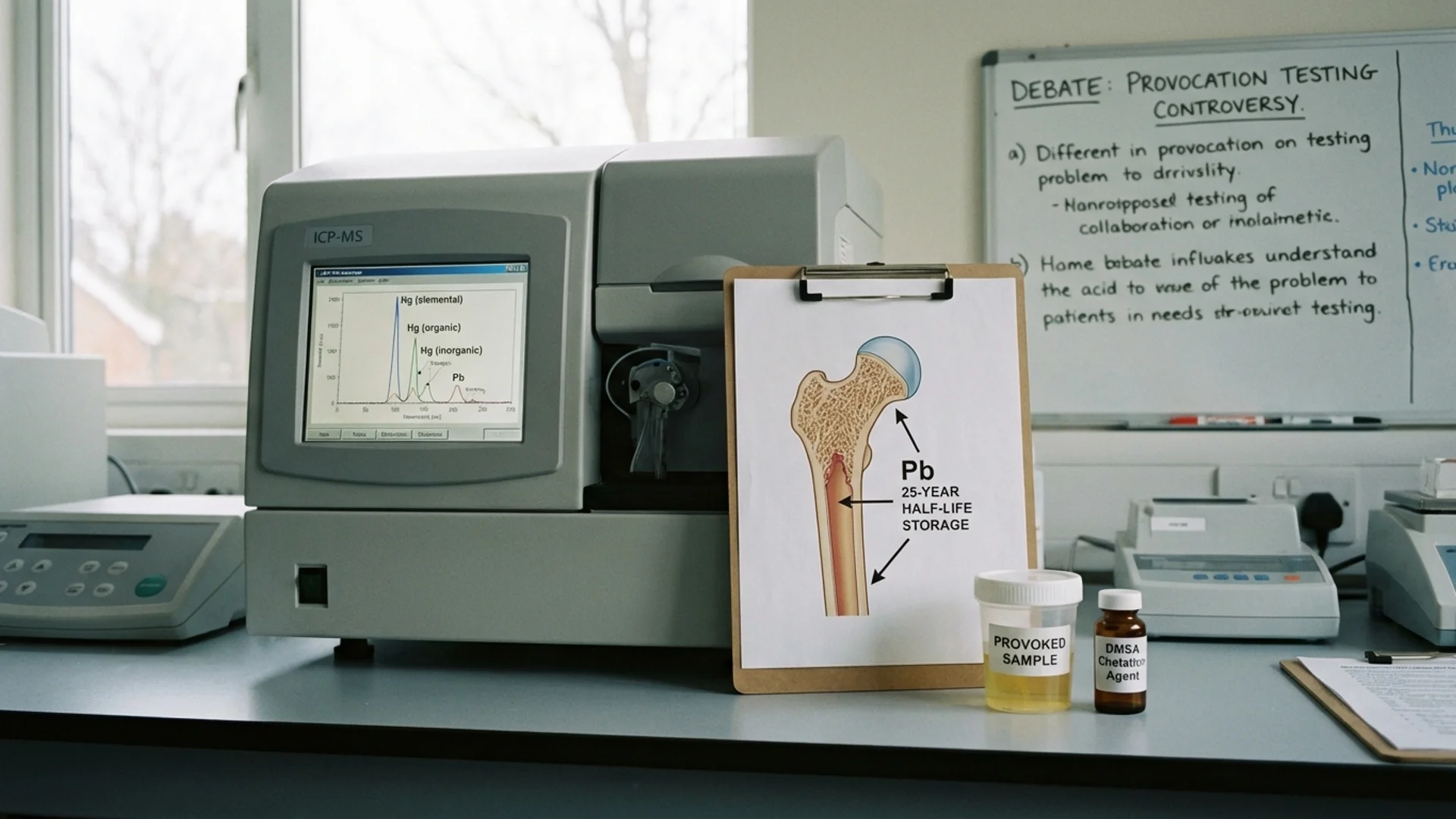
5. Toxicology
- Heavy metals (lead, mercury, cadmium, arsenic — provoked or unprovoked, depending on clinical context)
- Environmental toxins (mycotoxin panel, pesticide metabolites when indicated)
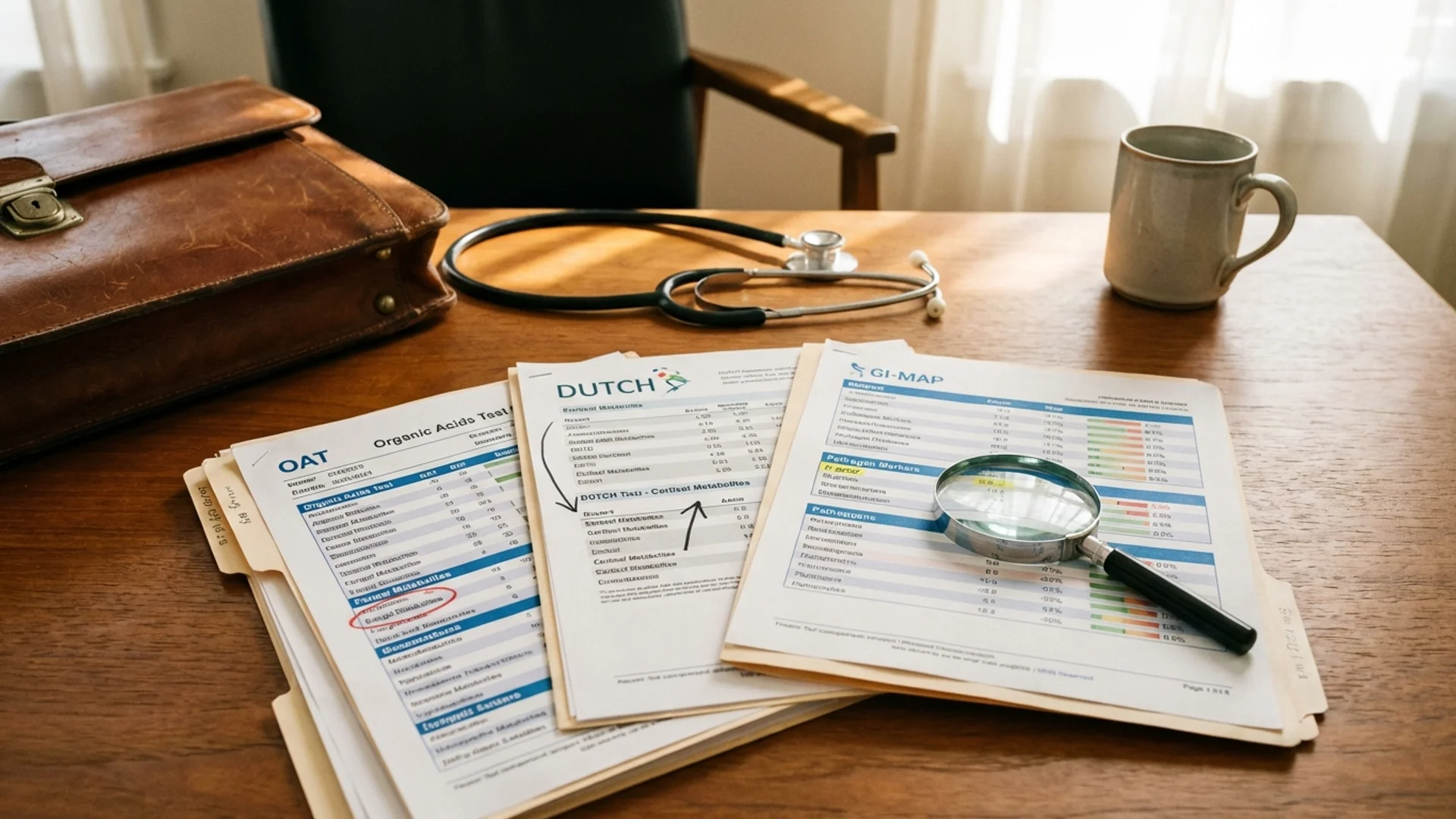
6. Specialized Testing
- Organic acids test (OAT) — metabolic intermediates that reveal mitochondrial function, neurotransmitter metabolism, nutrient status, and microbial metabolites
- DUTCH test — dried urine test for comprehensive hormones, including cortisol metabolites and sex hormone metabolites
- ELISpot testing — for cellular immune responses to specific pathogens (Lyme disease, viral reactivation)
- Oxidative stress markers (8-OHdG, MDA, glutathione levels)
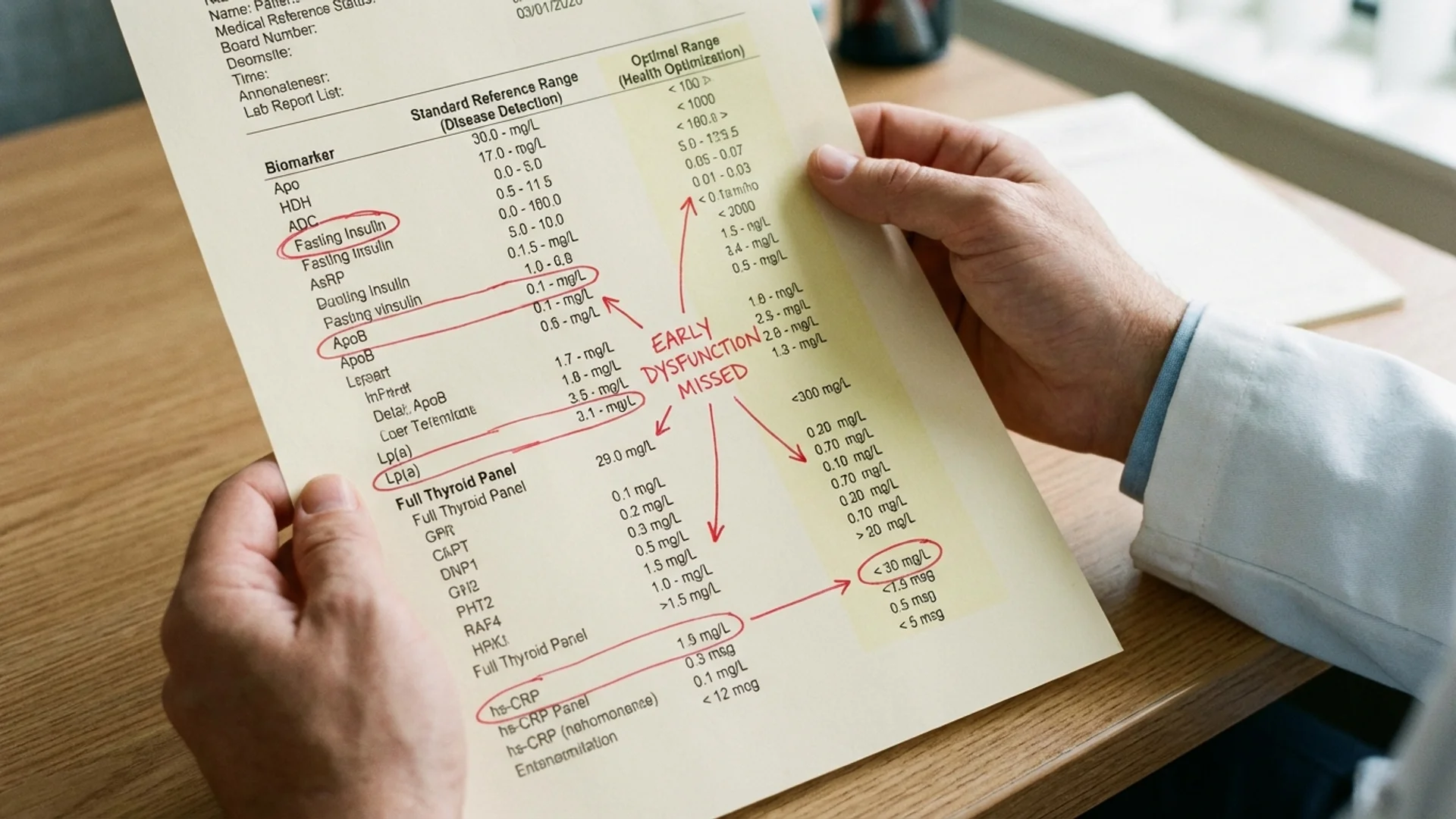
Reference Ranges vs. Optimal Ranges
One of the most important concepts in functional diagnostics is the distinction between reference ranges and optimal ranges.
Reference ranges are derived from the population of people who have blood drawn at a given laboratory. They represent the central 95% of results. The problem: the population being tested is not a healthy population. It includes people with undiagnosed conditions, subclinical deficiencies, and chronic disease. The reference range, therefore, represents the statistical norm, not the physiological optimum.
Examples:
| Marker | Reference Range | Optimal Range | Clinical Significance |
|---|---|---|---|
| Vitamin D (25-OH) | 30-100 ng/mL | 40-60 ng/mL | Below 40 is associated with immune impairment |
| Ferritin | 12-150 ng/mL (female) | 40-100 ng/mL | Below 40 often correlates with symptoms even when “normal” |
| TSH | 0.4-4.5 mIU/L | 0.5-2.0 mIU/L | Above 2.5 may indicate early thyroid dysfunction |
| Fasting insulin | 2-25 mIU/L | 3-8 mIU/L | Above 10 suggests insulin resistance |
| hs-CRP | 0-3.0 mg/L | Below 1.0 mg/L | Above 1.0 indicates clinically relevant inflammation |
| Homocysteine | 5-15 umol/L | Below 8 umol/L | Above 10 indicates methylation dysfunction |
I want to be transparent about an important nuance: optimal ranges are informed by clinical evidence and physiological reasoning, but they are not universally agreed upon. Different functional medicine practitioners use slightly different optimal ranges. What I present here reflects my clinical experience and the published evidence I find most persuasive.
When to Consider Functional Diagnostics
Not every patient needs every test. The appropriate panel depends on the clinical presentation. However, I recommend comprehensive functional diagnostics for patients who:
- Have been told their labs are “normal” despite persistent symptoms
- Have chronic fatigue, brain fog, or pain without clear diagnosis
- Have been diagnosed with an autoimmune condition and want to understand contributing factors
- Are dealing with chronic Lyme disease or post-COVID syndrome
- Want a proactive, prevention-focused health assessment
- Are preparing for intensive treatment (knowing baseline values improves treatment planning)
The goal is not to order tests for their own sake. The goal is to generate actionable information that changes the treatment plan. Every test I order should answer a specific clinical question.
The Practical Limitations
Functional diagnostics is not without limitations:
Cost. Many functional tests are not covered by standard health insurance. Patients should understand the costs before testing and prioritize based on clinical relevance.
Interpretation. The same result can mean different things in different clinical contexts. Functional diagnostics requires a physician who understands how to interpret results in the context of the individual patient, not just compare numbers to reference ranges.
Over-testing. It is possible to order too many tests, generating more data than can be meaningfully acted upon. The best functional diagnostics is targeted and hypothesis-driven, not shotgun.
Reproducibility. Some functional tests (particularly some specialized stool and urine analyses) have variable reproducibility between laboratories. Working with reputable, validated laboratories matters.
Despite these limitations, functional diagnostics remains one of the most valuable tools in integrative medicine. It transforms clinical care from reactive (waiting for disease to become diagnosable) to proactive (identifying and addressing dysfunction before it becomes disease).
Disclaimer: This article is provided for educational purposes and reflects one physician’s clinical perspective. It is not a substitute for individualized medical care. Diagnostic testing should be ordered and interpreted by a qualified physician in the context of a clinical evaluation.