You have headaches that come and go without a clear trigger. Your skin flushes after wine or fermented food. Your gut alternates between bloating and cramping. You have been told it is stress, IBS, or anxiety. You have been to an allergist, and the allergy tests came back negative.
Here is what I tell my patients: if your allergist says you do not have an allergy, they are probably right. But that does not mean histamine is not the problem. Histamine intolerance is not an allergy. It is a degradation deficit — and the distinction matters for treatment.
At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate (clinical data, smaller RCTs) |
| Primary Use | Chronic unexplained symptoms: headaches, flushing, GI distress, urticaria, anxiety |
| Key Mechanism | Impaired diamine oxidase (DAO) activity leading to systemic histamine excess |
What Histamine Actually Does
Histamine is not inherently harmful. It is a biogenic amine with critical physiological roles: gastric acid secretion, neurotransmission, immune regulation, circadian rhythm modulation, and vasodilation. Your body produces it, and you consume it through food. Under normal conditions, two enzyme systems keep histamine in balance.
Diamine oxidase (DAO) is the primary enzyme responsible for degrading extracellular histamine, particularly histamine absorbed from the gastrointestinal tract. It is produced predominantly in the intestinal mucosa, kidneys, and placenta [1].
Histamine N-methyltransferase (HNMT) handles intracellular histamine degradation, primarily in the liver and central nervous system.
When these systems — particularly DAO — cannot keep pace with histamine intake or production, histamine accumulates. The result is a condition that can mimic allergies, migraines, irritable bowel syndrome, anxiety disorders, and even cardiac arrhythmias.
Why This Gets Misdiagnosed
The diagnostic challenge with histamine intolerance is that it presents differently in almost every patient. The four histamine receptor subtypes (H1 through H4) are distributed across virtually every organ system. Depending on which receptors are most affected, symptoms may be predominantly:
- Dermatological: urticaria, flushing, pruritus, eczema flares
- Gastrointestinal: bloating, cramping, diarrhea, nausea, reflux
- Neurological: headaches, migraines, dizziness, brain fog, anxiety, insomnia
- Cardiovascular: tachycardia, hypotension, palpitations
- Respiratory: nasal congestion, rhinitis, asthma-like symptoms
- Gynecological: dysmenorrhea, premenstrual worsening of all symptoms
A patient presenting with migraines sees a neurologist. A patient with palpitations sees a cardiologist. A patient with bloating sees a gastroenterologist. Each specialist addresses their domain and often misses the unifying mechanism. In my clinical experience, patients with histamine intolerance have typically seen four to six specialists before the diagnosis is made.
The standard allergy workup — skin prick tests, specific IgE — is negative because histamine intolerance is not IgE-mediated. It is not an allergy. It is a metabolic insufficiency.
The Gut Connection
Let me be direct: in the majority of patients I see with histamine intolerance, the gut is the primary driver. This is not speculation — it follows directly from the biology.
DAO is produced predominantly by enterocytes in the intestinal villi. Anything that damages the intestinal mucosa — chronic inflammation, dysbiosis, small intestinal bacterial overgrowth (SIBO), celiac disease, inflammatory bowel disease, or even prolonged NSAID use — impairs DAO production [2].
This creates a vicious cycle:
- Gut inflammation reduces DAO production
- Reduced DAO allows dietary histamine to enter the systemic circulation
- Systemic histamine triggers further inflammation, including in the gut
- Gut inflammation worsens, further reducing DAO
This is why elimination diets alone are often insufficient. You can restrict high-histamine foods indefinitely and never resolve the underlying DAO deficit if the gut inflammation persists. The nuance matters: dietary restriction manages symptoms, but gut restoration addresses the cause.
The Microbiome Dimension
Certain gut bacteria are prolific histamine producers. Morganella morganii, Klebsiella pneumoniae, Enterobacter aerogenes, and specific strains of Lactobacillus and Enterococcus generate histamine as a metabolic byproduct through histidine decarboxylase activity [3].
Conversely, other bacterial strains — Bifidobacterium infantis, Lactobacillus rhamnosus — degrade histamine or promote DAO expression. The composition of the microbiome directly influences the net histamine burden in the gut lumen.
In patients with SIBO or dysbiosis, the histamine-producing bacterial population may be dramatically elevated. I have seen patients whose histamine intolerance symptoms resolved entirely after addressing SIBO, without any ongoing dietary restriction. This is what the research actually says: the microbiome is not a peripheral factor — it is central [4].
Diagnosis: What Works and What Does Not
Serum DAO Levels
Measuring serum DAO is the most commonly used test, and it has limitations. A low DAO level (below 10 U/mL) supports the diagnosis, but a normal level does not exclude it. DAO activity varies with meals, menstrual cycle, medications, and time of day. A single fasting measurement captures only a snapshot.
That said, in clinical practice, serum DAO below 10 U/mL combined with compatible symptoms has reasonable diagnostic value. I use it as one data point, not as a definitive test.
Histamine in Plasma and Urine
Plasma histamine is highly unstable and technically difficult to measure accurately. Methylhistamine in 24-hour urine is more reliable but still affected by dietary intake in the collection period. I find these tests most useful when consistently elevated across multiple measurements.
The Elimination-Reintroduction Protocol
In my clinical experience, the most reliable diagnostic tool remains a structured low-histamine elimination diet for two to four weeks, followed by systematic reintroduction. If symptoms improve substantially on elimination and return reproducibly with reintroduction, the diagnosis is essentially confirmed regardless of laboratory values.
This is pragmatic medicine. The test that matters most is the one that changes outcomes.
What to Rule Out
Before diagnosing histamine intolerance, I always exclude:
- Mast cell activation syndrome (MCAS): Elevated tryptase, 24-hour urine prostaglandins and histamine metabolites. MCAS involves inappropriate mast cell degranulation — a distinct mechanism from DAO insufficiency.
- Systemic mastocytosis: Rare but serious. Bone marrow biopsy if tryptase is persistently elevated.
- True IgE-mediated food allergies: Standard allergy workup.
- Celiac disease: Tissue transglutaminase antibodies. Celiac damages intestinal villi and directly impairs DAO production.
The Evidence for Treatment
Dietary Management
The low-histamine diet is the foundation, but I want to frame this correctly. The evidence supporting low-histamine diets for symptom control is moderate — multiple observational studies and smaller controlled trials show significant symptom improvement [5]. However, histamine content in foods varies enormously depending on freshness, storage conditions, bacterial contamination, and preparation methods. Published “histamine food lists” are approximations, not absolute values.
What I tell my patients: focus on freshness. Histamine accumulates in food over time through bacterial decarboxylation of histidine. A fresh piece of fish has minimal histamine. The same fish three days later may have very high levels. Fermented foods — aged cheese, sauerkraut, kombucha, wine — are consistently high. Beyond that, individual tolerance varies, and systematic self-experimentation is more useful than rigid lists.
DAO Supplementation
Exogenous DAO enzyme supplements (typically porcine-derived) taken before meals can improve histamine degradation in the gut lumen. A randomized, double-blind, placebo-controlled trial published in 2019 demonstrated that DAO supplementation significantly reduced symptom scores in patients with histamine intolerance compared to placebo [6].
This is one of the more solid pieces of evidence in this field. DAO supplementation is not curative — it is a bridge strategy that reduces symptom burden while underlying causes are addressed.
Nutrient Cofactors
DAO requires specific cofactors for enzymatic activity:
- Vitamin B6 (pyridoxal-5-phosphate): Essential cofactor for DAO. Deficiency impairs enzyme function. I routinely assess B6 status in patients with histamine intolerance.
- Vitamin C: Functions as a histamine-degrading agent and supports DAO activity. Doses of 1,000-2,000 mg daily have shown modest benefit in clinical observations.
- Copper: Required for DAO catalytic activity. However, supplementation should be guided by testing — copper excess carries its own risks.
- Zinc: Supports overall immune regulation and has indirect effects on histamine metabolism.
Gut Restoration
This is where I see the most meaningful long-term improvement. Addressing the underlying gut pathology — treating SIBO, rebalancing the microbiome, healing intestinal permeability, managing inflammation — restores endogenous DAO production.
In our clinical experience treating patients with histamine intolerance and concurrent gut pathology, a structured gut restoration protocol over three to six months frequently allows patients to liberalize their diet substantially. Some patients achieve complete resolution of histamine intolerance symptoms once the gut is healed. Not all — but enough that gut restoration should be the primary therapeutic target, not just a supplementary strategy.
Medications
For acute symptom management:
- H1 antihistamines (cetirizine, loratadine): symptom control, not disease modification
- H2 antihistamines (famotidine): useful for GI-predominant symptoms
- Cromoglicic acid (cromolyn sodium): mast cell stabilizer, helpful in a subset of patients
These are tools for symptom management, not solutions. I use them as bridges while addressing root causes.
What I See in Practice
Based on treating hundreds of patients with histamine intolerance at our hospital, several patterns are consistent:
The overlap with Lyme and post-COVID is substantial. Chronic infections and post-infectious states frequently damage the gut mucosa and shift the microbiome toward histamine-producing species. Many of our Lyme disease patients and post-COVID patients have secondary histamine intolerance that resolves as the primary condition improves.
Hormonal fluctuations matter. Estrogen inhibits DAO activity. This is why many women experience worsening histamine symptoms premenstrually, during perimenopause, or on estrogen-containing contraceptives. Addressing hormonal optimization can meaningfully impact histamine tolerance.
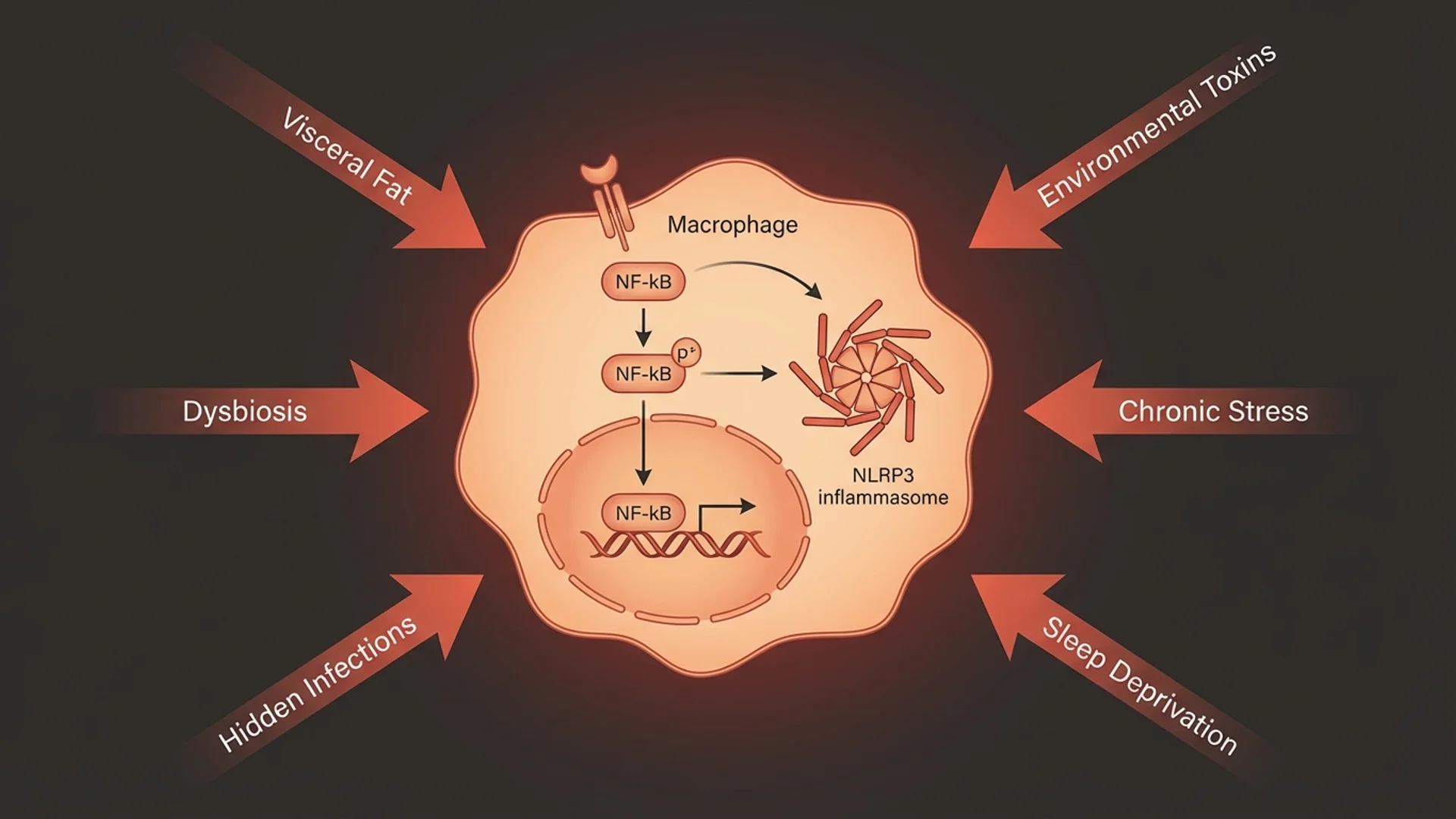
Stress is a real amplifier. Cortisol and catecholamines directly stimulate mast cell degranulation. Patients in chronic stress states have higher baseline histamine release, compounding any DAO insufficiency. This is not dismissing symptoms as “stress” — it is recognizing a measurable physiological interaction.
The patients who improve most are those who address all three layers simultaneously: reduce histamine load (diet), support degradation capacity (DAO enzyme, cofactors), and restore gut function (microbiome, mucosal healing).
Practical Protocol
For patients presenting with suspected histamine intolerance, my approach follows this sequence:
- Baseline assessment: Serum DAO, plasma histamine, tryptase (to exclude MCAS), comprehensive gut analysis including microbiome sequencing, celiac panel, inflammatory markers
- Two-to-four-week low-histamine elimination: Strict but time-limited. The goal is diagnostic clarity, not permanent restriction.
- Concurrent gut investigation: Breath testing for SIBO, stool analysis for dysbiosis, assessment for intestinal permeability
- Symptomatic support: DAO enzyme supplementation before meals, vitamin B6 (P5P 50-100 mg daily), vitamin C (1,000-2,000 mg daily), H1/H2 antihistamines as needed
- Gut restoration: Targeted antimicrobial or probiotic therapy based on test results, mucosal healing support (L-glutamine, zinc carnosine, butyrate)
- Systematic reintroduction: After four to eight weeks of gut restoration, gradual reintroduction of moderate-histamine foods to establish individual tolerance thresholds
- Long-term monitoring: Repeat DAO levels, symptom tracking, microbiome reassessment at three and six months
Safety and Considerations
Histamine intolerance treatment is generally low-risk, but several points deserve attention:
- DAO supplements are typically well tolerated. Patients with pork allergy should verify the source (most are porcine-derived).
- Overly restrictive diets maintained long-term can lead to nutritional deficiencies and disordered eating patterns. The goal is always to expand the diet over time, not to restrict it indefinitely.
- Copper supplementation should be guided by laboratory testing. Empiric copper supplementation without monitoring is inadvisable.
- Do not stop prescribed medications (including NSAIDs, certain antidepressants, or antihypertensives that may impair DAO) without discussing with your prescribing physician. Some of these medications are medically necessary, and the risk-benefit calculation must be individualized.
The Bottom Line
Histamine intolerance is a real, measurable, treatable condition — not a fad diagnosis and not “just allergies.” The mechanism is well understood: insufficient DAO activity relative to histamine load, most commonly driven by gut pathology. Treatment that addresses only diet without restoring gut function is treating the shadow, not the source. In my experience, patients who pursue comprehensive gut restoration alongside targeted histamine management achieve the most durable results.
References
- Maintz L, Novak N. Histamine and histamine intolerance. American Journal of Clinical Nutrition. 2007;85(5):1185-1196. PMID: 17490952.
- Comas-Baste O, et al. Histamine intolerance: The current state of the art. Biomolecules. 2020;10(8):1181. doi:10.3390/biom10081181.
- Landete JM, et al. Updated knowledge about histamine biosynthesis by bacteria. Critical Reviews in Food Science and Nutrition. 2008;48(8):697-714. PMID: 18756396.
- Schink M, et al. Microbial patterns in patients with histamine intolerance. Journal of Physiology and Pharmacology. 2018;69(4):579-593. PMID: 30552302.
- Son JH, et al. A histamine-free diet is helpful for treatment of adult patients with chronic spontaneous urticaria. Annals of Dermatology. 2018;30(2):164-172. doi:10.5021/ad.2018.30.2.164.
- Izquierdo-Casas J, et al. Diamine oxidase (DAO) supplement reduces headache in episodic migraine patients with DAO deficiency: A randomized double-blind trial. Clinical Nutrition. 2019;38(1):152-158. doi:10.1016/j.clnu.2018.01.013.
This content is educational and does not constitute medical advice. Histamine intolerance should be diagnosed and managed under the supervision of a qualified physician. Do not discontinue prescribed medications without consulting your doctor.