Topic
Supplements
Evidence-based supplement guidance from clinical practice. What works, what does not, proper dosing, interactions, and the difference between hospital-grade and consumer products.
Explore by Topic
Vitamin D
Beyond bone health — immune modulation, mood, and the optimal range debate.
Magnesium
Forms, dosing, and the widespread deficiency most physicians overlook.
Omega-3 Fatty Acids
EPA/DHA dosing, sources, and the anti-inflammatory evidence.
NAC (N-Acetyl Cysteine)
Glutathione precursor with evidence across respiratory, psychiatric, and liver health.
CoQ10
Mitochondrial electron carrier — critical for statin users and energy metabolism.
Curcumin
Anti-inflammatory bioavailability challenge and the formulations that actually work.
Probiotics
Strain-specific evidence, when they help, when they do not, and what to look for.
Quercetin
Senolytic, antihistamine, and zinc ionophore properties — what the evidence shows.
Berberine
AMPK activator with metformin-comparable glucose-lowering effects.
Free Guide
The Evidence-Based Supplement Guide
Download the complete physician's guide. Evidence-based, no hype.
All Articles
35 articles
Mistletoe Therapy (Iscador): Evidence in Integrative Oncology
Mistletoe extract (Iscador, Helixor) for cancer: mechanism, NK cell activation, quality of life evidence, injection protocols, and the German clinical tradition.
Nattokinase and Serrapeptase for Biofilm Disruption
How proteolytic enzymes nattokinase and serrapeptase degrade biofilm matrix components — mechanism, dosing, evidence, and clinical considerations.
Metformin vs. Berberine: AMPK Activators Compared
Head-to-head comparison of metformin and berberine for longevity, AMPK activation, blood sugar, and exercise compatibility. Evidence, dosing, and which to choose.
NAD+ IV vs NMN vs NR: Which NAD Precursor Is Best?
NAD+ IV, NMN, and NR compared by a physician. Bioavailability, evidence, cost, and who benefits from which approach based on clinical experience.
Best Supplements for Deep Sleep: Evidence Ranked
Physician-ranked guide to sleep supplements. Magnesium glycinate, glycine, apigenin, L-theanine, and ashwagandha compared by evidence quality for deep sleep enhancement.
Integrative Oncology: What It Is and What It Is Not
A clinician's guide to integrative oncology. What complementary therapies have evidence, how they work alongside conventional treatment, and what 35 years of clinical experience at Klinik St. Georg have shown.
Epithalon vs NMN: Anti-Aging Mechanisms Compared
Epithalon vs NMN comparison by Dr. Julian Douwes. Telomere lengthening vs NAD+ replenishment — different aging hallmarks, different evidence, and when to use each.
LL-37 and Vitamin D: The Immune Connection
How vitamin D regulates LL-37 production and why this matters for immunity. The cathelicidin pathway, optimal levels, and clinical implications.

Ashwagandha: Cortisol, Thyroid, and Evidence-Based Dosing
Evidence-based guide to ashwagandha. Cortisol reduction, thyroid effects, dosing, extract types, safety, and what the clinical data actually shows.
Berberine Dosage for Blood Sugar: Evidence-Based Protocol
Physician guide to berberine dosing for blood sugar, insulin sensitivity, and metabolic health. Optimal doses, timing, GI management, and comparison to metformin.
Berberine vs Metformin: AMPK Activation Compared
Head-to-head comparison of berberine and metformin for glucose control, lipids, and longevity. Both activate AMPK — but how do they really compare?
CoQ10: Ubiquinol vs Ubiquinone — What Actually Matters
Evidence-based guide to CoQ10 supplementation. Ubiquinol vs ubiquinone, absorption differences, statin interactions, mitochondrial function, and what I recommend in clinical practice.
CoQ10 Dosage by Condition: Heart, Fertility, Migraines, and Energy
Physician guide to CoQ10 dosing by condition. Ubiquinol vs ubiquinone, heart health, male fertility, migraine prevention, energy, and statin users. Evidence-based protocols.
CoQ10 for Statin Users: Why Your Cholesterol Medication Depletes CoQ10
Physician guide to CoQ10 depletion from statins. Why it happens, symptoms of statin-induced CoQ10 deficiency, optimal dosing with ubiquinol, and what the evidence shows.
Curcumin: Why Most Supplements Don't Work and Which Ones Do
The bioavailability problem with curcumin explained. Comparing Meriva, Longvida, BCM-95, Theracurmin, liposomal, and piperine forms. Dosing by condition.

Best Curcumin Supplements for Absorption: Meriva, BCM-95, Theracurmin, and Piperine Compared
Physician comparison of curcumin formulations for absorption. Meriva, BCM-95, Theracurmin, NovaSOL, and piperine ranked by bioavailability data, clinical evidence, and cost.
Curcumin for Joint Pain and Arthritis: Dosage, Timeline, and What the Meta-Analyses Show
Evidence-based curcumin dosing for joint pain and arthritis. Meta-analysis results, comparison to NSAIDs, best formulations, timeline to improvement, and physician protocols.

Curcumin vs. Turmeric Supplements: Why the Spice Alone Is Not Enough
Physician guide to curcumin vs turmeric supplements. Why turmeric spice has poor bioavailability, how curcumin extracts differ, and what to look for in a supplement.
Fish Oil vs. Krill Oil vs. Algae Oil: Which Omega-3 Source Is Best?
Physician comparison of fish oil, krill oil, and algae oil for omega-3 supplementation. EPA and DHA content, absorption, sustainability, cost, and evidence-based recommendations.

Lion's Mane: Nerve Growth Factor and Cognitive Benefits
Evidence-based guide to lion's mane mushroom for brain health. NGF stimulation, cognitive benefits, dosing, extract types, and what the clinical data supports.

Magnesium Deficiency Symptoms: The Warning Signs Most People Miss
Physician guide to magnesium deficiency symptoms including muscle cramps, insomnia, anxiety, heart palpitations, and fatigue. Testing, causes, and how to correct it.

Magnesium Glycinate vs. L-Threonate: Which Form for Sleep, Anxiety, and Brain Health?
Physician comparison of magnesium glycinate vs magnesium L-threonate. Which form for sleep, which for cognition, absorption differences, dosing, and evidence quality.

When to Take Magnesium: Morning vs. Night, With or Without Food
Physician guide to magnesium supplement timing. When to take glycinate, threonate, citrate, and other forms for maximum absorption and effect. Morning vs night, food interactions.
NAC (N-Acetyl Cysteine): The Most Underrated Supplement in Medicine
NAC N-acetyl cysteine benefits reviewed by a physician. Glutathione precursor, psychiatric uses, liver protection, COVID research, and dosing from 600-1800mg.

NAC Dosage Guide: How Much to Take for Liver, Lungs, and Immune Support
Evidence-based NAC dosing by condition. Liver support, respiratory health, immune function, mental health, and general antioxidant use. Physician-guided protocols.
NAC for Fertility: How N-Acetyl Cysteine Supports Reproductive Health
Evidence-based guide to NAC for fertility in men and women. PCOS, ovulation, sperm quality, oxidative stress, and dosing protocols from clinical trials.
NAC vs. Glutathione: Which Antioxidant Should You Take?
Physician comparison of NAC vs glutathione supplements. Oral bioavailability, mechanisms, when to use each, liposomal glutathione, and evidence-based recommendations.
Nattokinase: The Fibrinolytic Enzyme for Microclots
Evidence-based guide to nattokinase for fibrinolysis and microclots. Mechanism, dosing, post-COVID relevance, combination with serrapeptase, and safety with blood thinners.
Omega-3 Dosage for Inflammation: EPA and DHA for Joints, Brain, and Heart
Evidence-based omega-3 dosing for inflammation. How much EPA and DHA for joint pain, cardiovascular inflammation, neuroinflammation, and autoimmune conditions. Physician protocols.
Probiotics: Matching the Right Strain to the Right Condition
Evidence-based guide to probiotic strain selection. Which strains work for which conditions, when to avoid probiotics, CFU counts, spore-based vs traditional, and what I use in clinical practice.
Best Probiotic Strains by Condition: IBS, Bloating, Immunity, and Mood
Physician guide to evidence-based probiotic strain selection. Which specific strains work for IBS, bloating, immunity, mood, and vaginal health, with dosing and evidence grades.

How to Choose a Probiotic: CFU Count, Strains, and What Actually Matters
Physician guide to choosing a probiotic supplement. CFU count myths, strain identification, delivery mechanisms, third-party testing, and what the label should tell you.

Probiotics vs. Prebiotics vs. Postbiotics: What the Difference Means for Your Gut
Physician guide to probiotics, prebiotics, postbiotics, and synbiotics. Definitions, mechanisms, when to use each, and how they work together for gut health.
Quercetin as a Senolytic: Protocol, Dosage, and What the Research Shows
Physician guide to quercetin senolytic protocols. Quercetin + dasatinib evidence, quercetin + fisetin alternatives, dosing schedules, and the science of clearing senescent cells.

When to Take Supplements: The Complete Timing Guide
Evidence-based supplement timing guide. Fat-soluble vitamins with meals, magnesium at night, iron on an empty stomach, and how to build morning and evening stacks based on pharmacokinetics.
Complete Guide
The Physician's Guide to Supplements
In-depth reference by Dr. Julian Douwes
Why a Physician Writes About Supplements
Most supplement information falls into two camps: uncritical marketing (“this will change your life”) or blanket dismissal (“supplements are expensive urine”). Neither serves patients well.
I prescribe supplements daily — in a hospital setting, monitored with laboratory testing, adjusted based on response. I also see the damage from unguided supplementation: patients spending hundreds monthly on products that interact with their medications, contain contaminants, or simply do not work.
This guide bridges that gap. Evidence-graded. Honest about limitations. Written by someone who uses these tools clinically.
Evidence Grading System
Every supplement recommendation on this platform uses a five-tier system:
| Level | Meaning | Example |
|---|---|---|
| Strong | Multiple RCTs, meta-analyses | Vitamin D for immune function, omega-3 for inflammation |
| Moderate | Limited RCTs, consistent observational data | CoQ10 for statin users, NAC for glutathione support |
| Emerging | Preclinical evidence strong, human trials early | NMN for NAD+ restoration, fisetin as senolytic |
| Traditional | Historical clinical use, limited modern trials | Andrographis for infection, milk thistle for liver |
| Insufficient | Marketed but unproven | Most “detox” supplements, many nootropic stacks |
Quality: The First Question
Before asking “what should I take?” ask “what am I actually taking?”
The Quality Problem
The supplement industry operates under far less regulatory scrutiny than pharmaceuticals. The FDA does not pre-approve supplements for safety or efficacy. Third-party testing consistently finds products that contain less active ingredient than labeled, contain contaminants, or contain entirely the wrong compound.
What to Look For
- Third-party testing: USP Verified, NSF Certified for Sport, or ConsumerLab approved
- GMP certification: Not just compliance (legally required) but actual third-party audit
- Form matters: Magnesium oxide (poorly absorbed) vs. magnesium glycinate (well absorbed). Ubiquinone vs. ubiquinol. Folic acid vs. methylfolate.
- Practitioner-grade lines: Thorne, Pure Encapsulations, Designs for Health, Klaire Labs maintain higher standards than mass-market brands
The German Advantage
In Germany, products like mistletoe extract (Iscador, Helixor) and systemic enzyme therapy (Wobenzym) are approved pharmaceuticals — not “alternative supplements.” They undergo drug-level manufacturing oversight and clinical testing. This regulatory distinction matters.
Core Categories
Vitamins
Vitamin D3 + K2 — The most commonly deficient nutrient in chronically ill patients. We target serum 25(OH)D of 40-60 ng/mL. K2 (MK-7) directs calcium to bones, preventing vascular calcification. A 2025 DKFZ meta-analysis found 20% mortality reduction in deficient cancer cohorts. Always test before dosing. Evidence: Strong.
B-Complex (methylated) — Methylcobalamin, methylfolate, P-5-P, riboflavin-5-phosphate. Essential for energy metabolism, methylation, and neurotransmitter synthesis. Critical for MTHFR variant carriers. Evidence: Strong for deficiency.
High-Dose IV Vitamin C — At pharmacologic levels (achievable only via IV), vitamin C acts as a pro-oxidant selectively cytotoxic to cancer cells. A Phase 2 RCT showed doubling of overall survival in metastatic pancreatic cancer. Requires G6PD screening. Fundamentally different from oral supplementation. Evidence: Moderate-Strong for oncology.
Minerals
Magnesium — Cofactor in 300+ enzymatic reactions. A 2026 RCT showed magnesium L-threonate supplementation associated with 7.5-year cognitive age reduction. Six forms for six purposes: glycinate (sleep), L-threonate (cognition), malate (energy), taurate (cardiovascular), citrate (bowel motility), oxide (avoid — low bioavailability). Evidence: Strong.
Zinc — Essential for T-cell maturation and immune function. 15-30 mg/day. Long-term use requires copper co-supplementation. Evidence: Moderate.
Selenium — Required for glutathione peroxidase and thyroid hormone conversion. 200 mcg/day selenomethionine. Narrow therapeutic window — excess is toxic. Evidence: Moderate.
Antioxidants and Mitochondrial Support
NAC (N-Acetylcysteine) — Glutathione precursor (4-fold synthesis increase). Mucolytic. Biofilm disruptor. Used in our Lyme protocols for both detoxification support and biofilm disruption. 600-1,800 mg/day. Evidence: Moderate-Strong.
Glutathione — The master antioxidant. IV delivery bypasses poor oral absorption. Liposomal and S-acetyl forms improve oral bioavailability. Lyme patients frequently exhibit depleted glutathione. Evidence: Moderate.
CoQ10 — Mitochondrial electron transport chain cofactor. Ubiquinol form better absorbed. Combined with alpha-lipoic acid, a prospective study showed substantially reduced fatigue in chronic COVID patients. Essential for statin users. Evidence: Moderate.
Fatty Acids
Omega-3 (EPA/DHA) — Anti-inflammatory through resolvin and protectin synthesis. Decreased omega-3 levels documented in CFS patients. Triglyceride form outperforms ethyl ester for bioavailability. Test with omega-3 index (target 8-12%). Quality varies enormously — check TOTOX values and heavy metal testing. Evidence: Strong.
Herbal and Botanical
Curcumin — NF-kB inhibition, anti-inflammatory, anti-proliferative. Bioavailability is the challenge — requires piperine, liposomal, or phytosome formulation. Evidence: Moderate.
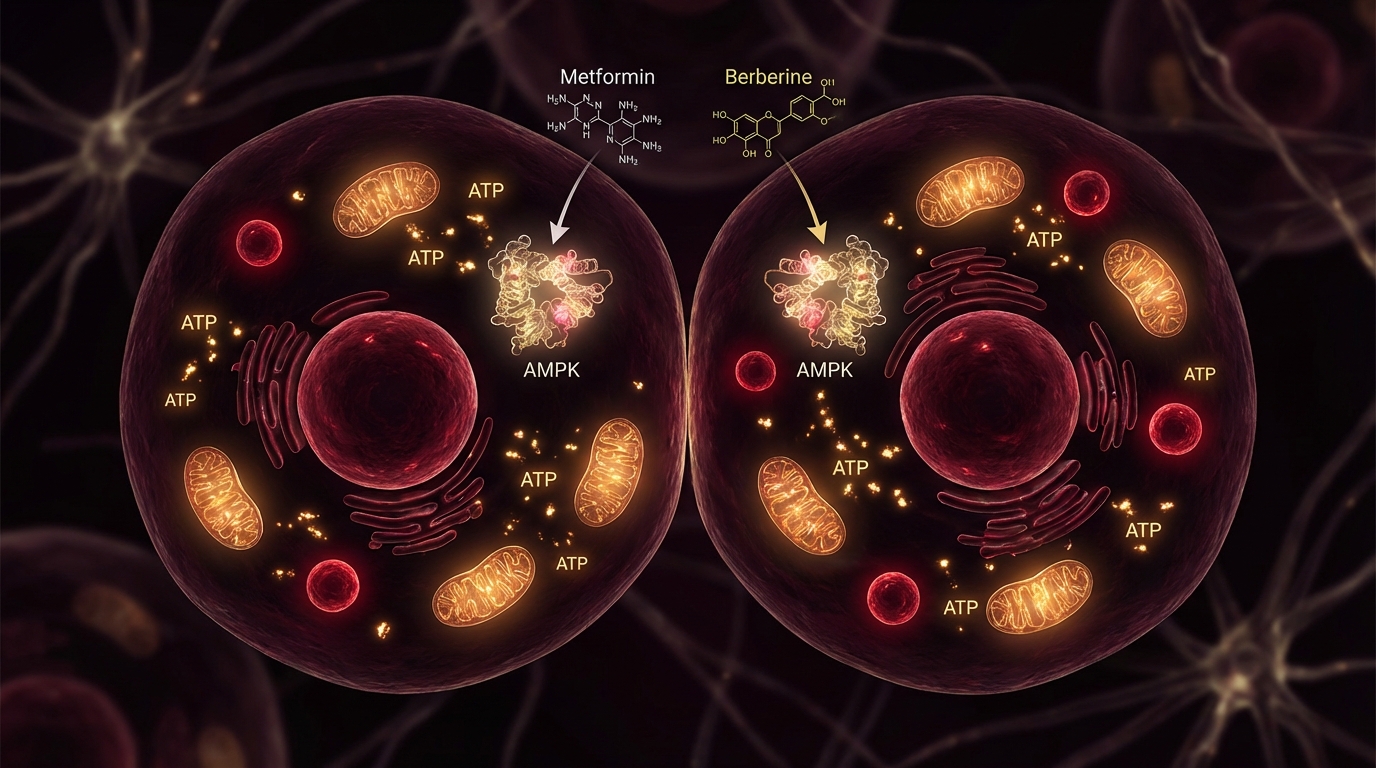
Berberine — AMPK activator (same pathway as metformin), antimicrobial, glucose regulation. Emerging evidence as PD-L1 checkpoint inhibitor with immunomodulatory actions. Evidence: Moderate.
Mistletoe Extract — Immunostimulation through lectins activating NK cells and T-cells. Approved as cancer therapy in Germany. 62% of oncology patients in German studies received mistletoe. Phase I trial at Johns Hopkins established safety. Evidence: Moderate (European standard of care for integrative oncology).
Ashwagandha — HPA axis regulation. A 2025 meta-analysis confirmed statistically significant cortisol reduction (15-30%) and anxiety improvement. Evidence: Strong for stress/cortisol.
Enzymes and Fibrinolytics
Nattokinase — Fibrinolytic enzyme. A 2024 study showed 84% microclot reduction in vitro. Directly relevant to Dr. Beate Jaeger’s microclot research in Post-COVID. RCT found enzyme + probiotic combination achieved 91% fatigue-free status in Post-COVID at 14 days. Evidence: Emerging.
Wobenzym — German pharmaceutical. Combination of bromelain, trypsin, papain, and rutin. Meta-analysis confirmed non-inferiority to diclofenac for knee osteoarthritis with better safety profile. Evidence: Moderate.
Longevity Compounds
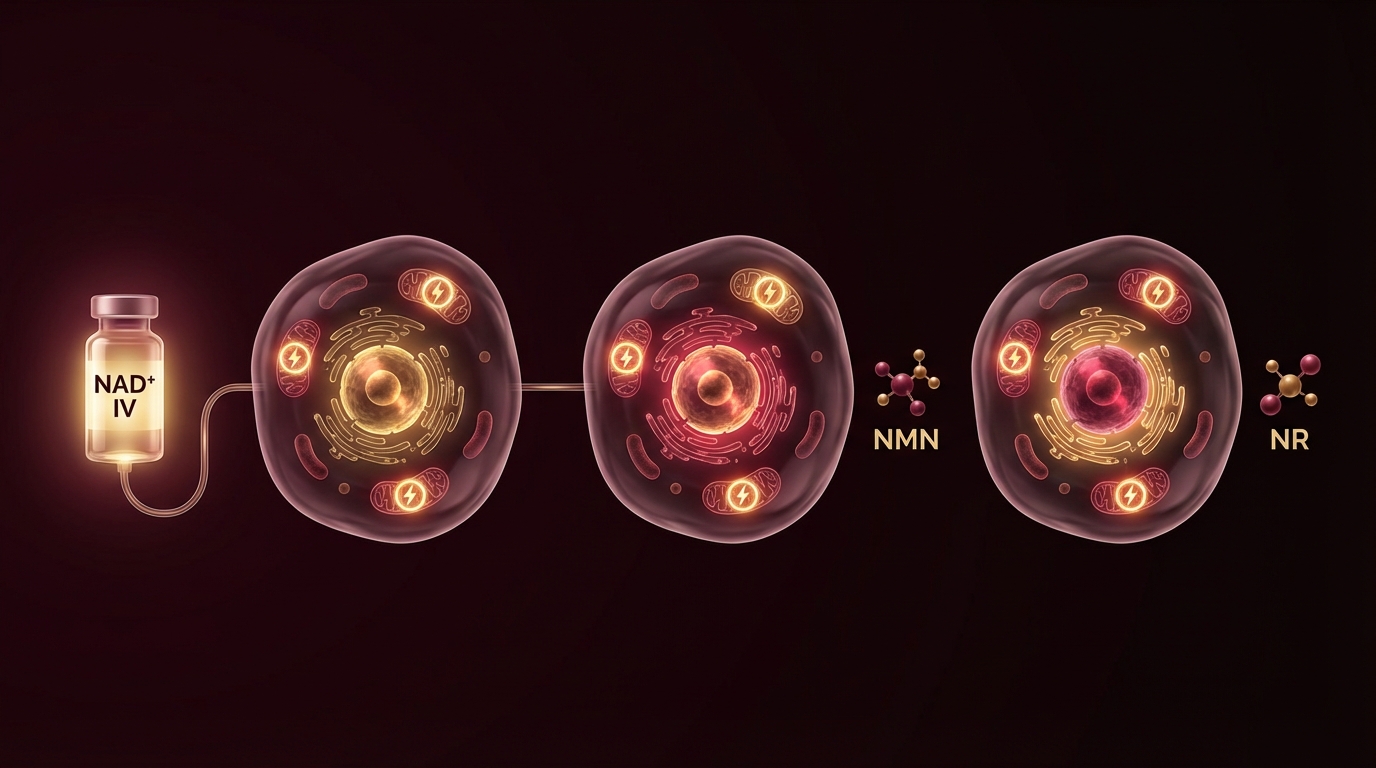
NMN/NR — NAD+ precursors. January 2026 RCT showed both double circulating NAD+ levels. NMN reduced inflammatory signals post-exercise (February 2026 RCT). FDA confirmed NMN remains available as dietary supplement (September 2025). Important caveat: lifespan extension NOT proven in humans. Evidence: Emerging.
Quercetin — Senolytic (clears senescent “zombie cells”), anti-inflammatory, mast cell stabilizer. Quercetin + dasatinib is the most studied senolytic combination. Evidence: Moderate for anti-inflammatory, Emerging for senolytic.
Drug-Supplement Interactions
This is the section most supplement guides skip. Critical interactions:
- Omega-3 + anticoagulants — Additive bleeding risk at high doses (>3g/day)
- Curcumin + chemotherapy — May interfere with certain agents; timing matters
- St. John’s Wort + practically everything — Potent CYP450 inducer
- NAC + nitroglycerin — Potentiates hypotension
- Vitamin K2 + warfarin — Alters INR (consistent intake is key, not avoidance)
- Berberine + metformin — Additive glucose lowering (monitor closely)
- Ashwagandha + thyroid medication — May increase thyroid hormone levels
- Quercetin + cyclosporine — Increases drug levels
Always disclose your full supplement list to every prescribing physician.
Supplements to Stop Before Treatment
If you are coming to St. George Hospital for treatment, we will provide specific guidance. General principles:
- 7-14 days before surgery: Stop omega-3, vitamin E, ginkgo, garlic supplements (bleeding risk)
- Before apheresis: Stop nattokinase/serrapeptase (fibrinolytic overlap)
- Before immunotherapy: Discuss antioxidants (theoretical concern about reducing treatment efficacy)
- Before hormone-sensitive procedures: Pause DIM, I3C, maca, DHEA
Building Your Stack
The most common mistake is starting with advanced compounds before establishing foundations. Our approach:
Foundation (everyone): Vitamin D3+K2, magnesium, omega-3, B-complex, probiotics. Test, dose, and verify.
Condition-specific (guided by labs): NAC for glutathione support, CoQ10 for mitochondrial function, zinc for immune support, curcumin for inflammation. Add based on diagnostic findings, not marketing.
Advanced (physician-supervised): NMN/NR for NAD+ restoration, senolytic protocols, peptides, IV formulations. These require monitoring and medical oversight.
Start with fewer, higher-quality supplements rather than more, cheaper ones. Test before and after. If a supplement isn’t moving your biomarkers in the right direction within 90 days, stop it.