Topic
Peptide Therapy
BPC-157, thymosin alpha-1, GHK-Cu, and the emerging clinical evidence. What works, what is hype, and what I use in practice.
Explore by Topic
BPC-157
Gastric pentadecapeptide for tissue repair, angiogenesis, and gastrointestinal healing.
TB-500 (Thymosin Beta-4)
Tissue repair peptide promoting cell migration, angiogenesis, and anti-fibrotic effects.
Thymosin Alpha-1
Immune-restoring thymic peptide approved in 35+ countries. Strongest evidence base of any therapeutic peptide.
GHK-Cu
Copper-binding tripeptide modulating 4,000+ genes for tissue remodeling and collagen synthesis.
LL-37
Human cathelicidin antimicrobial peptide for biofilm disruption and innate immune defense.
KPV
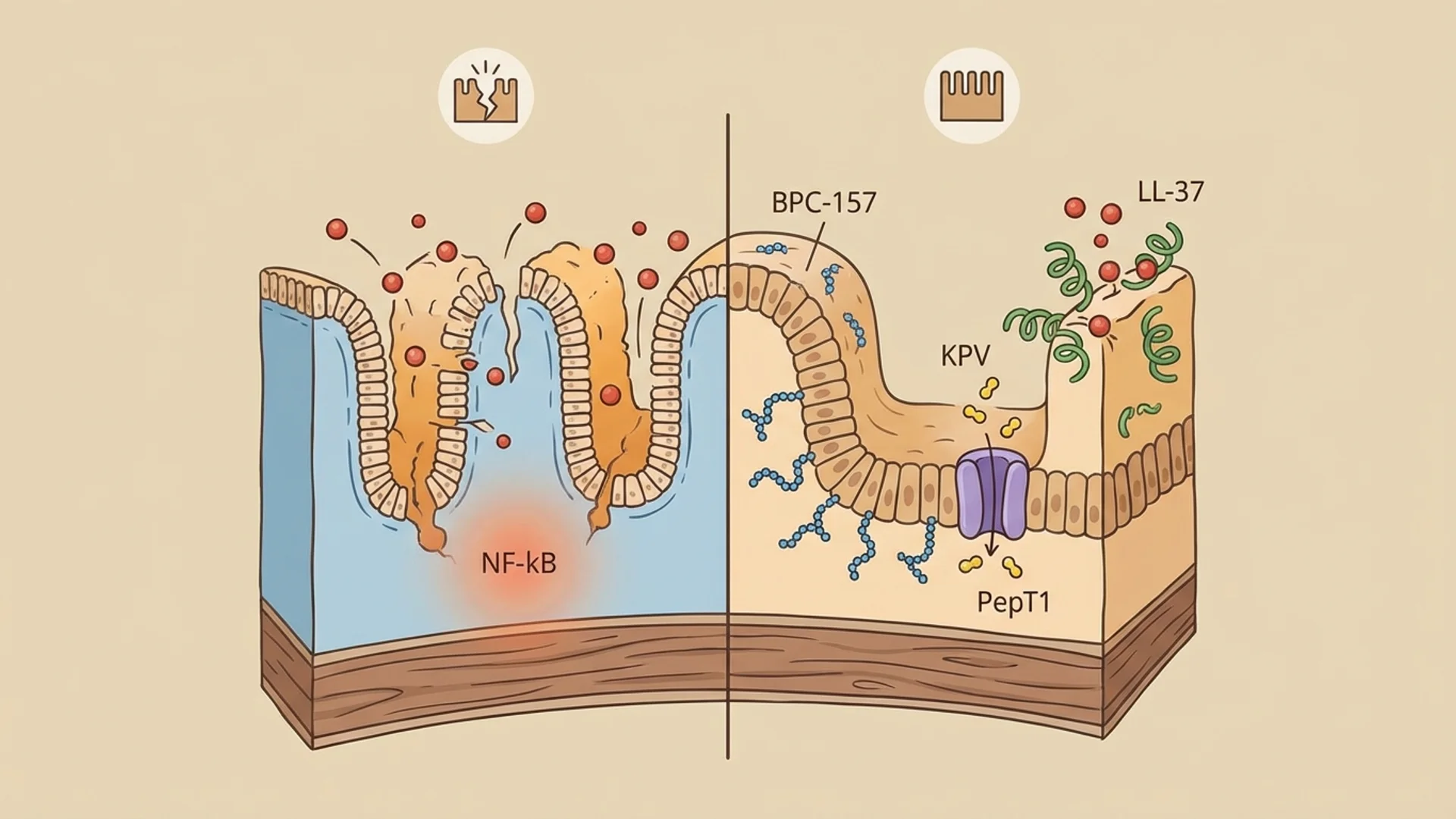
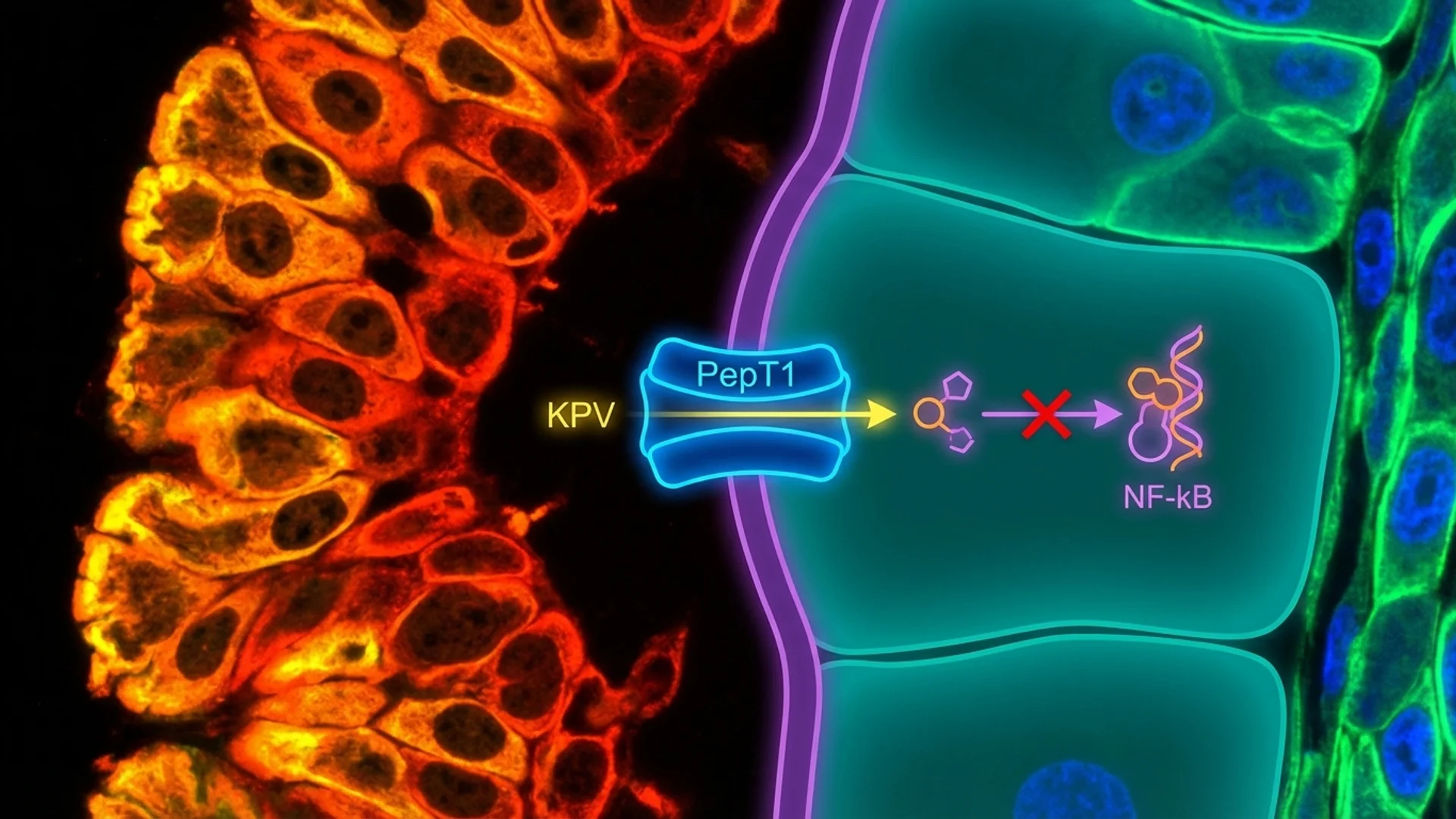
Alpha-MSH fragment for NF-kB inhibition with preferential uptake in inflamed gut tissue.
Selank
Synthetic tuftsin-derived anxiolytic and nootropic peptide. Approved in Russia.
DSIP
Endogenous neuropeptide modulating sleep architecture and the stress-hormone axis.
Epithalon
Telomerase-activating tetrapeptide for anti-aging and melatonin restoration.
Dihexa
Synthetic hexapeptide promoting synaptogenesis through the HGF/c-Met receptor system.
CJC-1295 / Ipamorelin
Growth hormone secretagogues stimulating pulsatile GH release through complementary pituitary pathways.
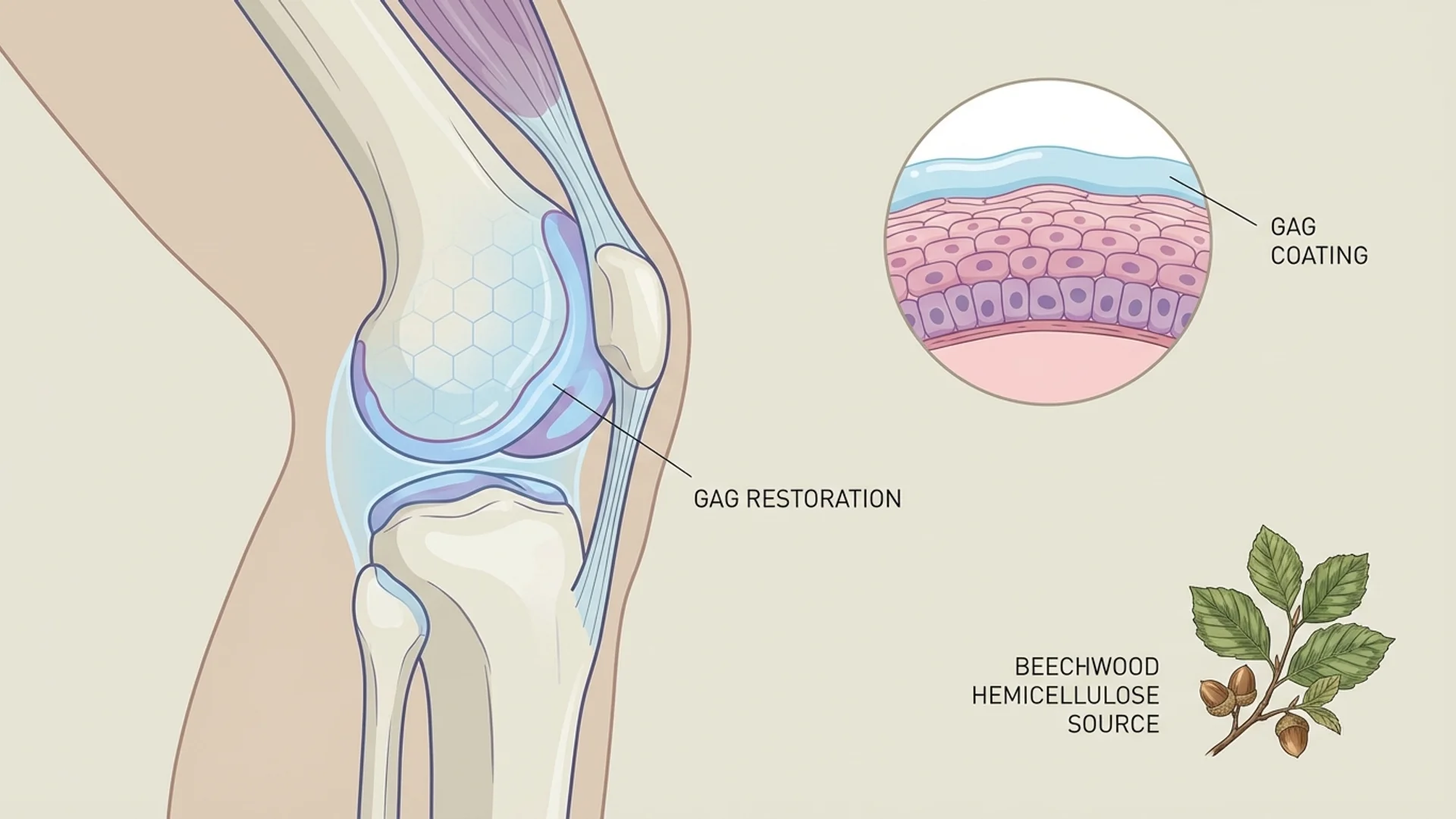
Pentosan Polysulfate
FDA-approved GAG-layer restoring agent for interstitial cystitis and osteoarthritis.
Peptide Safety
Safety profiles, monitoring requirements, and risk assessment across peptide compounds.
Peptide Sourcing
How to ensure pharmaceutical-grade quality and avoid grey-market risks.
Peptide Protocols
Clinical protocols combining multiple peptides for specific conditions.
Free Guide
The Physician's Complete Guide to Peptide Therapy
Download the complete physician's guide. Evidence-based, no hype.
Articles
45 articles
BPC-157 Dosage Guide: Subcutaneous, Oral, and Injection Protocols
Evidence-based BPC-157 dosing protocols. Subcutaneous vs oral routes, loading vs maintenance, body weight calculations, and clinical observations.
BPC-157 Side Effects: What the Evidence Actually Shows
Honest assessment of BPC-157 side effects, safety data, FDA warnings, and theoretical risks. What we know, what we don't, and what to watch for.
BPC-157 vs TB-500: Which Peptide for Tissue Repair?
A clinical comparison of BPC-157 and TB-500 for tissue repair. Mechanisms, evidence quality, best use cases, combination protocols, and what I observe in practice.
CJC-1295/Ipamorelin Dosage: Growth Hormone Protocol
Evidence-based CJC-1295/Ipamorelin dosing guide by Dr. Julian Douwes. Nightly subcutaneous protocols, DAC vs no-DAC, cycling, and growth hormone optimization.
CJC-1295/Ipamorelin for Weight Loss and Body Composition
CJC-1295/Ipamorelin for fat loss and body recomposition. Dr. Julian Douwes explains growth hormone mechanisms, realistic timelines, and what the evidence supports.
Dihexa Dosage: Nootropic Protocol and Safety
Dihexa dosing guide by Dr. Julian Douwes. Oral and subcutaneous protocols, the c-Met safety question, and why caution is warranted with this potent nootropic peptide.
Dihexa Safety: The c-Met Cancer Risk Question
Dihexa safety analysis by Dr. Julian Douwes. The HGF/c-Met oncogenic pathway concern, retracted research, failed clinical trials, and what patients must understand.
DSIP Dosage and Protocol for Sleep
Evidence-based DSIP dosing guide for sleep. Subcutaneous protocols, timing, cycling, and realistic expectations from Dr. Julian Douwes.

DSIP vs Melatonin: Which Sleep Peptide?
DSIP vs melatonin comparison by Dr. Julian Douwes. Sleep architecture modulation vs circadian timing — mechanisms, evidence levels, and when to use each.
Epithalon Dosage: Telomere Protocol and Cycling
Evidence-based Epithalon dosing guide. Injection protocols, 10-20 day cycling, annual scheduling, and telomere monitoring from Dr. Julian Douwes.
Epithalon vs NMN: Anti-Aging Mechanisms Compared
Epithalon vs NMN comparison by Dr. Julian Douwes. Telomere lengthening vs NAD+ replenishment — different aging hallmarks, different evidence, and when to use each.
GHK-Cu Dosage: Topical, Injection, and Combination Protocols
Complete GHK-Cu dosing guide. Topical concentrations, subcutaneous injection protocols, microneedling delivery, and combination strategies.
GHK-Cu for Skin: Anti-Aging Evidence and Protocols
GHK-Cu copper peptide for skin anti-aging. Collagen synthesis, wrinkle reduction evidence, topical vs injectable protocols, and retinol comparison.
How to Inject Peptides: A Step-by-Step Patient Guide
Step-by-step guide to subcutaneous peptide injection. Equipment, reconstitution, injection sites, rotation, storage, and sterility from a physician's perspective.
KPV for Gut Inflammation: IBD, Colitis, and Clinical Evidence
How the KPV tripeptide reduces gut inflammation. NF-kB inhibition, PepT1 uptake, IBD and colitis evidence, oral dosing, and clinical observations.
Are Peptides Legal? A 2026 Regulatory Guide
Comprehensive guide to peptide legality in 2026. FDA regulations, EU framework, Australia's scheduling, compounding pharmacy rules, and grey market risks explained by a physician.
LL-37 for Biofilm Disruption in Chronic Lyme
How LL-37 disrupts Borrelia biofilms in chronic Lyme disease. Mechanism, preclinical evidence, protocol context, and clinical observations.
LL-37 and Vitamin D: The Immune Connection
How vitamin D regulates LL-37 production and why this matters for immunity. The cathelicidin pathway, optimal levels, and clinical implications.
Pentosan Polysulfate for Knee Osteoarthritis
Pentosan polysulfate for knee OA by Dr. Julian Douwes. Disease-modifying potential, subcutaneous protocols, cartilage repair evidence, and comparison with hyaluronic acid.
Pentosan Polysulfate Eye Toxicity: Maculopathy Risk
Pentosan polysulfate maculopathy explained by Dr. Julian Douwes. Retinal toxicity risk, screening guidelines, reversibility questions, and what every PPS user must know.
Selank Dosage: Nasal Spray Protocol and Cycling
Evidence-based Selank dosing guide. Intranasal spray protocols, cycling schedules, stacking considerations, and what I observe in clinical practice.
Selank vs Semax: Anxiolytic vs Nootropic Compared
Selank vs Semax comparison by Dr. Julian Douwes. GABAergic anxiolytic vs dopaminergic nootropic — mechanisms, evidence, dosing, and which to choose.
Semaglutide: Beyond Weight Loss — A Physician's Assessment
An evidence-based clinical assessment of semaglutide. GLP-1 mechanism, cardiovascular benefits, neuroprotective signals, muscle loss concerns, and who should and should not use it.
TB-500 Dosage: Loading, Maintenance, and Cycling
Evidence-based TB-500 dosing protocols. Loading and maintenance phases, injection frequency, cycling schedules, and clinical dosing rationale.
TB-500 Side Effects and Safety
Honest assessment of TB-500 side effects, WADA ban context, theoretical risks, and what clinical experience shows about Thymosin Beta-4 safety.
TB-500 for Tendon and Ligament Repair
How TB-500 supports tendon and ligament healing. Mechanisms, preclinical evidence, clinical observations, and practical protocols for connective tissue.
Thymosin Alpha-1 for Cancer: Immunotherapy Support
How Thymosin Alpha-1 supports cancer immunotherapy. T-cell activation, dendritic cell maturation, clinical trial data, and practical protocols.
Thymosin Alpha-1 Dosage and Protocol
Evidence-based Thymosin Alpha-1 dosing. Subcutaneous protocols for immune support, cancer adjunct, infection, and chronic disease applications.
BPC-157: What the Research Actually Shows
Honest physician's assessment of BPC-157 peptide. Mechanisms, animal vs human evidence, dosing, safety, and clinical observations from Dr. Julian Douwes.
CJC-1295/Ipamorelin: Growth Hormone Secretagogues
CJC-1295 and Ipamorelin review by Dr. Julian Douwes. Growth hormone optimization, body composition, evidence for GH secretagogues, dosing and safety.
Dihexa: The Cognitive Peptide with Limited Data
Dihexa peptide review by Dr. Julian Douwes. Potent cognitive peptide, HGF/c-Met mechanism, extremely limited human data, and why caution is warranted.
DSIP: Delta Sleep-Inducing Peptide for Sleep
DSIP peptide review by Dr. Julian Douwes. Delta sleep-inducing peptide for sleep regulation, stress resilience, and neuroendocrine balance. Evidence assessment.
Epithalon: Telomerase Activation and Anti-Aging
Epithalon peptide review by Dr. Julian Douwes. Telomerase activation, longevity research, limited human data, and the telomere-cancer question examined honestly
GHK-Cu: The Copper Peptide for Tissue Remodeling
GHK-Cu copper peptide review. Gene expression modulation, wound healing, skin rejuvenation, and anti-aging research assessed by Dr. Julian Douwes.
Peptide Therapy for Gut Healing
How BPC-157, KPV, and LL-37 support gastrointestinal repair. Dr. Julian Douwes explains peptide protocols for IBD, leaky gut, and gut barrier dysfunction.
KPV: The Anti-Inflammatory Tripeptide for Gut Health
KPV peptide review by Dr. Julian Douwes. Anti-inflammatory tripeptide derived from alpha-MSH, researched for IBD and gut healing. Evidence and clinical use.
LL-37: The Antimicrobial Peptide for Innate Immunity
LL-37 antimicrobial peptide review by Dr. Julian Douwes. Innate immunity, biofilm disruption, Lyme disease applications, and clinical perspective.
Peptide Therapy for Lyme Disease
How Dr. Julian Douwes uses peptides in chronic Lyme disease treatment. Thymosin alpha-1, LL-37, BPC-157 protocols alongside standard Lyme therapy.
Pentosan Polysulfate: Beyond Bladder Conditions
Pentosan polysulfate (PPS) review by Dr. Julian Douwes. FDA-approved for IC, emerging osteoarthritis evidence, unique mechanism, and clinical applications.
Peptide Therapy for Recovery and Performance
BPC-157 and TB-500 for injury recovery, surgical healing, and athletic performance. Evidence-based protocol from Dr. Julian Douwes.
Peptide Safety: What You Need to Know
Comprehensive guide to peptide therapy safety. Regulatory status, quality concerns, side effects, contraindications, and why physician oversight matters.
Selank: The Anxiolytic Peptide from Russia
Selank peptide review by Dr. Julian Douwes. Russian-developed anxiolytic and nootropic peptide, nasal administration, BDNF modulation, and evidence assessment.
Peptide Sourcing: Hospital-Grade vs. Grey Market
Guide to peptide sourcing and quality. Compounding pharmacies vs research chemicals, testing standards, what to look for, and why source matters for safety.
TB-500: Thymosin Beta-4 for Tissue Repair
Evidence-based review of TB-500 peptide for tissue repair and wound healing. Mechanisms, research status, dosing, and clinical perspective from Dr. Julian Douwe
Thymosin Alpha-1: The Immune Modulator with Real Data
Thymosin Alpha-1 review by Dr. Julian Douwes. Approved in 35+ countries, backed by human clinical trials. Immune modulation for infections and cancer support.
Complete Guide
The Physician's Guide to Peptide Therapy
In-depth reference by Dr. Julian Douwes
The Complete Guide to Peptides: A Physician’s Perspective
By Dr. Julian Douwes, M.D. — Chief Medical Officer, Klinik St. Georg
Key Takeaways:
- Peptides are short chains of amino acids that act as signaling molecules throughout the body, influencing everything from tissue repair to immune regulation to cognitive function.
- The evidence base for therapeutic peptides varies enormously — some have robust human clinical trial data, while others rely primarily on animal models and clinical observation.
- Regulatory status differs by jurisdiction and by peptide. Patients should understand that many peptides used in clinical practice are not FDA-approved for the indications they are commonly prescribed for.
- Quality control is a genuine concern. Not all peptide sources are equivalent, and contamination, degradation, and mislabeling are documented problems in the compounding and gray-market supply chain.
- Peptides are tools in a broader clinical framework — not standalone solutions. In my practice, they are integrated into comprehensive treatment protocols that address root causes, not symptoms alone.
Table of Contents
- What Are Peptides?
- How Peptides Work
- Categories of Therapeutic Peptides
- Are Peptides Safe?
- How I Use Peptides in Practice
- Understanding the Evidence Hierarchy
What Are Peptides?
At the most basic level, peptides are short chains of amino acids — typically between 2 and 50 amino acids in length. Once a chain exceeds roughly 50 amino acids, we generally classify it as a protein. This distinction matters because peptides, by virtue of their smaller size, tend to have different pharmacokinetic properties than larger proteins: they can be more readily absorbed, they often have shorter half-lives, and they frequently act as highly specific signaling molecules.
Your body produces thousands of endogenous peptides. Insulin, with 51 amino acids, sits right at the boundary between peptide and protein. Oxytocin, at 9 amino acids, is unambiguously a peptide. Growth hormone-releasing hormone, thymosin beta-4, and brain-derived neurotrophic factor fragments are all peptides your body manufactures and uses for specific physiological purposes.
What has changed in the last two decades is our ability to synthesize these molecules — and novel analogs of them — in the laboratory. This has opened up therapeutic possibilities that did not exist when I began practicing medicine. It has also opened the door to considerable confusion, misinformation, and in some cases genuine risk.
Let me be clear about something from the outset: peptides are not a category of supplement. They are bioactive molecules that interact with specific receptor systems and signaling pathways. They deserve the same rigor of evaluation that we would apply to any pharmaceutical intervention.
How Peptides Work
Receptor Binding and Signal Transduction
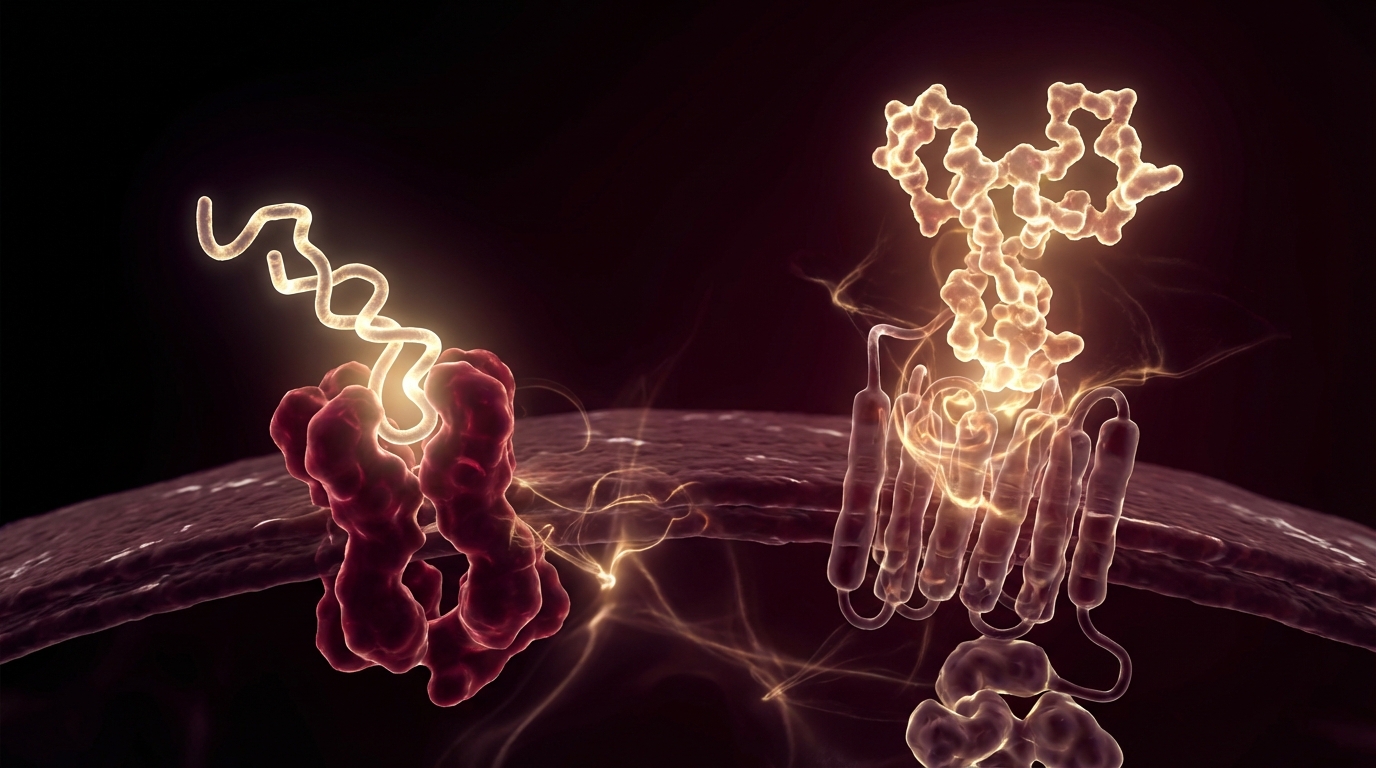
Most therapeutic peptides exert their effects by binding to specific cell-surface receptors. When a peptide binds to its target receptor, it initiates a signaling cascade inside the cell — a series of biochemical events that ultimately change cell behavior. This is the same fundamental mechanism by which your body’s endogenous peptides work.
The specificity of this receptor binding is both the strength and the limitation of peptide therapy. A peptide that binds tightly to the growth hormone secretagogue receptor will reliably stimulate growth hormone release. But if that same receptor exists in tissues you were not targeting, you may see effects you did not intend.
Bioavailability and Administration
One of the practical challenges with peptide therapy is bioavailability. Peptides are, after all, chains of amino acids — and your digestive system is specifically designed to break amino acid chains apart. This is why most therapeutic peptides are administered by subcutaneous injection rather than orally. The peptide is injected into the fatty tissue just beneath the skin, from which it is absorbed into the bloodstream relatively intact.
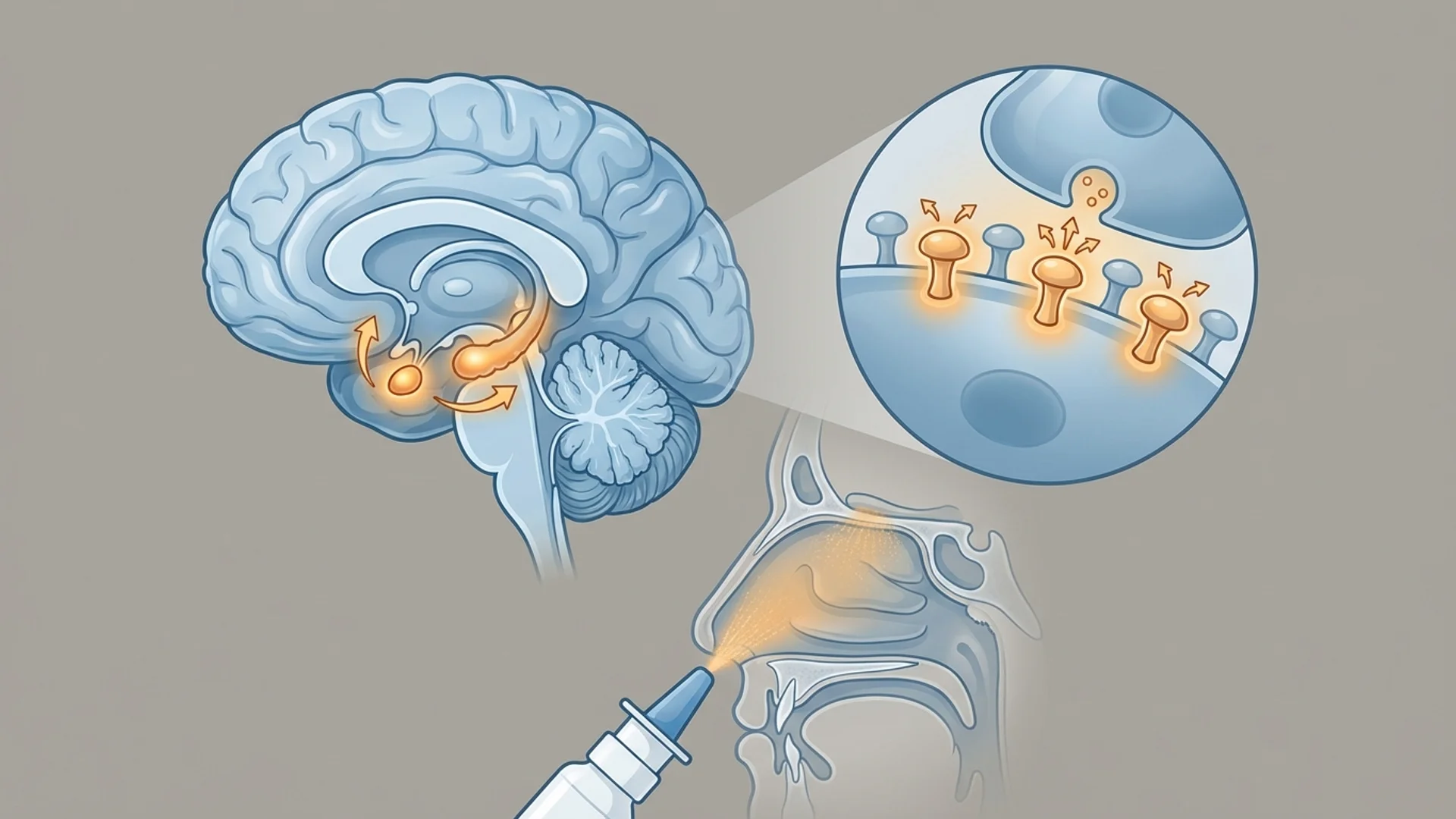
Some peptides can be administered intranasally, which exploits the rich vascular supply of the nasal mucosa to achieve systemic absorption while bypassing first-pass hepatic metabolism. A smaller number of peptides have been formulated for oral administration using protective encapsulation technologies, though oral bioavailability remains generally inferior to injectable routes.
Half-life is another critical consideration. Many naturally occurring peptides have half-lives measured in minutes. Therapeutic analogs are often engineered with amino acid substitutions or chemical modifications that extend their half-life, but even so, most therapeutic peptides are cleared from circulation within hours. This has implications for dosing frequency and for the design of treatment protocols.
Downstream Effects
The downstream effects of peptide signaling are diverse. Depending on the peptide and its target, you may see:
- Upregulation of growth factors — increased production of VEGF, EGF, FGF, or other growth factors that drive tissue repair and angiogenesis
- Modulation of inflammatory pathways — shifting the balance between pro-inflammatory and anti-inflammatory cytokines
- Neuroendocrine signaling — stimulation or inhibition of hormone release from the pituitary, hypothalamus, or other endocrine organs
- Immune cell activation or suppression — direct effects on T-cell function, NK cell activity, or macrophage polarization
- Epigenetic modification — some peptides appear to influence gene expression through chromatin remodeling, though this is an area where mechanistic understanding remains incomplete
Categories of Therapeutic Peptides
Healing and Tissue Repair Peptides
BPC-157 (Body Protection Compound-157)
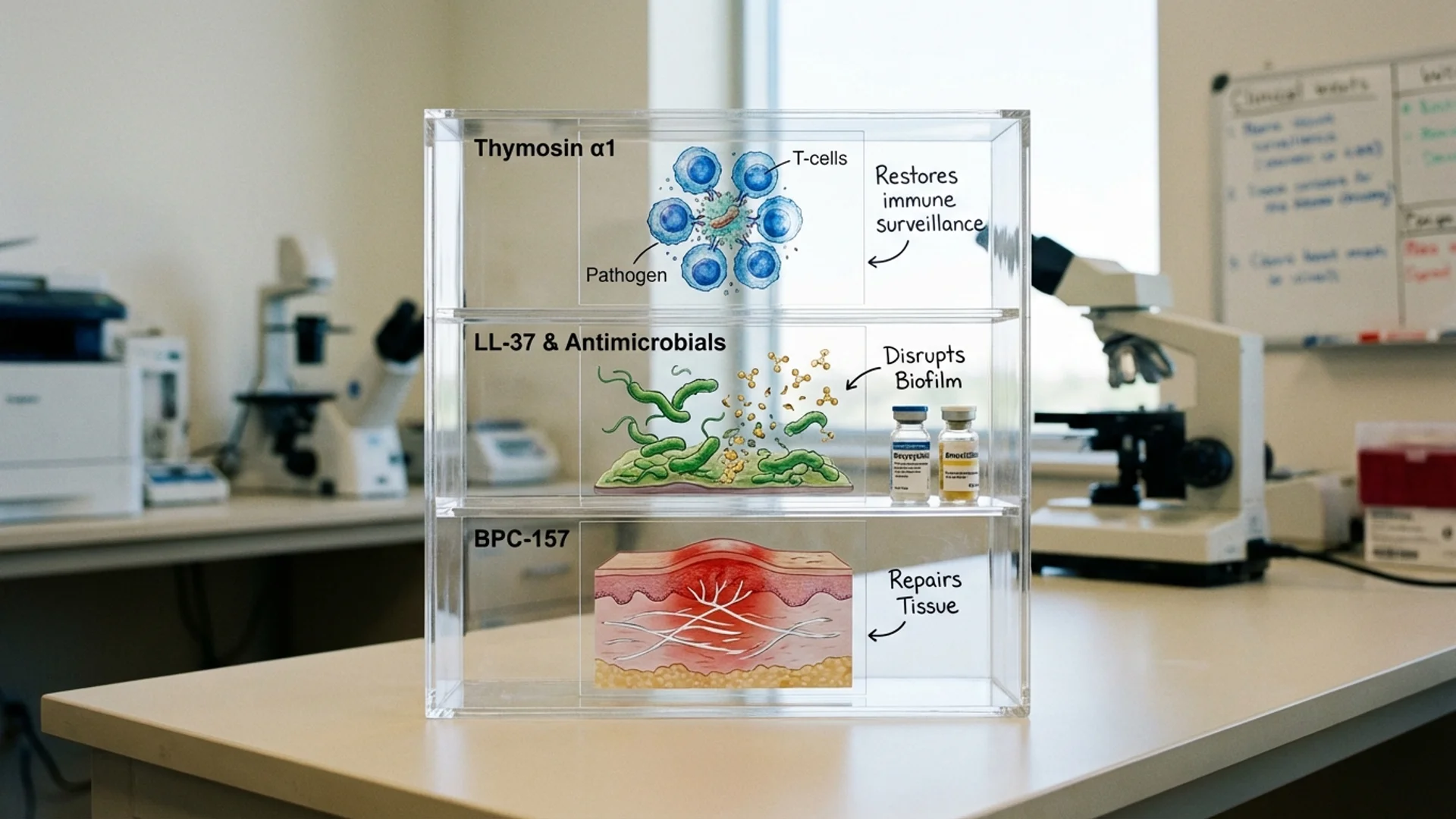
BPC-157 is a synthetic 15-amino-acid peptide derived from a sequence found in human gastric juice. It has been the subject of extensive preclinical research — and I want to emphasize the word “preclinical.” The vast majority of published BPC-157 studies are animal models: rats with severed tendons, mice with induced colitis, rabbits with muscle injuries.
In these animal models, BPC-157 has demonstrated remarkable effects: accelerated tendon healing, enhanced angiogenesis, protection against NSAID-induced gut damage, and neuroprotective properties. The proposed mechanisms include upregulation of growth hormone receptor expression, activation of the FAK-paxillin pathway in tendon fibroblasts, and modulation of the nitric oxide system.
What we do not have, as of this writing, are large-scale randomized controlled human trials. What we have instead is a growing body of clinical observation from physicians who have integrated BPC-157 into their practice.
TB-500 (Thymosin Beta-4 Fragment)
TB-500 is a synthetic fragment of thymosin beta-4, a 43-amino-acid peptide that plays a central role in actin regulation and cell migration. In preclinical models, TB-500 has shown effects on wound healing, cardiac repair following ischemic injury, and reduction of inflammatory fibrosis.
The evidence base for TB-500 is similar in character to BPC-157: strong preclinical signals, limited controlled human data, and a growing volume of clinical observation. Thymosin beta-4 itself has been studied in human clinical trials for dry eye (Timbion/RegeneRx) and cardiac repair, which provides some translational context for the fragment.
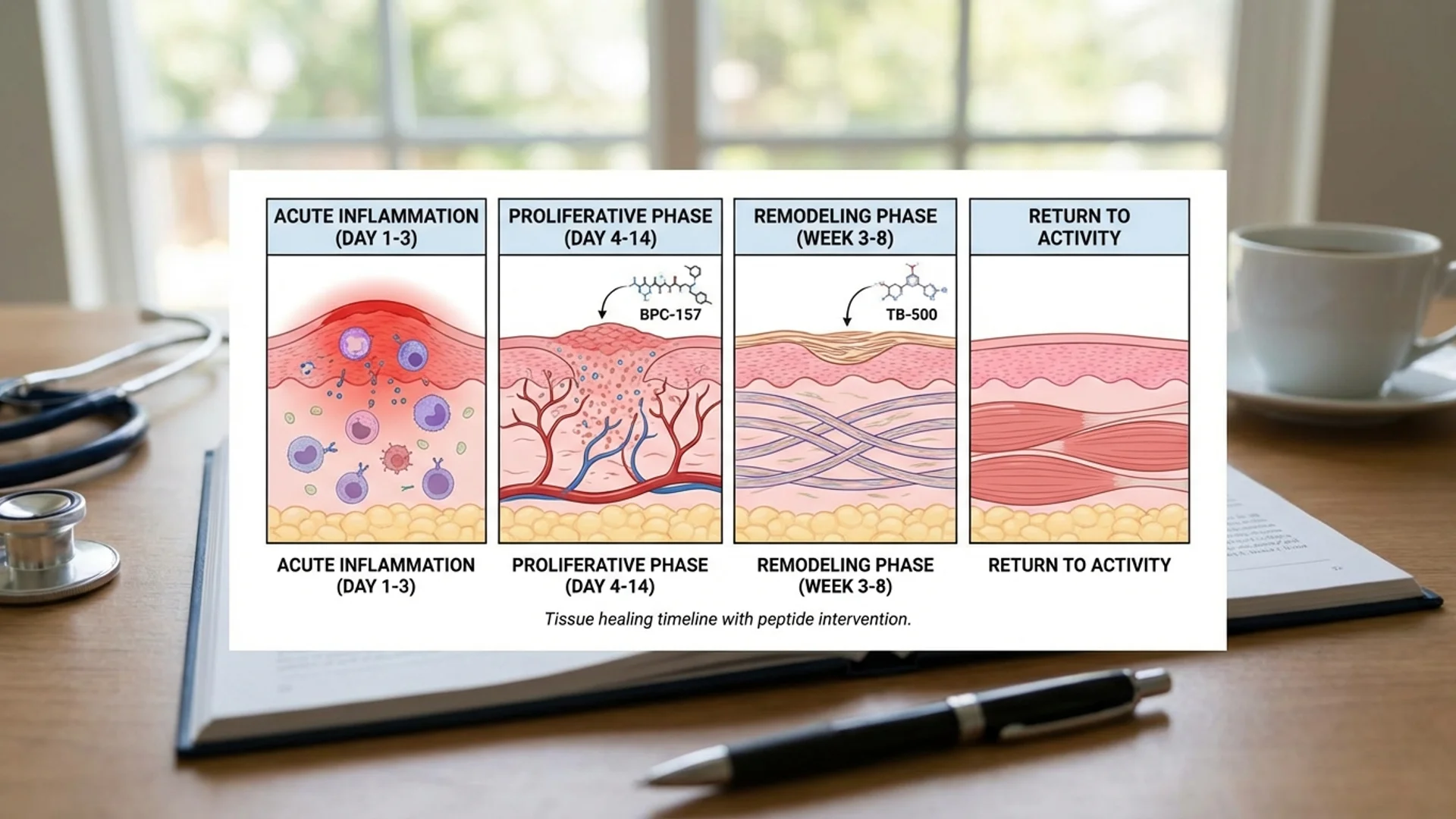
In practice, BPC-157 and TB-500 are frequently combined in tissue repair protocols. The rationale is that they appear to work through complementary mechanisms — BPC-157 primarily through growth factor and angiogenesis pathways, TB-500 primarily through actin polymerization and cell migration.
Immune-Modulating Peptides
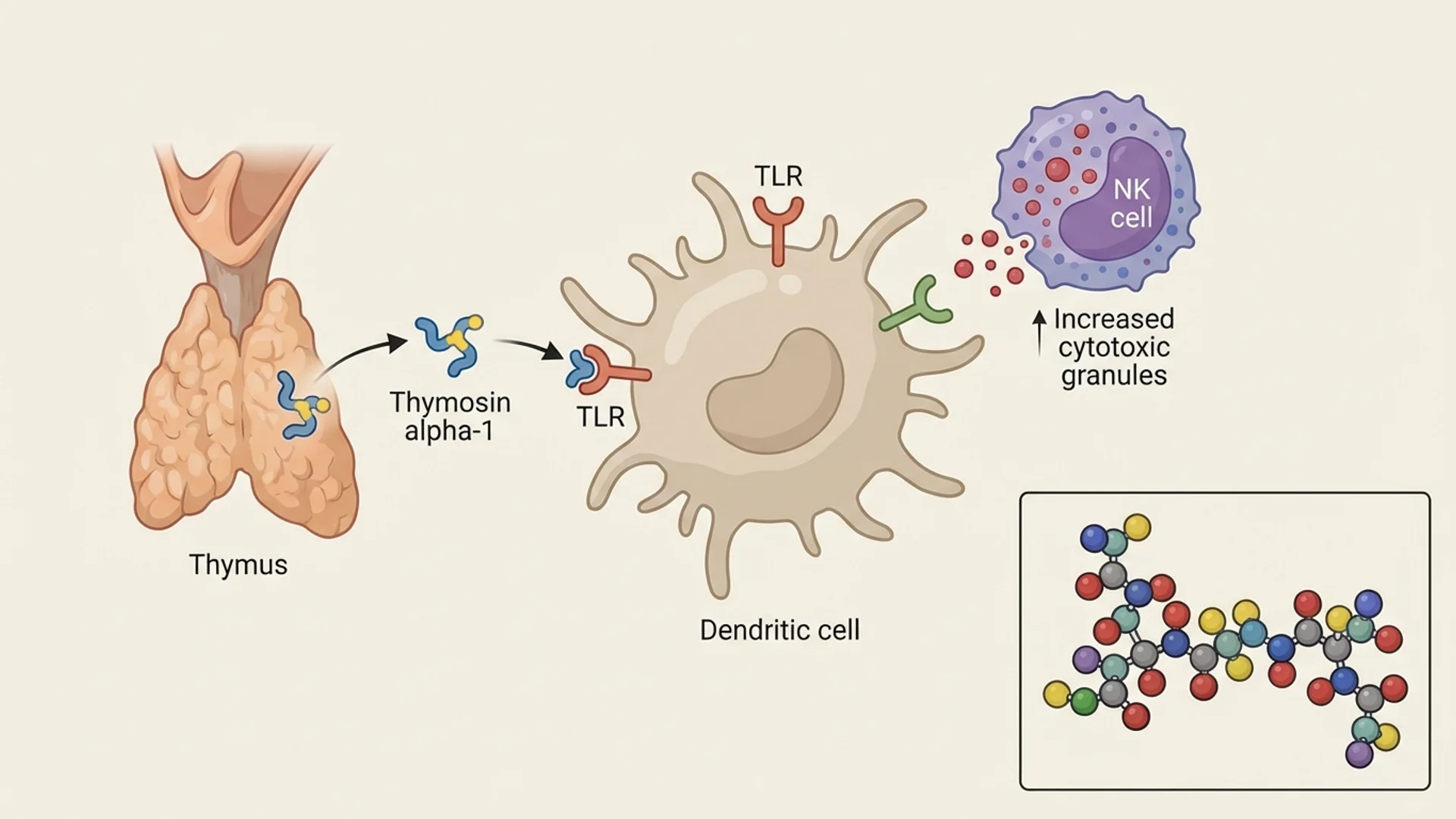
Thymosin alpha-1 occupies a different position in the evidence hierarchy than most therapeutic peptides. It is an approved pharmaceutical in over 35 countries for the treatment of hepatitis B, hepatitis C, and as an immune adjuvant. It has been the subject of numerous human clinical trials and has a well-characterized safety profile.
Ta1 acts primarily on dendritic cells and T-lymphocytes. It promotes the maturation of dendritic cells, enhances antigen presentation, and stimulates the differentiation of T-cell precursors into mature, functional T-cells. In clinical practice, I find Ta1 particularly relevant in the context of chronic infections where immune exhaustion is a factor.
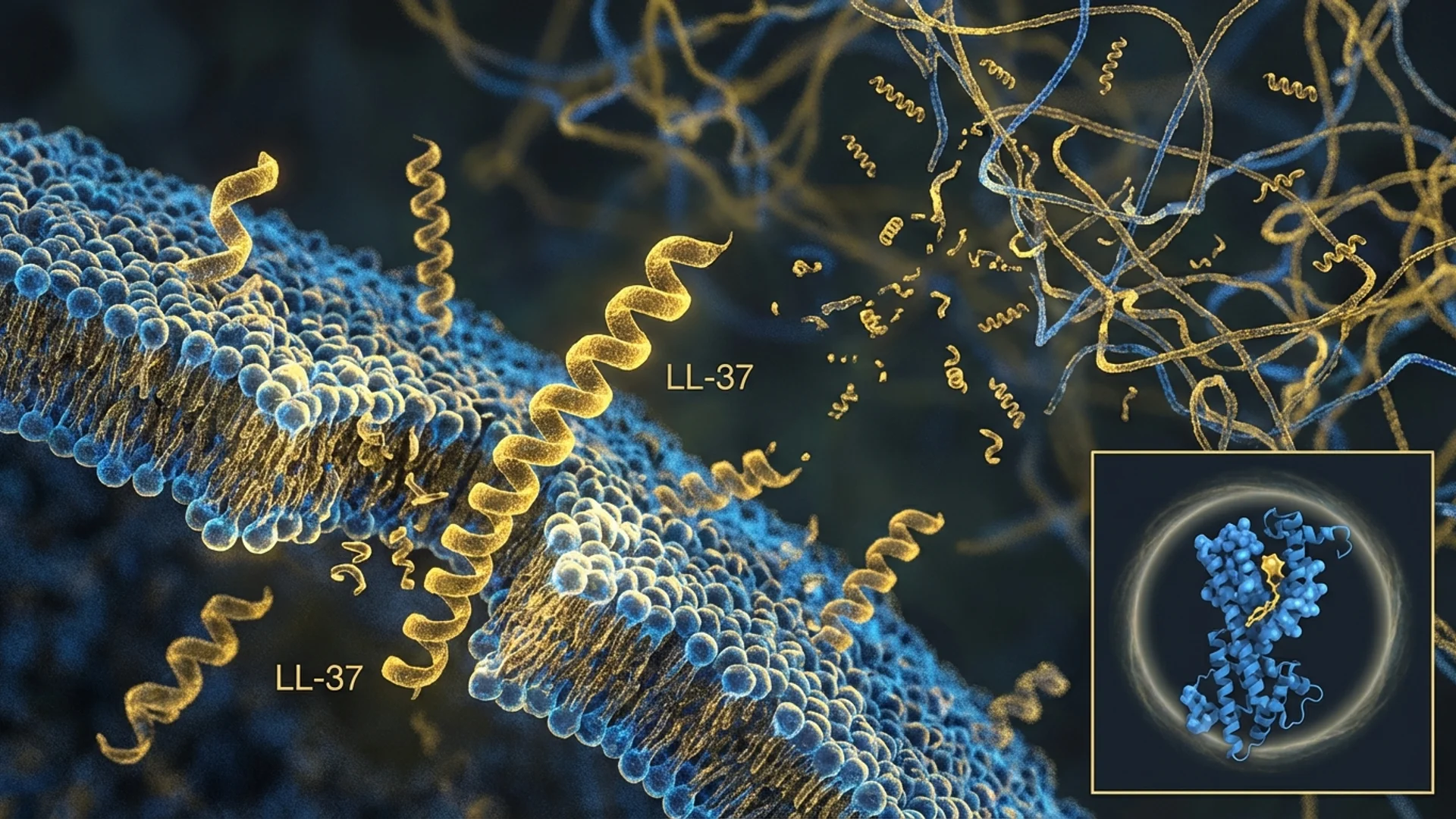
LL-37 is the only human cathelicidin antimicrobial peptide. It is part of the innate immune system and has direct antimicrobial activity against bacteria, fungi, and enveloped viruses. Beyond its direct antimicrobial effects, LL-37 modulates inflammation, promotes wound healing, and influences adaptive immune responses.
Research into therapeutic applications of LL-37 is earlier-stage than Ta1, but the peptide is of particular interest in the context of biofilm-associated infections — a relevant consideration in chronic Lyme disease, where Borrelia burgdorferi biofilm formation is a proposed mechanism of persistence.
KPV is a tripeptide (Lys-Pro-Val) derived from alpha-melanocyte-stimulating hormone (alpha-MSH). It has demonstrated anti-inflammatory effects in preclinical models of inflammatory bowel disease, acting through inhibition of NF-kB signaling and modulation of inflammatory cytokine production.
Cognitive and Neuroprotective Peptides
Selank is a synthetic analog of the endogenous peptide tuftsin, developed at the Institute of Molecular Genetics of the Russian Academy of Sciences. It is approved in Russia as an anxiolytic and nootropic medication. Selank modulates the expression of brain-derived neurotrophic factor (BDNF) and influences the balance of monoamine neurotransmitters, including serotonin and dopamine.
Dihexa is a synthetic hexapeptide analog of angiotensin IV that has shown remarkable potency in preclinical models of cognitive enhancement. It operates through the hepatocyte growth factor/c-Met receptor system and appears to promote synaptogenesis.
I include Dihexa here because patients frequently ask about it, but I want to be candid: this is a peptide where the gap between preclinical promise and clinical evidence is particularly wide. I do not currently use Dihexa in my practice.
Anti-Aging and Longevity Peptides
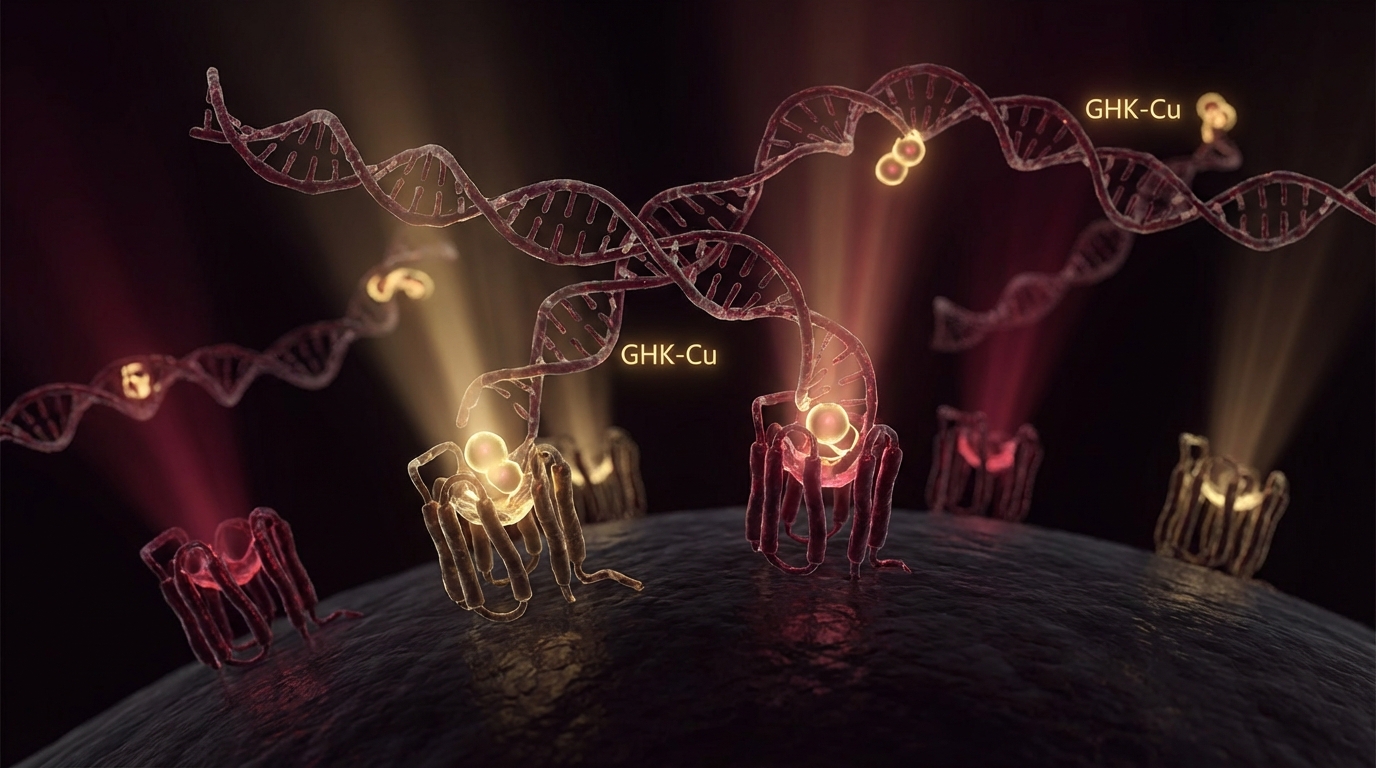
GHK-Cu is a naturally occurring tripeptide with a high affinity for copper ions. It was first identified in human plasma and has been extensively studied for its effects on wound healing, skin remodeling, and anti-inflammatory signaling. A landmark study identified over 4,000 genes whose expression was influenced by GHK-Cu, including genes involved in DNA repair, antioxidant defense, and the ubiquitin-proteasome system.
Epithalon is a synthetic tetrapeptide based on the naturally occurring pineal peptide epithalamin. Its primary proposed mechanism of action is the activation of telomerase — the enzyme that maintains telomere length. The research comes primarily from the laboratory of Professor Vladimir Khavinson at the St. Petersburg Institute of Bioregulation and Gerontology.
I want to be measured in my assessment here. Telomerase activation is a double-edged sword — telomerase is also active in many cancers, and the long-term oncological implications of exogenous telomerase activation are not fully understood.
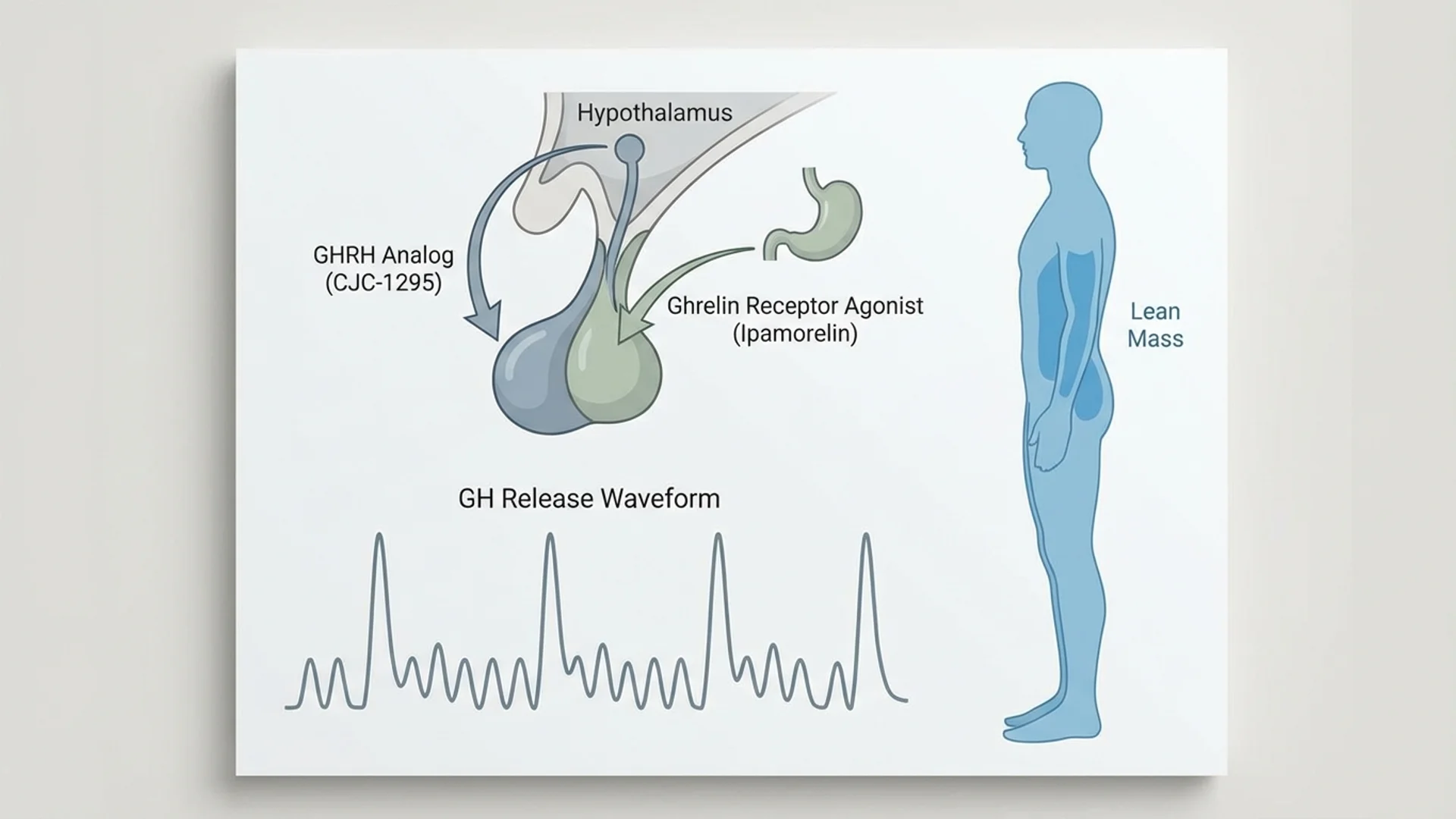
Growth Hormone Secretagogues
This combination represents one of the most commonly used growth hormone secretagogue protocols. CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH), while Ipamorelin is a selective growth hormone secretagogue receptor agonist. Together, they stimulate the pulsatile release of growth hormone from the pituitary gland.
Sleep and Recovery Peptides
DSIP (Delta Sleep-Inducing Peptide)
DSIP is a nine-amino-acid peptide that was originally isolated from the blood of rabbits during electrically induced sleep. Its role in sleep regulation has been studied for decades, though the mechanisms remain incompletely understood.
Unique Mechanism Peptides
While technically a semi-synthetic polysaccharide rather than a peptide, PPS is frequently discussed in the peptide therapy context. It is FDA-approved for interstitial cystitis and has emerging evidence for osteoarthritis treatment through a novel mechanism involving stimulation of cartilage matrix production.
Are Peptides Safe?
This is the question I am asked most frequently, and the honest answer is: it depends on the peptide, the source, the dose, the duration, and the patient.
What We Know
Certain peptides have well-established safety profiles. Thymosin alpha-1 has been used in millions of patients across dozens of countries with a safety record that compares favorably to most pharmaceuticals. Insulin, arguably the most widely used peptide therapeutic, has a century of clinical experience behind it.
For other peptides, particularly those used off-label or obtained from compounding pharmacies, the safety data is more limited. BPC-157 has no reported serious adverse events in the published literature, but the published literature consists almost entirely of animal studies and short-term human observations. Absence of evidence is not evidence of absence.
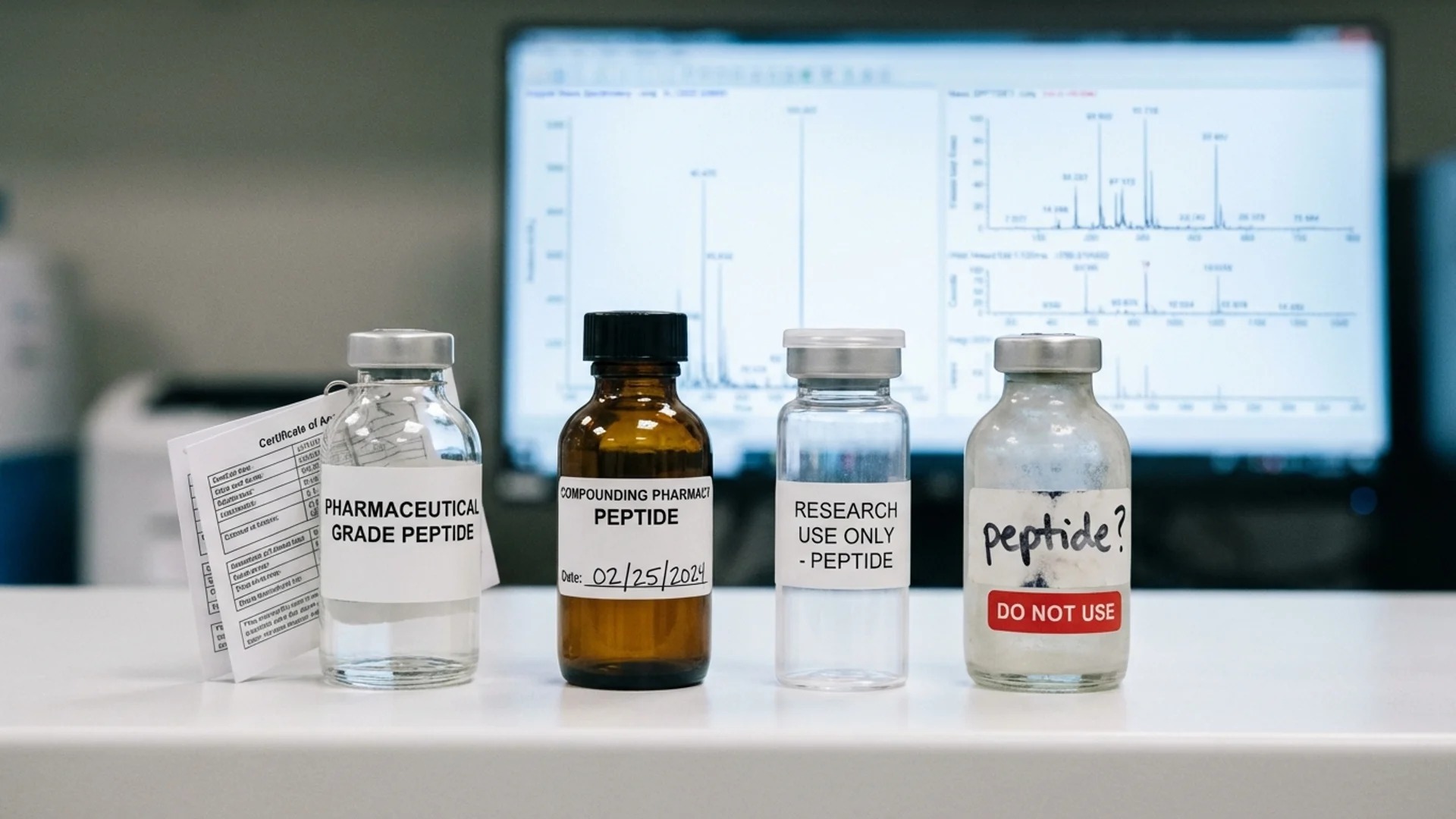
Quality and Sourcing
The quality issue deserves particular emphasis. When a patient obtains a peptide from a regulated pharmaceutical manufacturer, they can have reasonable confidence in purity, sterility, and accurate concentration. When peptides are obtained from compounding pharmacies, the quality depends entirely on the pharmacy’s manufacturing standards. And when peptides are purchased from online “research chemical” suppliers — which, regrettably, is common — quality assurance is essentially nonexistent.
I have seen laboratory analyses of peptides purchased from gray-market sources that showed contamination with bacterial endotoxins, degradation products, and in some cases entirely the wrong peptide. This is not a theoretical concern. It is a documented, practical problem that puts patients at risk.
For a deeper discussion of these issues, see my articles on Peptide Safety and Peptide Sourcing.
Regulatory Landscape
The regulatory status of therapeutic peptides is complex and evolving. In the United States, the FDA has moved in recent years to restrict the compounding of certain peptides, including BPC-157 and several growth hormone secretagogues. In Europe, the regulatory framework varies by country. In other jurisdictions, some of these same peptides are approved pharmaceuticals.
What I tell my patients is this: regulatory status and therapeutic value are not the same thing. A peptide can be therapeutically valuable and not yet approved, or approved and of limited therapeutic value. But regulatory status does matter for quality assurance, legal access, and insurance coverage, and patients should make informed decisions with full knowledge of the regulatory context in their jurisdiction.
Research Gaps
The most significant gap in the peptide literature is the absence of long-term safety data for most therapeutic peptides. We have decades of safety data for insulin, for growth hormone, for some of the established peptide pharmaceuticals. But for many of the peptides that have entered clinical practice in the last decade, our long-term safety understanding is based on mechanistic reasoning and relatively short observation windows.
This does not mean these peptides are unsafe. It means we are operating with incomplete information, and both physicians and patients should acknowledge this honestly.
How I Use Peptides in Practice
My approach to peptide therapy is guided by several principles.
First, peptides are never the starting point. Before I consider peptide interventions, I want to understand the patient’s underlying condition, their metabolic and immune status, their nutritional foundations, and their exposure history. Peptides are modulators — they work best when the system they are modulating has been otherwise optimized.
Second, I match the peptide to the pathophysiology. A patient with chronic Lyme disease and documented immune exhaustion has a clear mechanistic rationale for thymosin alpha-1. A patient recovering from a tendon injury has a rationale for BPC-157 and TB-500. I do not prescribe peptides based on popularity or patient request alone.
Third, I am transparent about the evidence. I tell patients when we are working with robust clinical trial data, when we are extrapolating from animal models, and when we are relying on clinical observation. Patients deserve to make informed decisions, and that requires honesty about what we know and what we do not.
Fourth, I monitor outcomes. Every peptide intervention in my practice is accompanied by appropriate baseline and follow-up assessments. If a patient is receiving thymosin alpha-1 for immune modulation, I want to see their lymphocyte subsets before and after. If we are using a metabolic peptide, I want to track relevant biomarkers. Clinical impression is valuable, but measurable outcomes are better.
Fifth, I use pharmaceutical-grade sources. I will not prescribe or administer peptides whose provenance I cannot verify. This limits the peptides available in my practice to those I can source through regulated channels — a constraint I accept willingly in exchange for confidence in what I am giving my patients.
In the context of our work at Klinik St. Georg, peptides are integrated into broader treatment protocols for chronic infections, post-COVID recovery, oncological support, and longevity medicine. They are one tool among many — alongside hyperthermia, apheresis, IV therapies, and the full diagnostic and therapeutic capabilities of a multidisciplinary hospital. That integrative context is, I believe, where peptides deliver the most value.
Understanding the Evidence Hierarchy
When I discuss the evidence for any therapeutic intervention with patients, I use a framework that distinguishes between different levels of evidence:
Level 1: Randomized Controlled Trials (RCTs) and Meta-Analyses. This is the gold standard. When multiple well-designed RCTs consistently show that an intervention works, we can have high confidence in its efficacy. Very few therapeutic peptides have this level of evidence, with thymosin alpha-1 being a notable exception.
Level 2: Controlled Human Studies. Smaller clinical trials, often open-label or with limited controls. These provide meaningful human data but are more susceptible to bias. GHK-Cu for topical applications falls into this category.
Level 3: Animal Studies and Mechanistic Research. The bulk of the peptide literature sits here. Animal models provide valuable mechanistic insight and safety signals, but the translation from mouse to human is uncertain. BPC-157 is the paradigmatic example — extensive animal data, very limited controlled human data.
Level 4: Clinical Observation and Case Reports. Individual physician experience and patient reports. Valuable for hypothesis generation and for identifying signals that deserve formal study, but subject to selection bias, placebo effects, and confounding variables.
Level 5: Mechanistic Reasoning. “This peptide activates pathway X, and pathway X is involved in condition Y, therefore this peptide should help with condition Y.” Logical, but frequently wrong. Biology is more complex than any single pathway model.
When I recommend a peptide intervention, I tell patients where on this hierarchy the supporting evidence sits. This is not to discourage them — many important medical advances began with Level 3 and 4 evidence. It is to ensure that expectations are calibrated to reality.
Related Reading
- BPC-157: What the Research Actually Shows — Deep dive on the most discussed tissue repair peptide
- TB-500: Thymosin Beta-4 for Tissue Repair — Cell migration and wound healing peptide
- Thymosin Alpha-1: The Immune Modulator with Real Data — The peptide with the strongest evidence base
- Peptide Safety: What You Need to Know — Risks, regulatory status, and physician oversight
- Peptide Sourcing: Hospital-Grade vs. Grey Market — Quality issues and what to look for
- Peptide Therapy for Lyme Disease — How peptides complement standard Lyme treatment
- Peptide Therapy for Gut Healing — BPC-157, KPV, and LL-37 for gastrointestinal repair
- Peptide Therapy for Recovery and Performance — BPC-157 and TB-500 for injury and surgical recovery
References
- Sikiric P, et al. “Brain-gut Axis and Pentadecapeptide BPC 157: Theoretical and Practical Implications.” Curr Neuropharmacol. 2016;14(8):857-865.
- Sikiric P, et al. “Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL 14736, Pliva, Croatia).” Ann N Y Acad Sci. 2006;1070:324-340.
- Goldstein AL, et al. “Thymosin alpha 1: isolation and sequence analysis of an immunologically active thymic polypeptide.” Proc Natl Acad Sci USA. 1977;74(2):725-729.
- Garaci E, et al. “Thymosin alpha 1 in the treatment of cancer: from basic research to clinical application.” Int J Immunopharmacol. 2000;22(12):1067-1076.
- Pickart L, Vasquez-Soltero JM, Margolina A. “GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration.” Biomed Res Int. 2015;2015:648108.
- Khavinson VK, et al. “Peptide Epitalon activates chromatin at the old age.” Neuro Endocrinol Lett. 2003;24(5):329-333.
- Lee C, et al. “The mitochondrial-derived peptide MOTS-c promotes metabolic homeostasis and reduces obesity and insulin resistance.” Cell Metab. 2015;21(3):443-454.
- Sosne G, et al. “Thymosin beta 4: a potential novel therapy for neurotrophic keratopathy, dry eye, and ocular surface diseases.” Vitam Horm. 2016;102:277-306.
- Uchida S, et al. “Dihexa, a brain-penetrant angiotensin IV analog, enhances cognition in rats.” Pharmacol Biochem Behav. 2014;118:16-21.
- Kozlov VA, et al. “Selank and its metabolic fragment Thr-Lys-Pro: mechanisms of action and review of preclinical and clinical studies.” Curr Protein Pept Sci. 2019;20(7):615-625.
Disclaimer: This article is intended for educational purposes and reflects one physician’s perspective on the current state of peptide therapy. It should not be construed as medical advice. Peptide therapy should only be undertaken under the supervision of a qualified physician. Regulatory status and availability of specific peptides vary by jurisdiction.