If you want to intervene in aging, you need a map. Not a list of supplements. Not a podcast recommendation. A map — a systematic framework that tells you what is going wrong, where it is going wrong, and which interventions target which processes.
The hallmarks of aging provide that map. First proposed by Lopez-Otin and colleagues in 2013 and updated in January 2023 to include 12 hallmarks, this framework is the closest thing longevity medicine has to a periodic table [1]. Every serious longevity intervention — from rapamycin to senolytics to NAD+ precursors — can be mapped to specific hallmarks it targets. Every meaningful biomarker can be connected to a hallmark it measures.
In my clinical practice, the hallmarks framework is how I think about longevity. Not as a single intervention, but as 12 interconnected targets. Here is what each hallmark is, how I measure it, and what my clinical toolbox offers against it.
At a Glance
| Property | Value |
|---|---|
| Evidence Level | Strong (foundational framework, extensive supporting literature) |
| Primary Use | Systematic framework for understanding and targeting biological aging |
| Key Mechanism | 12 interconnected cellular and systemic processes that drive age-related decline |
The Architecture of Aging
The 2023 update organizes the 12 hallmarks into three categories [1]:
Primary hallmarks (causes of cellular damage):
- Genomic instability
- Telomere attrition
- Epigenetic alterations
- Loss of proteostasis
- Disabled macroautophagy
Antagonistic hallmarks (responses to damage): 6. Deregulated nutrient sensing 7. Mitochondrial dysfunction 8. Cellular senescence
Integrative hallmarks (systemic consequences): 9. Stem cell exhaustion 10. Altered intercellular communication 11. Chronic inflammation 12. Dysbiosis
This hierarchy matters clinically. Primary hallmarks are upstream causes. Antagonistic hallmarks are the body’s initially protective responses that become harmful over time. Integrative hallmarks are the systemic consequences that ultimately produce the clinical features we associate with aging. Intervening upstream produces broader effects than treating downstream symptoms.
1. Genomic Instability
What It Is
Your DNA accumulates damage throughout life — from oxidative stress, radiation, replication errors, and environmental toxins. Normally, DNA repair mechanisms fix most damage. With aging, repair capacity declines while damage accumulates. The result: somatic mutations, chromosomal aberrations, and gene expression errors that impair cellular function [2].
How to Measure It
- 8-OHdG (8-hydroxy-2’-deoxyguanosine): A urinary marker of oxidative DNA damage. Elevated levels indicate increased genomic stress.
- Gamma-H2AX foci: Research-grade assay that quantifies DNA double-strand breaks. Not widely available clinically but the gold standard.
- Micronucleus assay: Detects chromosomal instability in peripheral blood lymphocytes.
What Targets It
- NAD+ precursors (NMN, NR): NAD+ is required by PARP enzymes for DNA repair. Declining NAD+ levels impair repair capacity. NAD+ IV therapy directly replenishes this critical cofactor.
- Antioxidant optimization: Not mega-dose supplementation — targeted optimization of glutathione, SOD, and catalase systems.
- Environmental toxin reduction: Heavy metals, mold toxins, and persistent organic pollutants accelerate genomic damage. Diagnostics identify burden; detoxification protocols reduce it.
2. Telomere Attrition
What It Is
Telomeres are the protective caps at the ends of chromosomes. They shorten with each cell division and with oxidative stress. When telomeres reach a critical length, cells enter senescence or apoptosis. Shortened telomeres are associated with virtually every age-related disease [3].
How to Measure It
- Telomere length testing: Available via qPCR or Flow-FISH methods. I use this as part of baseline biological age assessment. Single measurements are less informative than serial measurements over time.
- Context matters: Telomere length is one biomarker, not a death sentence. Short telomeres in the context of good epigenetic age and low inflammation are very different from short telomeres with accelerated biological aging.
What Targets It
- Telomerase activators: TA-65 (cycloastragenol) has modest evidence for telomere maintenance. Epithalon (epitalon) is a peptide that activates telomerase — the evidence is emerging but mechanistically coherent.
- Lifestyle foundations: Exercise, stress management, and adequate sleep are consistently associated with longer telomeres. This is not a platitude — the data is robust.
- Addressing accelerators: Chronic infection (Lyme disease), chronic inflammation, and oxidative stress all accelerate telomere shortening. Treating the root cause matters more than telomere-specific supplements.
I discuss telomere biology and practical interventions in greater detail here.
3. Epigenetic Alterations
What It Is
Epigenetics controls which genes are expressed without changing the DNA sequence itself. The three main epigenetic mechanisms — DNA methylation, histone modifications, and chromatin remodeling — become progressively dysregulated with age. Genes that should be silenced become active. Genes that should be active become silenced. The result is cellular identity loss and functional decline [4].
How to Measure It
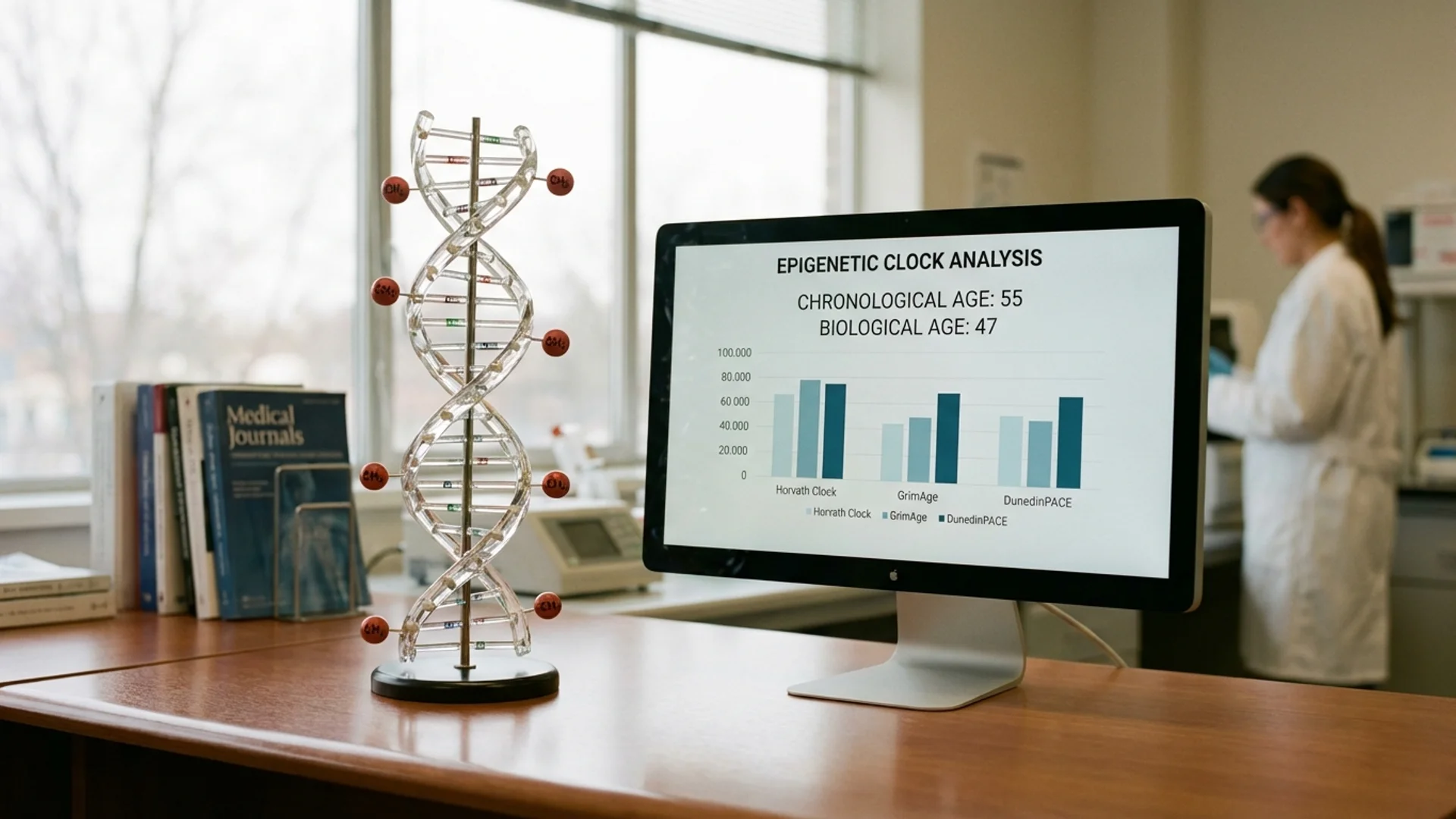
- Epigenetic clocks: The most clinically actionable aging biomarker available today. Horvath, GrimAge, and DunedinPACE clocks measure biological age based on DNA methylation patterns. I use these routinely — they tell me whether a patient is aging faster or slower than their chronological age, and they respond measurably to interventions.
- Serial measurements: A single clock measurement is a snapshot. Measuring at baseline and after intervention (6-12 months) reveals trajectory.
What Targets It
- Rapamycin: Has demonstrated epigenetic age reversal in human studies. I discuss rapamycin in longevity in detail.
- Alpha-ketoglutarate: A metabolite that serves as a cofactor for TET enzymes (DNA demethylation) and Jumonji histone demethylases. Preliminary data shows biological age reduction.
- Methyl donor optimization: Adequate folate, B12, betaine, and choline support proper methylation. This is basic but frequently overlooked.
- Lifestyle: Caloric restriction, exercise, and sleep optimization are the most evidence-backed epigenetic age modifiers.
4. Loss of Proteostasis
What It Is
Cells maintain protein quality through a network of chaperones, the ubiquitin-proteasome system, and autophagy. With age, this network deteriorates. Misfolded proteins accumulate, forming aggregates that impair cellular function. This hallmark is central to Alzheimer’s (amyloid, tau), Parkinson’s (alpha-synuclein), and other neurodegenerative diseases [1].
How to Measure It
- Direct measurement is limited clinically. There is no widely available blood test for proteostasis.
- Proxy markers: Heat shock protein levels (HSP70, HSP90) can indicate chaperone system status. Amyloid PET imaging for neurodegenerative contexts.
- Functional assessment: Cognitive testing and neurological exam as indirect markers of CNS proteostasis.
What Targets It
- Whole-body hyperthermia: Heat stress activates the heat shock response — a powerful upregulation of chaperone proteins that refold damaged proteins and clear aggregates. This is one of the mechanistic reasons hyperthermia has longevity benefits beyond infection treatment. Two sessions at moderate temperature (40 degrees C) stimulate robust HSP expression.
- Autophagy activation: Fasting, rapamycin, and spermidine promote autophagic clearance of damaged proteins (see Hallmark 5).
- Cold and heat exposure protocols: Deliberate thermal stress trains the proteostasis network.
5. Disabled Macroautophagy
What It Is
Autophagy is the cell’s recycling system — it degrades damaged organelles, protein aggregates, and intracellular pathogens. The 2023 update elevated macroautophagy from a component of proteostasis to its own hallmark, reflecting its central importance. Autophagic capacity declines significantly with age, allowing cellular debris to accumulate [1].
How to Measure It
- LC3-II/LC3-I ratio: Research marker for autophagic flux. Not widely available clinically.
- p62/SQSTM1 levels: Accumulation of p62 indicates impaired autophagy.
- Practical proxy: Insulin sensitivity and fasting glucose. Chronic hyperinsulinemia suppresses autophagy via mTOR activation.
What Targets It
- Intermittent fasting: The most accessible autophagy activator. Sixteen to eighteen hours of fasting activates AMPK and inhibits mTOR, both of which promote autophagy. I recommend time-restricted eating as a foundation for virtually all longevity patients.
- Rapamycin: The most potent pharmacological autophagy activator. mTOR is the master switch — inhibiting it with rapamycin directly promotes autophagic flux.
- Spermidine: A naturally occurring polyamine that induces autophagy through multiple mechanisms. Found in wheat germ, aged cheese, and mushrooms. Supplementation at 1-3 mg/day has emerging evidence for longevity benefit.
- Exercise: Both aerobic and resistance training activate autophagy acutely. Regular exercise maintains autophagic capacity.
6. Deregulated Nutrient Sensing
What It Is
Four interconnected nutrient-sensing pathways regulate growth, metabolism, and repair: mTOR (senses amino acids), insulin/IGF-1 signaling (senses glucose), AMPK (senses energy deficit), and sirtuins (sense NAD+). In youth, these systems balance growth with maintenance. With aging and chronic overnutrition, the balance shifts toward persistent growth signaling — promoting cell growth over repair, proliferation over quality control [5].
How to Measure It
- Fasting insulin and HOMA-IR: Direct markers of insulin/IGF-1 pathway status. Fasting insulin above 8 uIU/mL indicates suboptimal nutrient sensing.
- IGF-1 levels: Context-dependent. Very high levels indicate growth-dominant signaling. Very low levels may indicate insufficient repair capacity.
- HbA1c and fasting glucose: Integrated markers of glycemic control.
- These are part of my standard longevity blood panel.
What Targets It
- Caloric restriction and fasting: The most validated longevity intervention across species. Reduces insulin/IGF-1 signaling, activates AMPK, and upregulates sirtuins.
- Rapamycin: Direct mTOR inhibition. The only pharmacological intervention that extends lifespan in every organism tested, from yeast to mammals.
- Metformin: Activates AMPK, reduces hepatic glucose output, and modulates mTOR. The TAME trial is testing its effects on aging in humans.
- NAD+ precursors: Support sirtuin activity. NAD+ declines with age, impairing sirtuin-mediated repair and metabolic regulation.
7. Mitochondrial Dysfunction
What It Is
Mitochondria are the energy factories of every cell. With aging, mitochondrial DNA accumulates mutations, the electron transport chain becomes less efficient, reactive oxygen species (ROS) production increases, and mitochondrial biogenesis declines. The result: reduced cellular energy, increased oxidative damage, and impaired metabolic flexibility [6].
How to Measure It
- Organic acids testing: Markers of mitochondrial metabolic function (citrate, succinate, fumarate ratios).
- Lactate/pyruvate ratio: Elevated ratio suggests impaired mitochondrial oxidative phosphorylation.
- CoQ10 levels: CoQ10 is essential for electron transport chain function and declines with age.
- Cardiopulmonary exercise testing (VO2 max): Functional measure of mitochondrial capacity. VO2 max is one of the strongest predictors of all-cause mortality.
I discuss mitochondrial assessment and optimization in detail here.
What Targets It
- IHHT (Intermittent Hypoxic-Hyperoxic Training): Alternating hypoxia and hyperoxia triggers mitochondrial biogenesis and eliminates dysfunctional mitochondria through mitophagy. This is one of my most frequently prescribed longevity interventions.
- CoQ10 supplementation: 200-400 mg ubiquinol daily supports electron transport chain function.
- Exercise: The most powerful mitochondrial biogenesis stimulus. Both endurance and high-intensity interval training promote mitochondrial quantity and quality.
- NAD+ precursors: Support mitochondrial NAD+ pools required for oxidative phosphorylation and sirtuin-mediated mitochondrial maintenance.
- Methylene blue: An electron carrier that can bypass Complex I and Complex III blockades in the electron transport chain. Investigational for mitochondrial dysfunction.
8. Cellular Senescence
What It Is
When cells accumulate irreparable damage, they enter a state of permanent growth arrest called senescence. Senescent cells do not divide, but they remain metabolically active, secreting a cocktail of inflammatory cytokines, growth factors, and proteases — the senescence-associated secretory phenotype (SASP). This SASP damages surrounding tissue and promotes aging in neighboring cells [7].
How to Measure It
- p16INK4a expression: The most established senescence biomarker, measurable in peripheral blood T cells. Levels increase exponentially with age.
- SASP markers: IL-6, MMP-3, PAI-1 — elevated levels suggest increased senescent cell burden.
- Currently, no single test definitively quantifies senescent cell burden in living humans. This remains a major research gap.
What Targets It
- Senolytics: Dasatinib plus quercetin, fisetin — drugs that selectively kill senescent cells. I discuss the evidence, protocols, and limitations in detail in my dedicated article.
- Whole-body hyperthermia: Heat stress appears to promote clearance of senescent cells, though the mechanism is less well characterized than direct senolytic agents.
- Exercise: Regular physical activity reduces senescent cell markers, likely through immune-mediated clearance (immunosurveillance of senescent cells).
- Fasting: Autophagy, which is activated by fasting, can clear pre-senescent cells before they fully commit to the senescent phenotype.
9. Stem Cell Exhaustion
What It Is
Tissue regeneration depends on resident stem cell populations. With aging, stem cells decline in number and function — reduced self-renewal capacity, increased quiescence, lineage bias (hematopoietic stem cells shift toward myeloid at the expense of lymphoid output, contributing to immunosenescence). The regenerative capacity of every organ system declines as stem cells exhaust [1].
How to Measure It
- Complete blood count with differential: Shifts in myeloid-to-lymphoid ratios can reflect hematopoietic stem cell aging.
- CD34+ stem cell counts: Circulating progenitor cell levels decline with age.
- Functional measures: Wound healing speed, recovery from illness or surgery, exercise recovery capacity.
What Targets It
- Stem cell therapies: Mesenchymal stem cell (MSC) infusions can supplement declining endogenous stem cell populations. The evidence is moderate and context-dependent.
- Hyperbaric oxygen therapy: Has demonstrated increased circulating stem cell mobilization in human studies.
- NAD+ precursors: NAD+ supports stem cell function and self-renewal capacity.
- Exercise: Resistance training and endurance exercise maintain stem cell pools and improve mobilization.
- Peptides: Epithalon and thymosin alpha-1 may support stem cell maintenance, though evidence is early-stage.
10. Altered Intercellular Communication
What It Is
Cells communicate through hormones, cytokines, extracellular vesicles, and direct contact. With aging, this communication network degrades. Hormonal signaling declines (testosterone, estrogen, growth hormone, thyroid). Pro-inflammatory signaling increases. The extracellular matrix stiffens, impairing mechanical signaling. The net result: coordinated tissue function breaks down [1].
How to Measure It
- Comprehensive hormone panel: Testosterone, estradiol, DHEA-S, IGF-1, thyroid (full panel), cortisol rhythm.
- Inflammatory markers: hsCRP, IL-6, TNF-alpha — markers of the age-related shift toward pro-inflammatory signaling (“inflammaging”).
- Extracellular matrix markers: Research-stage assessments of matrix metalloproteinases and collagen crosslinks.
What Targets It
- Hormone optimization: Restoring hormonal communication to physiological levels — not supraphysiological, not youth-chasing, but functional optimization guided by symptoms and labs.
- Anti-inflammatory interventions: From omega-3 fatty acids and specialized pro-resolving mediators to anti-inflammatory protocols targeting NF-kB and NLRP3.
- Peptide therapy: Thymosin alpha-1 for immune communication, BPC-157 for vascular signaling, GHK-Cu for extracellular matrix support.
- Parabiosis-inspired approaches: Plasma exchange (therapeutic plasma exchange/apheresis) to dilute age-related circulating factors — an emerging area with intriguing early data.
11. Chronic Inflammation (Inflammaging)
What It Is
The 2023 update elevated chronic inflammation to its own hallmark — reflecting its central role in driving virtually every age-related disease. Inflammaging is a low-grade, sterile, chronic inflammatory state characterized by elevated circulating cytokines, activated innate immune cells, and impaired resolution of inflammation. It is both a consequence of other hallmarks (senescent cell SASP, gut dysbiosis, mitochondrial damage) and a driver of further aging [8].
How to Measure It
- hsCRP: The most accessible marker. Levels below 0.5 mg/L are optimal. Above 1.0 consistently indicates meaningful chronic inflammation.
- IL-6: More specific than CRP for inflammaging. Elevated IL-6 is one of the strongest predictors of all-cause mortality in the elderly.
- TNF-alpha, IL-1beta: Additional inflammatory cytokines that characterize the inflammaging phenotype.
- Neutrophil-to-lymphocyte ratio (NLR): Simple, inexpensive, and surprisingly predictive of inflammatory burden and mortality risk.
What Targets It
Virtually everything in the longevity medicine toolbox targets inflammation, because it is downstream of multiple hallmarks. The question is which upstream driver is primary:
- If driven by senescence: Senolytics
- If driven by gut dysbiosis: Microbiome restoration (see Hallmark 12)
- If driven by chronic infection: Treat the infection — Lyme, reactivated viruses, chronic EBV
- If driven by mitochondrial dysfunction: IHHT, CoQ10, exercise
- If driven by metabolic dysfunction: Address insulin resistance, optimize nutrient sensing
The worst approach is simply suppressing inflammation with NSAIDs or steroids without identifying the driver. That is treating the smoke alarm, not the fire.
12. Dysbiosis
What It Is
The newest hallmark, added in the 2023 update. The gut microbiome changes substantially with aging: microbial diversity decreases, beneficial species decline (Bifidobacteria, Akkermansia, Faecalibacterium), and pathobionts increase. The aged microbiome produces fewer short-chain fatty acids, weakens the intestinal barrier, and shifts immune signaling toward pro-inflammatory patterns. Fascinatingly, transferring a young microbiome to aged mice extends lifespan and improves brain function — establishing causation, not just correlation [9].
How to Measure It
- Comprehensive microbiome sequencing: Shotgun metagenomic sequencing provides species-level identification and functional pathway analysis. I use this routinely.
- Short-chain fatty acid levels: Fecal butyrate, propionate, and acetate levels reflect microbial metabolic function.
- Intestinal permeability markers: Zonulin, LPS antibodies — markers of barrier integrity.
- Microbiome testing is part of our standard diagnostic workup.
What Targets It
- Dietary diversity: The single most important modulator of microbiome composition. Fiber diversity — not just fiber quantity — feeds diverse bacterial populations.
- Targeted probiotics: Species-specific supplementation based on testing results. Not generic probiotic capsules — targeted restoration of depleted species.
- Gut restoration protocols: Comprehensive approach combining prebiotics, probiotics, mucosal healing agents, and antimicrobial treatment of pathobionts where indicated.
- Fecal microbiota transplantation (FMT): The most direct approach to microbiome restoration. Evidence is strong for C. difficile and emerging for other conditions. Investigational for longevity, but the preclinical data (aged mice receiving young donor microbiome) is striking.
- Avoid unnecessary antibiotics: Broad-spectrum antibiotics cause lasting microbiome disruption. Every antibiotic course should be clinically justified.
How I Use This Framework
In my clinical practice, the hallmarks framework translates into three practical steps:
Step 1: Measure the Hallmarks
No patient gets a generic longevity protocol. Every patient gets a comprehensive assessment that maps their specific hallmark profile:
- Epigenetic age testing (Hallmark 3)
- Comprehensive blood panel including inflammatory markers, hormones, metabolic parameters (Hallmarks 6, 10, 11)
- Telomere length (Hallmark 2)
- Mitochondrial function testing (Hallmark 7)
- Microbiome sequencing (Hallmark 12)
- Immune function panel (Hallmarks 9, 10, 11)
- Oxidative stress markers (Hallmark 1)
Step 2: Identify the Dominant Drivers
Not all hallmarks are equally accelerated in every patient. A 55-year-old former athlete may have excellent mitochondrial function but significant epigenetic aging from chronic stress. A 40-year-old with Lyme history may have dominant inflammation and dysbiosis with relatively preserved metabolic health. The treatment targets the dominant drivers, not a generic checklist.
Step 3: Intervene with Specificity
Match the intervention to the hallmark:
| Dominant Hallmark | Primary Intervention |
|---|---|
| Genomic instability | NAD+, detoxification, antioxidant optimization |
| Telomere attrition | Epithalon, lifestyle optimization, infection treatment |
| Epigenetic alterations | Rapamycin, alpha-ketoglutarate, methyl donor optimization |
| Loss of proteostasis | Hyperthermia, cold/heat protocols |
| Disabled autophagy | Fasting protocols, rapamycin, spermidine |
| Deregulated nutrient sensing | Metformin, fasting, dietary optimization |
| Mitochondrial dysfunction | IHHT, CoQ10, exercise, NAD+, methylene blue |
| Cellular senescence | Senolytics (D+Q, fisetin) |
| Stem cell exhaustion | MSC therapy, hyperbaric oxygen, NAD+ |
| Altered intercellular communication | Hormone optimization, peptide therapy, apheresis |
| Chronic inflammation | Address upstream driver (infection, senescence, dysbiosis, metabolic) |
| Dysbiosis | Microbiome restoration, gut reset protocol, dietary diversity |
The Interconnection Problem
Here is the nuance that matters: these hallmarks do not operate independently. Mitochondrial dysfunction increases ROS, which causes genomic instability. Genomic instability triggers senescence. Senescent cells drive inflammation. Inflammation promotes dysbiosis. Dysbiosis worsens inflammation. Everything connects.
This is why single-intervention longevity strategies are fundamentally limited. Taking rapamycin alone addresses hallmarks 3, 5, and 6 but does nothing for hallmarks 1, 2, 7, or 12. Taking a senolytic alone addresses hallmark 8 but not the upstream drivers creating new senescent cells.
The physician’s role — and this is what I tell my patients — is to identify which hallmarks are most accelerated in your specific biology and build a protocol that addresses the interconnected web, not just a single thread. This is personalized longevity medicine, and it is what distinguishes clinical practice from internet advice.
The Bottom Line
The 12 hallmarks of aging are not abstract biology. They are a clinical framework that transforms longevity medicine from guesswork into targeted intervention. Every hallmark can be measured, at least partially. Every hallmark has interventions that target it, ranging from strong evidence to emerging. The art of longevity medicine lies in assessing which hallmarks are dominant in each individual and building a protocol that addresses the interconnected drivers — not throwing every supplement at the wall and hoping something works. My father founded this hospital with the conviction that medicine should use every tool available. The hallmarks framework tells us which tools to reach for first.
References
- Lopez-Otin C, et al. Hallmarks of aging: An expanding universe. Cell. 2023;186(2):243-278. doi:10.1016/j.cell.2022.11.001.
- Schumacher B, et al. The central role of DNA damage in the ageing process. Nature. 2021;592(7856):695-703. doi:10.1038/s41586-021-03307-7.
- Blackburn EH, et al. Human telomere biology: A contributory and interactive factor in aging, disease risks, and protection. Science. 2015;350(6265):1193-1198. doi:10.1126/science.aab3389.
- Pal S, Tyler JK. Epigenetics and aging. Science Advances. 2016;2(7):e1600584. doi:10.1126/sciadv.1600584.
- Fontana L, et al. Extending healthy life span — from yeast to humans. Science. 2010;328(5976):321-326. doi:10.1126/science.1172539.
- Sun N, et al. The mitochondrial basis of aging. Molecular Cell. 2016;61(5):654-666. doi:10.1016/j.molcel.2016.01.028.
- Childs BG, et al. Senescent cells: an emerging target for diseases of ageing. Nature Reviews Drug Discovery. 2017;16(10):718-735. doi:10.1038/nrd.2017.116.
- Franceschi C, et al. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nature Reviews Endocrinology. 2018;14(10):576-590. doi:10.1038/s41574-018-0059-4.
- Boehme M, et al. Microbiota from young mice counteracts selective age-associated behavioral deficits. Nature Aging. 2021;1:666-676. doi:10.1038/s43587-021-00093-9.
This content is educational and does not constitute medical advice. Longevity interventions, including rapamycin, senolytics, and hormone optimization, are medical treatments that require physician supervision, individualized assessment, and ongoing monitoring. Every conventional medicine was once alternative medicine — but every intervention deserves rigorous evaluation before clinical use.