Topic
Infectiology
Chronic Lyme, Post-COVID, co-infections, biofilms, and the integrative approach to persistent infections. 30 years of clinical experience at St. George Hospital.
Explore by Topic
Lyme Disease (Borrelia)
Chronic Borrelia infection — diagnosis, treatment, and the persistent disease controversy.
Bartonella
The stealth co-infection that is often the primary driver of neuropsychiatric symptoms.
Babesia
Intraerythrocytic parasite causing hemolytic symptoms and fatigue in co-infected patients.
Biofilms
How bacterial biofilms protect persistent infections and strategies to disrupt them.
Co-Infections
Multiple simultaneous tick-borne infections and their synergistic effects.
Post-COVID / Long COVID
Microclots, spike protein persistence, brain fog, and treatment approaches.
Mold & CIRS
Chronic inflammatory response syndrome from biotoxin and mold exposure.
Reactivated Viruses
EBV, CMV, HHV-6 reactivation in immunocompromised and post-infectious patients.
Herxheimer Reactions
Managing die-off reactions during antimicrobial and detoxification treatment.
Therapeutic Apheresis
Blood filtration for toxin removal, microclot clearance, and immune modulation.
Free Guide
The Complete Lyme Disease Treatment Guide
Download the complete physician's guide. Evidence-based, no hype.
Articles
60 articles
CD57 Test in Lyme Disease: Useful or Unreliable?
The CD57 test in Lyme disease — what it measures, Dr. Stricker's original hypothesis, conflicting study results, and how clinicians actually use it in practice.

iSpot Lyme T-Cell Test: A Better Way to Detect Borrelia?
How the iSpot Lyme (ELISpot) T-cell test works, its advantages over antibody testing, 84% sensitivity data, limitations, and when it adds clinical value.
Lyme Disease False Negatives: Why Standard Tests Miss Chronic Lyme
Why Lyme disease tests come back negative in patients with active infection. ELISA sensitivity gaps, antibody window, seronegative Lyme, and what to do when tests miss.

Lyme Disease, Gut Dysbiosis, and Leaky Gut
How Lyme disease disrupts the gut microbiome. Antibiotic-driven dysbiosis, Borrelia's effect on intestinal permeability, the Hopkins microbiome findings, and recovery strategies.

Western Blot vs ELISA: Lyme Testing Accuracy Compared
Head-to-head comparison of Western Blot and ELISA for Lyme disease. Sensitivity at each stage, what the bands mean, the two-tier protocol, and why the system misses patients.
Whole-Body Hyperthermia for Lyme: Why 2 Sessions, Not 6
Why St. George Hospital uses 2 extreme hyperthermia sessions at 41.6-41.8°C for Lyme eradication, not 5-6 moderate sessions. The science behind the protocol.
Hyperthermia Side Effects and What to Expect During Treatment
Honest guide to whole-body hyperthermia side effects. What happens during treatment, common reactions, Herxheimer responses, recovery timeline, and contraindications.
What Is Whole-Body Hyperthermia? A Complete Guide
Whole body hyperthermia treatment explained by a physician. How controlled fever therapy works for Lyme, cancer, and post-COVID at St. George Hospital.
Babesia and Air Hunger: Why You Can't Catch Your Breath
Why Babesia causes air hunger — the autonomic and hemolytic mechanisms behind this hallmark symptom, and what it means for diagnosis and treatment.
Babesia Treatment Failure: What to Do When Standard Therapy Doesn't Work
Options beyond atovaquone-azithromycin for relapsing babesiosis. Combination protocols, herbal adjuncts, and when exchange transfusion is considered.
Babesia vs Malaria: Intraerythrocytic Parasites Compared
How Babesia and malaria parasites differ in transmission, symptoms, diagnostics, and treatment — and why Babesia is often called the malaria of the North.
Bartonella Herbal Treatment Protocols
Evidence-based herbal protocols for Bartonella including Cryptolepis, Japanese Knotweed, and Cat's Claw — what the research shows and how clinicians use them.
Bartonella and Neuropsychiatric Symptoms
How Bartonella infection causes anxiety, rage, OCD, and psychiatric symptoms — the NC State research, diagnostic challenges, and treatment approaches.
Bartonella Stretch Marks (Striae): What They Mean
How to identify Bartonella-Associated Cutaneous Lesions (BACL) — the distinctive skin markings that mimic stretch marks and signal active Bartonella infection.
Why Antibiotics Alone Fail Against Biofilms
How bacterial biofilms reduce antibiotic efficacy by 100-1,000x, why standard treatment courses miss persistent infections, and what integrative approaches add.
Biofilm Disruption Protocols for Chronic Infections
A clinical overview of biofilm disruption strategies for persistent Lyme disease — the three-phase approach of disrupt, kill, and clear.
Nattokinase and Serrapeptase for Biofilm Disruption
How proteolytic enzymes nattokinase and serrapeptase degrade biofilm matrix components — mechanism, dosing, evidence, and clinical considerations.
CIRS Symptom Checklist: HLA-DR Genetics and Biotoxin Illness
The 37 symptoms of CIRS across 13 clusters, HLA-DR genetic susceptibility, and why 25% of the population cannot clear biotoxins normally.
CIRS vs MCAS: Overlapping Conditions Differentiated
How to distinguish CIRS from MCAS, why they frequently co-occur, and why treating only one often fails. HLA-DR genetics, mast cell activation, and the upstream driver.
EBV Reactivation: When Epstein-Barr Comes Back
Why Epstein-Barr virus reactivates in chronic illness, how it drives fatigue and immune dysfunction, and what treatment options exist for reactivated EBV.
Lyme Treatment: Germany vs the United States
A direct comparison of American IDSA Lyme guidelines and German integrative Lyme treatment. Why patients travel to Germany, what's different, and what the evidence supports.
H.E.L.P. Apheresis: How Blood Filtration Removes What Shouldn't Be There
How H.E.L.P. apheresis filters LDL, fibrinogen, CRP, and microclots from your blood. Mechanism, session details, evidence, and clinical experience at Klinik St. Georg.
Is Herxing a Good Sign? What Die-Off Actually Means
Does a Herxheimer reaction mean treatment is working? The science behind die-off, why worse does not always mean better, and the goal of controlled pathogen clearance.
Managing Herxheimer Reactions at Home
Evidence-based strategies for managing Jarisch-Herxheimer reactions during Lyme treatment — hydration, detox support, dose pacing, and when to call your doctor.

Herxheimer Reaction vs Disease Flare: How to Tell the Difference
A clinical framework for distinguishing Jarisch-Herxheimer reactions from disease flares in Lyme treatment — timing, symptom patterns, and when to act.
HHV-6 and Lyme Disease: The Co-Reactivation Problem
Why HHV-6 reactivates in virtually all chronic Lyme patients, its contribution to neurological symptoms, and testing and treatment approaches.
Mold Testing: Urine Mycotoxins vs ERMI vs Air Testing
Comparing mold testing methods — urine mycotoxin testing for body burden, ERMI for environmental exposure, and air sampling limitations. Which test you actually need.
Neuroborreliosis: When Lyme Crosses the Blood-Brain Barrier
How Borrelia invades the central nervous system, why neuroborreliosis is underdiagnosed, and how hyperthermia, TPS, and multimodal protocols treat what antibiotics alone cannot reach.
How Reactivated Viruses Suppress Your Immune System
The immune suppression cascade: how Lyme disease triggers EBV, HHV-6, and CMV reactivation, and how these viruses further suppress immunity in a vicious cycle.
Lyme Disease Symptoms: The Complete Checklist Doctors Miss
Comprehensive Lyme disease symptom checklist covering neurological, musculoskeletal, cardiac, psychiatric, and GI manifestations. Based on treating 12,000+ Lyme patients at Klinik St. Georg.
Medical Treatment in Germany: A Complete Guide for International Patients
Everything international patients need to know about medical treatment in Germany. Visa, costs, insurance, travel logistics, and what to expect at Klinik St. Georg in Bad Aibling — based on treating patients from 90+ countries.

Brain Fog Treatment: A Physician's Complete Guide
Brain fog treatment options from neuroinflammation workup to neuromodulation. Causes include post-COVID, Lyme, MCAS, and mold. TPS, NAD+, and hyperbaric oxygen covered.

Clearing Brain Fog After Treatment: Recovery Timeline
What to expect during brain fog recovery after Lyme treatment — the multi-system recovery approach, realistic timelines, and evidence-based strategies.
Brain Fog and Neuroinflammation: The PET Scan Evidence
What causes brain fog in Lyme disease — Johns Hopkins PET scan findings showing glial activation, neuroinflammation mechanisms, and treatment implications.

Neurofeedback for Lyme Brain Fog
How neurofeedback retrains dysregulated brainwave patterns in Lyme disease patients. qEEG findings, clinical evidence, and what to expect from treatment.

PEMF for Lyme Disease and Chronic Pain
How pulsed electromagnetic field therapy supports pain relief and inflammation reduction in Lyme disease — mechanism, clinical evidence, and practical considerations.
LL-37 for Biofilm Disruption in Chronic Lyme
How LL-37 disrupts Borrelia biofilms in chronic Lyme disease. Mechanism, preclinical evidence, protocol context, and clinical observations.
Apheresis for Long COVID: Removing Microclots and Restoring Circulation
How H.E.L.P. apheresis removes microclots and inflammatory mediators in Long COVID patients. Session protocols, evidence from Pretorius research, and clinical experience at Klinik St. Georg.
Long COVID: Symptoms, Mechanisms, and What Actually Helps
A clinical guide to Long COVID symptoms and treatment based on 500+ patients. Microclots, spike protein persistence, endothelial dysfunction, and the therapies that produce measurable results.
Nattokinase: The Fibrinolytic Enzyme for Microclots
Evidence-based guide to nattokinase for fibrinolysis and microclots. Mechanism, dosing, post-COVID relevance, combination with serrapeptase, and safety with blood thinners.

Lyme Testing: Why Standard ELISA Fails
Why standard Lyme disease tests miss infections, and which advanced tests provide accurate results. ELISpot, CD57, and beyond.
Antibiotic Resistance and Alternatives
How antibiotic resistance affects chronic infection treatment and what alternatives exist. A physician's perspective on navigating a post-antibiotic landscape.

Apheresis for Chronic Infections
How therapeutic apheresis filters inflammatory mediators, autoantibodies, and microclots. Applications in post-COVID and chronic infection treatment.
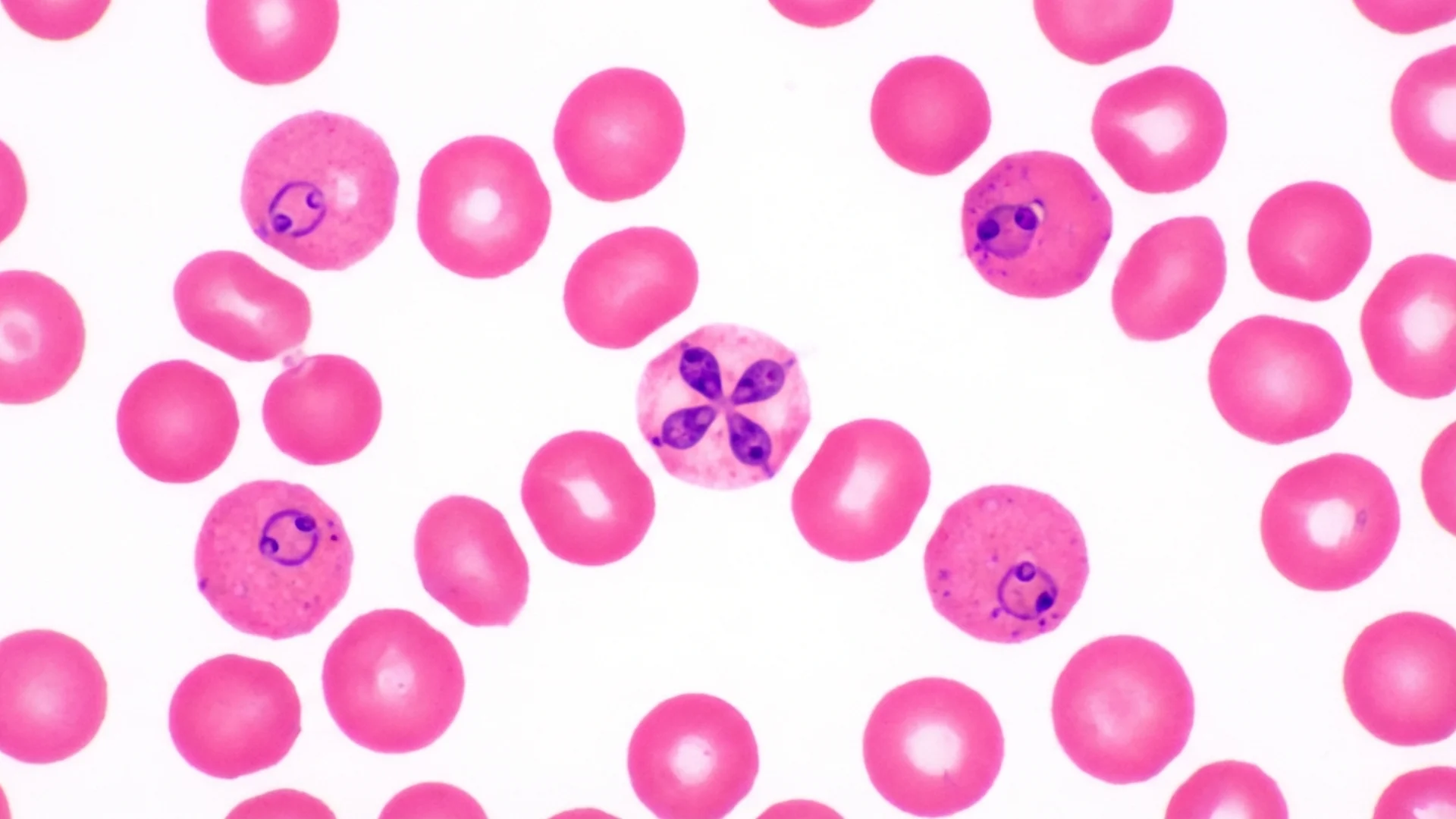
Babesia: The Parasitic Co-Infection
How Babesia differs from bacterial co-infections, why it requires antiparasitic treatment, and clinical signs that suggest Babesia involvement.
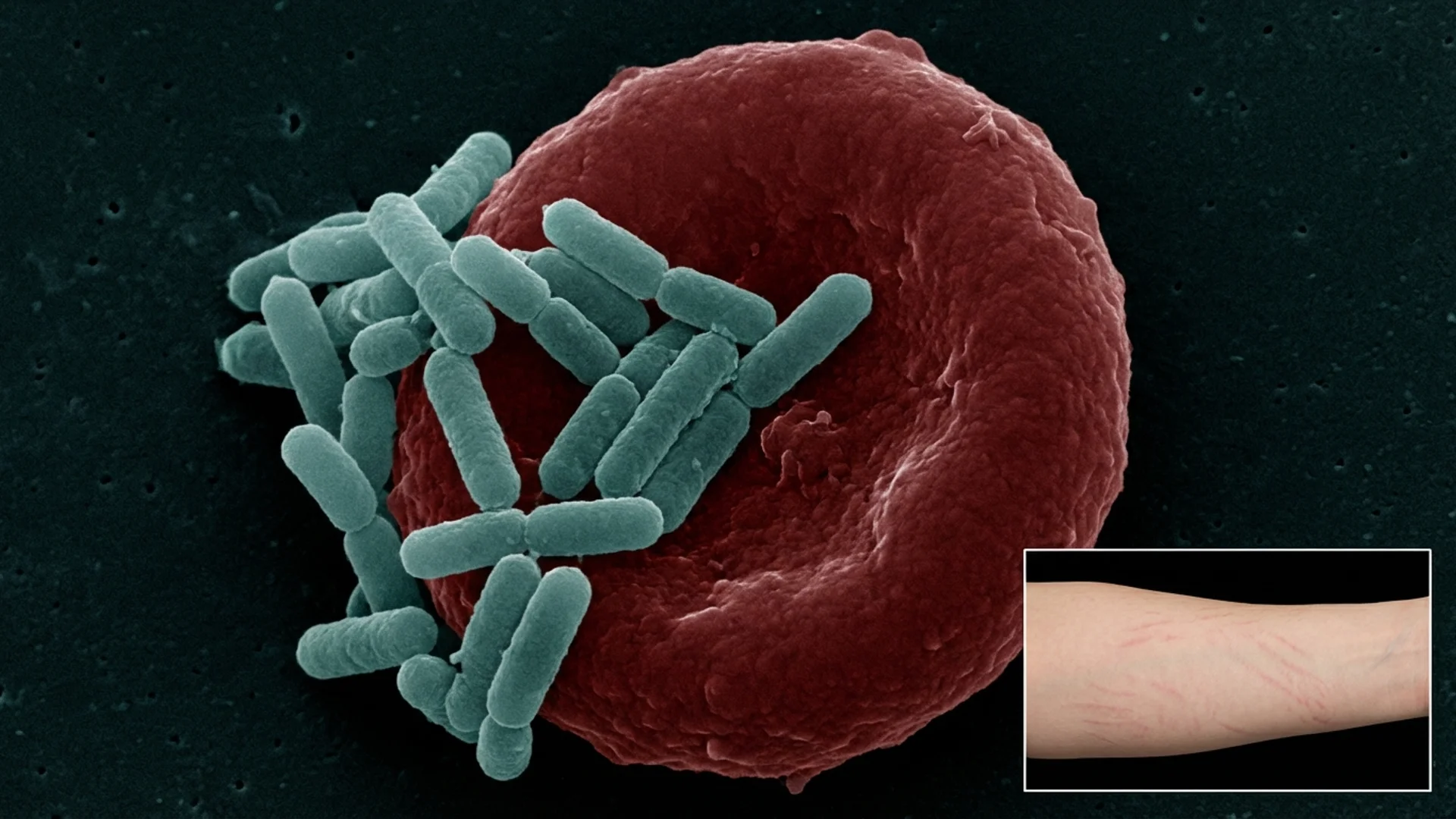
Bartonella: The Stealth Pathogen
Bartonella infection -- symptoms, diagnostic challenges, treatment approaches, and why this co-infection is often the primary driver of illness.
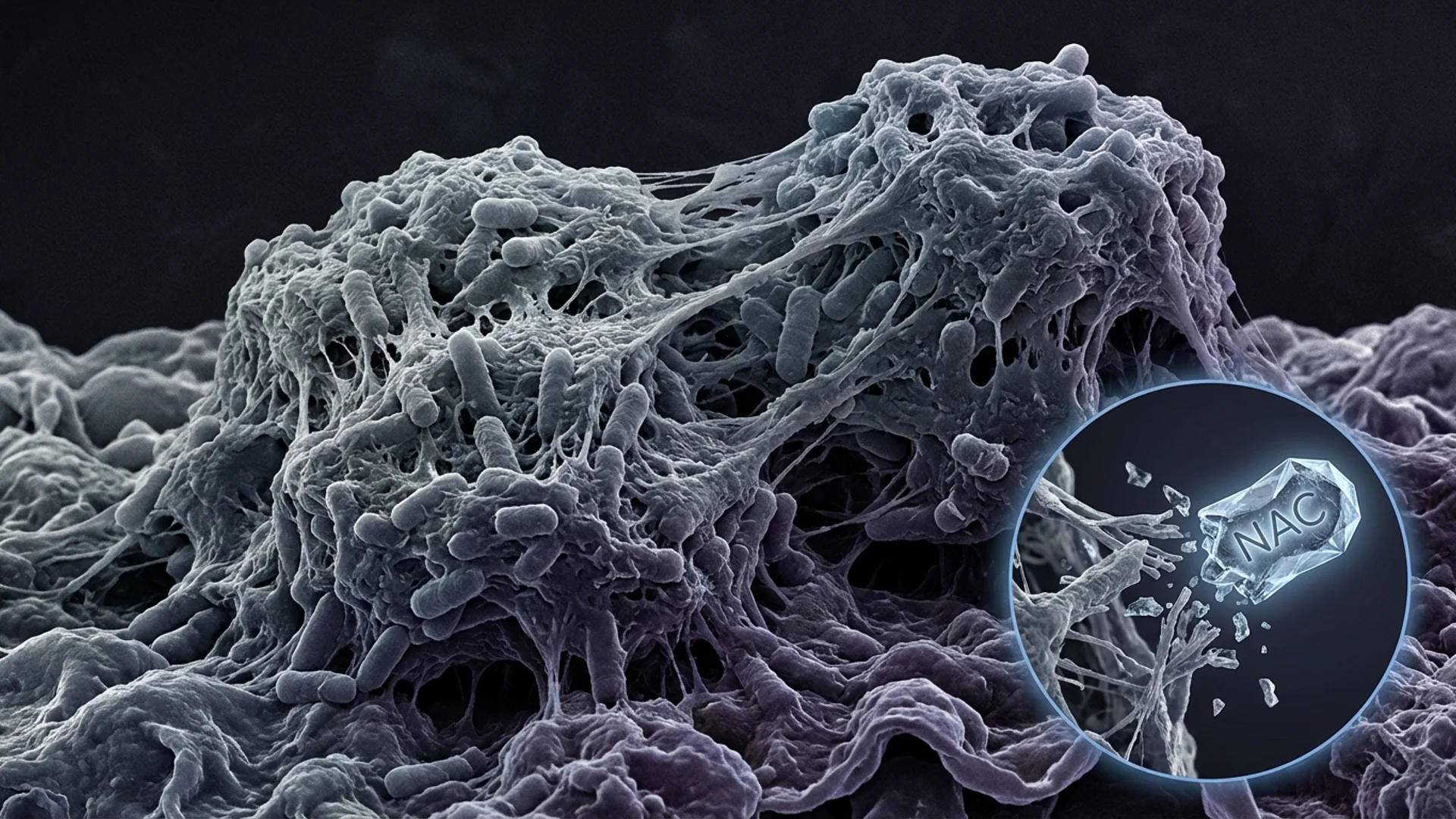
Biofilms: Why Infections Persist
How biofilms protect chronic infections from antibiotics and the immune system. Disruption strategies and clinical implications.
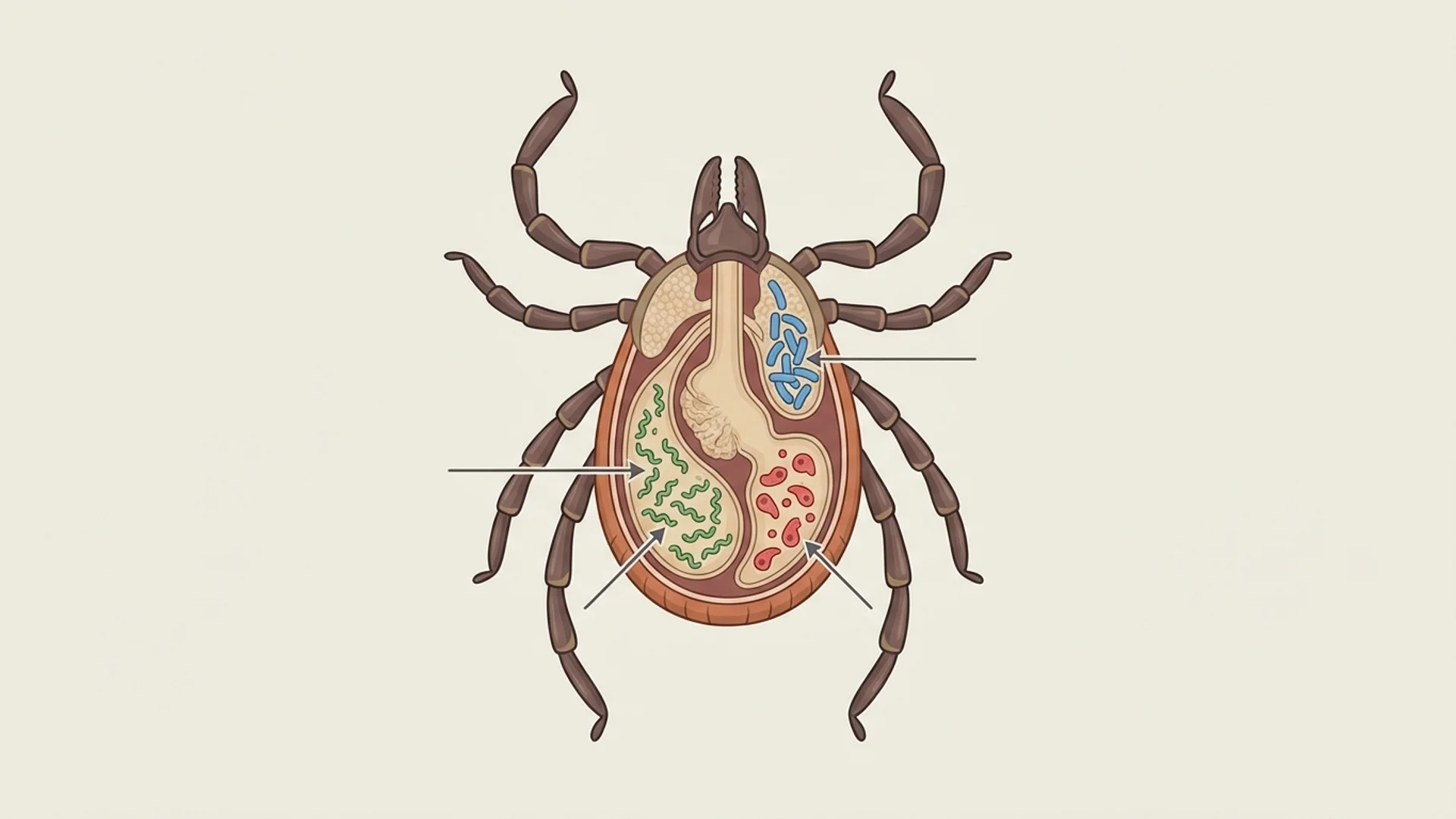
Co-Infections: The Hidden Complexity
Overview of tick-borne co-infections -- Bartonella, Babesia, Ehrlichia, Mycoplasma -- and why treating Lyme alone is often insufficient.
Ehrlichia and Anaplasma
Ehrlichiosis and anaplasmosis -- obligate intracellular co-infections that target white blood cells. Diagnosis, treatment, and clinical significance.
Herxheimer Reactions: What They Are
Understanding Jarisch-Herxheimer reactions during infection treatment. Why symptoms worsen before improving and how to manage the process.
Chronic Lyme Disease: What Medicine Misses
What conventional medicine gets wrong about chronic Lyme disease, why standard treatment fails some patients, and our integrative approach.

Why Patients Fly to Germany for Lyme Treatment
Why international patients seek Lyme disease treatment in Germany. Medical culture, treatment options, and what makes the German approach different.

Mold Illness and CIRS
Chronic Inflammatory Response Syndrome from mold exposure. How it overlaps with chronic infections, diagnosis, and treatment approaches.
Mycoplasma and Chlamydia Pneumoniae
How Mycoplasma and Chlamydia pneumoniae establish chronic intracellular infection. Symptoms, diagnosis, and treatment approaches.

Post-COVID Syndrome: Our Treatment Approach
How we treat Long COVID and post-COVID syndrome. Mechanisms, diagnostics, and a multimodal treatment program grounded in clinical experience.
Post-COVID Brain Fog: Mechanisms and Treatment
Why COVID-19 causes persistent cognitive dysfunction and what can be done about it. Mechanisms, assessment, and treatment strategies.
Microclots and Endothelial Dysfunction
How microclots and damaged blood vessel linings drive post-COVID symptoms. Dr. Beate Jaeger's research and clinical implications.
EBV, CMV, and HHV-6 Reactivation
How Epstein-Barr virus, cytomegalovirus, and HHV-6 reactivate during immune compromise. Diagnosis, clinical significance, and treatment.
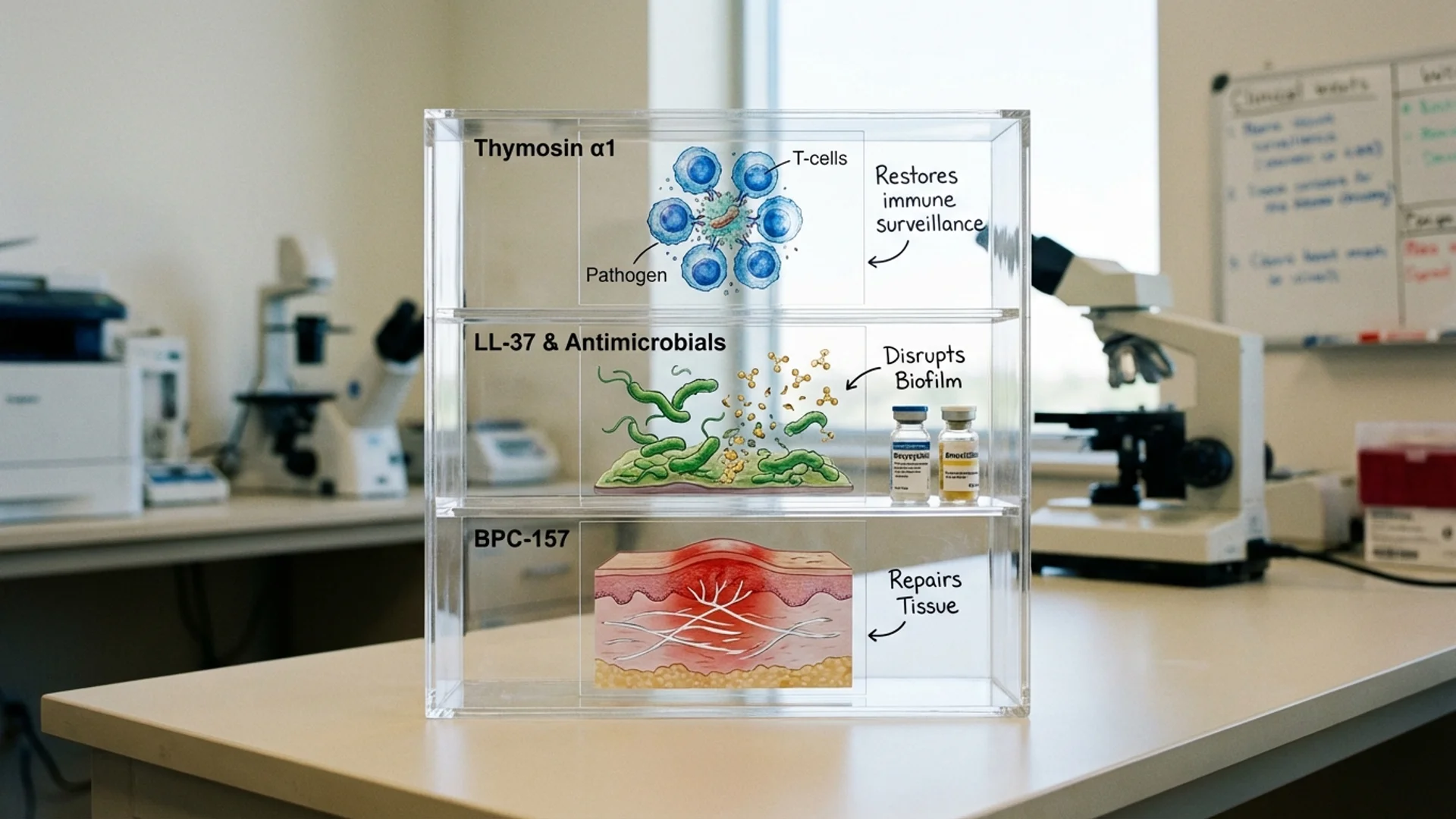
Peptide Therapy for Lyme Disease
How Dr. Julian Douwes uses peptides in chronic Lyme disease treatment. Thymosin alpha-1, LL-37, BPC-157 protocols alongside standard Lyme therapy.

Lyme Support Protocol: Between Treatments
A supplement and lifestyle protocol for Lyme disease patients between clinical treatments. Evidence levels included. By Dr. Julian Douwes.

Post-COVID Recovery Protocol
An evidence-based recovery protocol addressing inflammation, clotting, energy, and immune regulation after COVID-19. By Dr. Julian Douwes.
Complete Guide
Chronic Infections: A Modern Epidemic
In-depth reference by Dr. Julian Douwes
Chronic Infections: A Modern Epidemic
There is a category of patient that every experienced physician recognizes. They have seen multiple specialists. Their standard blood work is largely “normal.” They have been told their symptoms are stress-related, psychosomatic, or simply part of aging. They have fatigue that sleep does not resolve, cognitive difficulties that neurologists cannot explain, joint pain that rheumatologists find no inflammatory markers for, and a general sense that something is fundamentally wrong.
Many of these patients carry chronic infections.
This is not a fringe claim. It is an acknowledgment that our diagnostic framework — built primarily around acute infections with clear onset, identifiable pathogens, and definitive treatment — is poorly suited to the detection and management of persistent, low-grade, multisystemic infectious disease.
Why Chronic Infections Are Underdiagnosed
The problem begins with how we think about infection. Medical education teaches infection as a binary: you have an infection, or you do not. You treat it with an appropriate antibiotic, antiviral, or antifungal, and the infection resolves. This framework works well for acute pneumonia, urinary tract infections, and strep throat.
It works poorly for organisms that have evolved sophisticated survival strategies:
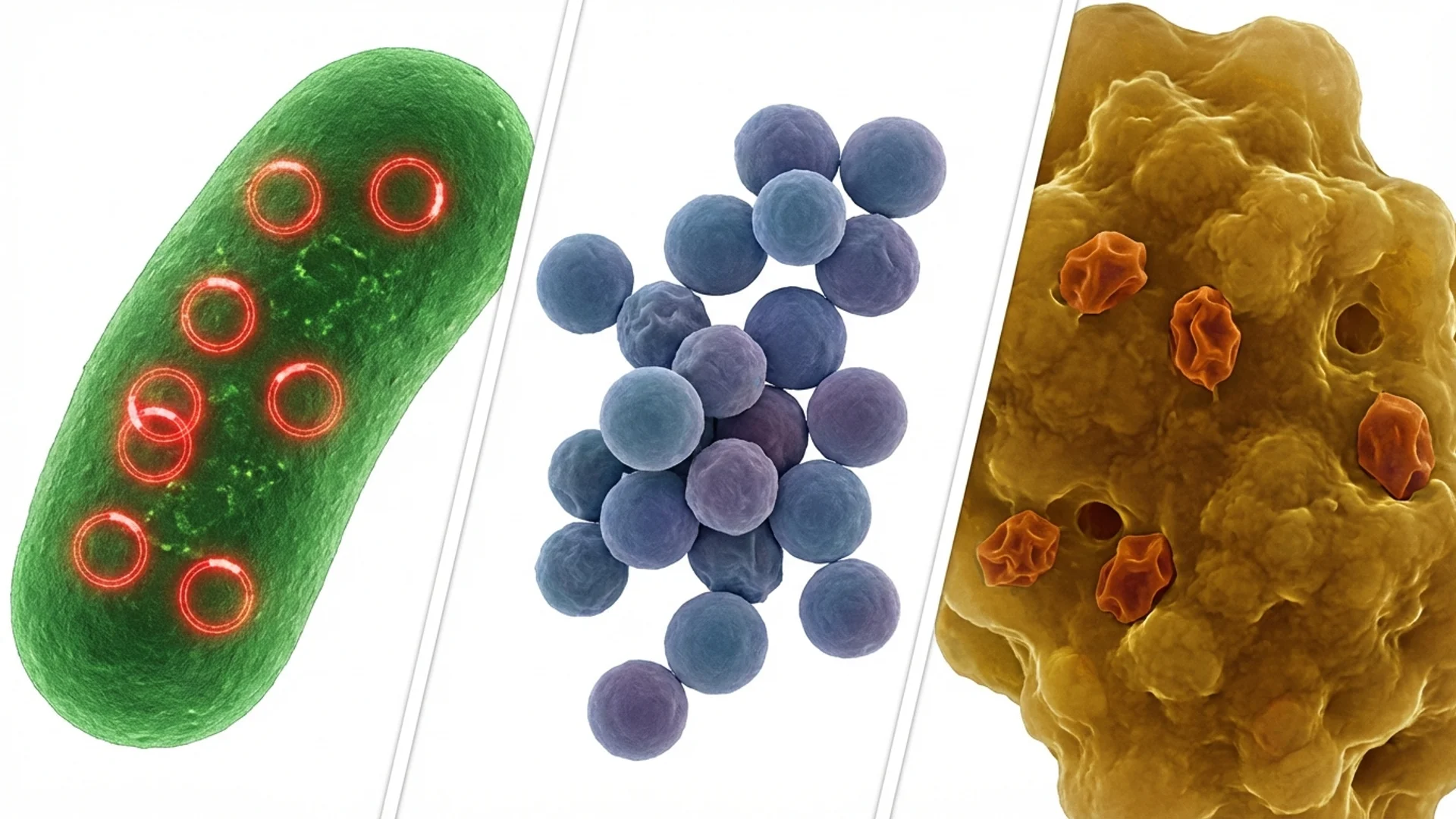
Intracellular persistence. Many pathogens — Borrelia, Bartonella, Mycoplasma, Chlamydia pneumoniae, Brucella — can survive inside human cells, shielded from both the immune system and many antibiotics. Standard serology may miss active infection because the immune response is compartmentalized [1].
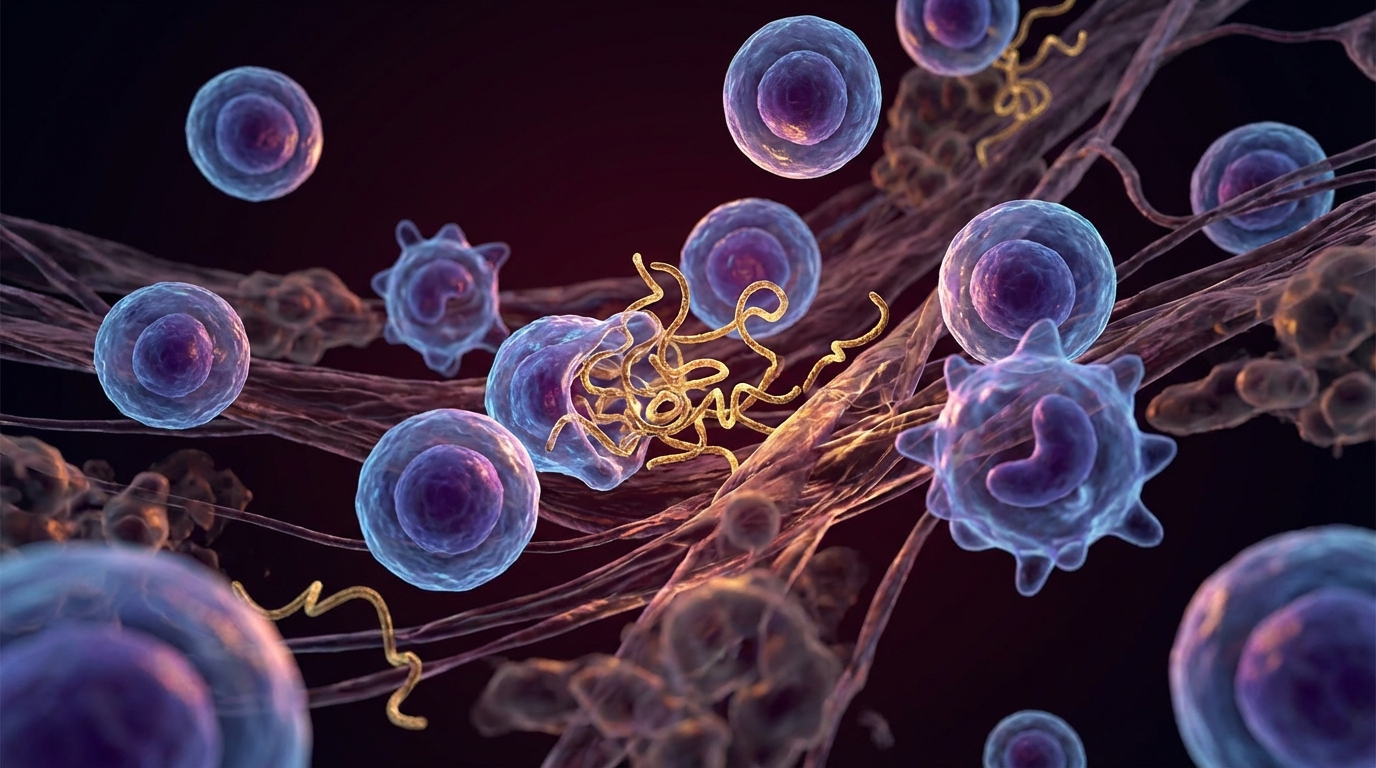
Biofilm formation. Certain organisms form protective biofilm communities — structured aggregates encased in an extracellular matrix that conventional antibiotics penetrate poorly. I discuss biofilms in detail in a dedicated article, because understanding them is essential to understanding why infections persist.
Immune evasion. Chronic pathogens have evolved to modulate host immune responses. Borrelia burgdorferi changes its surface proteins. EBV establishes lifelong latency in B cells. These are not passive organisms hiding in corners — they actively manipulate the immune system to ensure their survival.
Diagnostic limitations. The standard tests for many chronic infections are insensitive. Two-tier Lyme testing misses an estimated 30-60% of cases, depending on the stage and population studied [2]. Bartonella testing has even lower sensitivity. EBV and CMV serology can show “past infection” even when reactivation is occurring. The result is that many chronically infected patients test “negative” by standard criteria.
The Scope of the Problem
Chronic infections are not rare. Consider the epidemiology:
-
Lyme disease: The CDC acknowledges approximately 476,000 new cases annually in the United States alone. In Central Europe, where I practice, tick-borne diseases are endemic. An estimated 10-20% of treated Lyme patients develop persistent symptoms — a population numbering in the millions globally.
-
Epstein-Barr virus (EBV): Approximately 95% of the global adult population is seropositive. In most people, EBV remains latent. In some, it reactivates, contributing to chronic fatigue, autoimmune disease, and potentially certain cancers [3].
-
Post-COVID: An estimated 10-30% of COVID-19 survivors develop persistent symptoms. This represents tens of millions of people worldwide dealing with a post-infectious syndrome.
-
Mycoplasma and Chlamydia pneumoniae: Common respiratory pathogens that can establish chronic, intracellular infection associated with fatigue, neurological symptoms, and respiratory complaints.
-
Mold illness: While not a traditional “infection,” chronic mold exposure and Chronic Inflammatory Response Syndrome (CIRS) produce a clinical picture that overlaps significantly with chronic infection.
How Chronic Infections Cause Systemic Disease
The mistake that conventional medicine often makes is looking for the infection in the organ that hurts. A patient with joint pain gets a joint workup. A patient with cognitive complaints gets a neurological workup. A patient with fatigue gets a thyroid test.
Chronic infections do not respect organ boundaries. They cause systemic disease through several mechanisms:
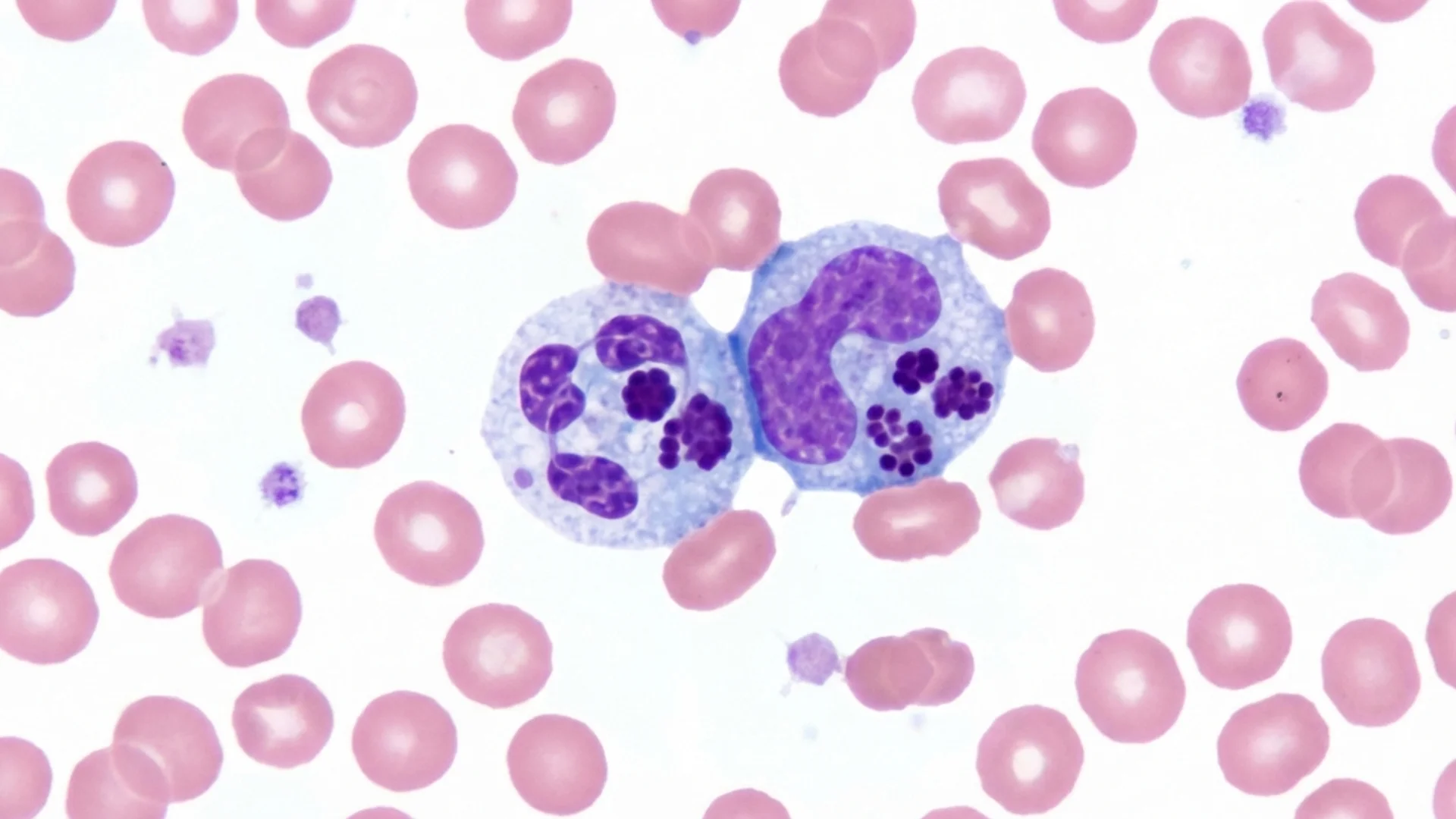
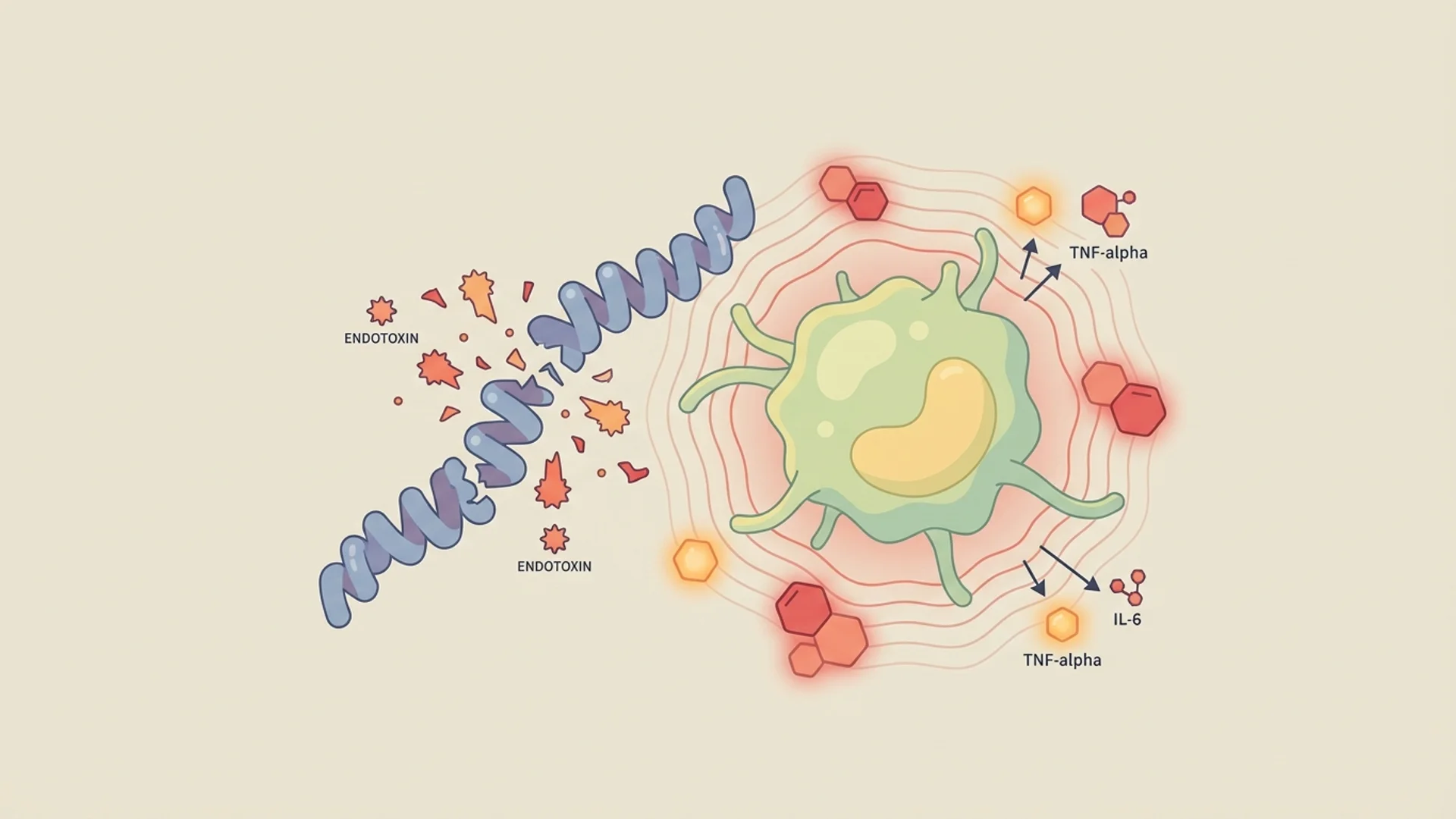
Chronic immune activation. The persistent presence of microbial antigens keeps the immune system in a state of chronic activation, producing inflammatory cytokines (IL-1, IL-6, TNF-alpha) that affect every organ system. This is the mechanism behind much of the fatigue, cognitive dysfunction, and pain that chronic infection patients experience.
Molecular mimicry and autoimmunity. Some microbial antigens resemble human proteins. The immune response directed against the pathogen cross-reacts with the patient’s own tissues, producing autoimmune-like symptoms. This has been documented in Lyme disease (cross-reactivity with neural tissue) and streptococcal infection (rheumatic heart disease).
Mitochondrial disruption. Multiple chronic pathogens directly impair mitochondrial function, either through toxin production, intracellular parasitism, or the metabolic cost of sustained immune activation. This explains the profound fatigue that characterizes most chronic infectious conditions.
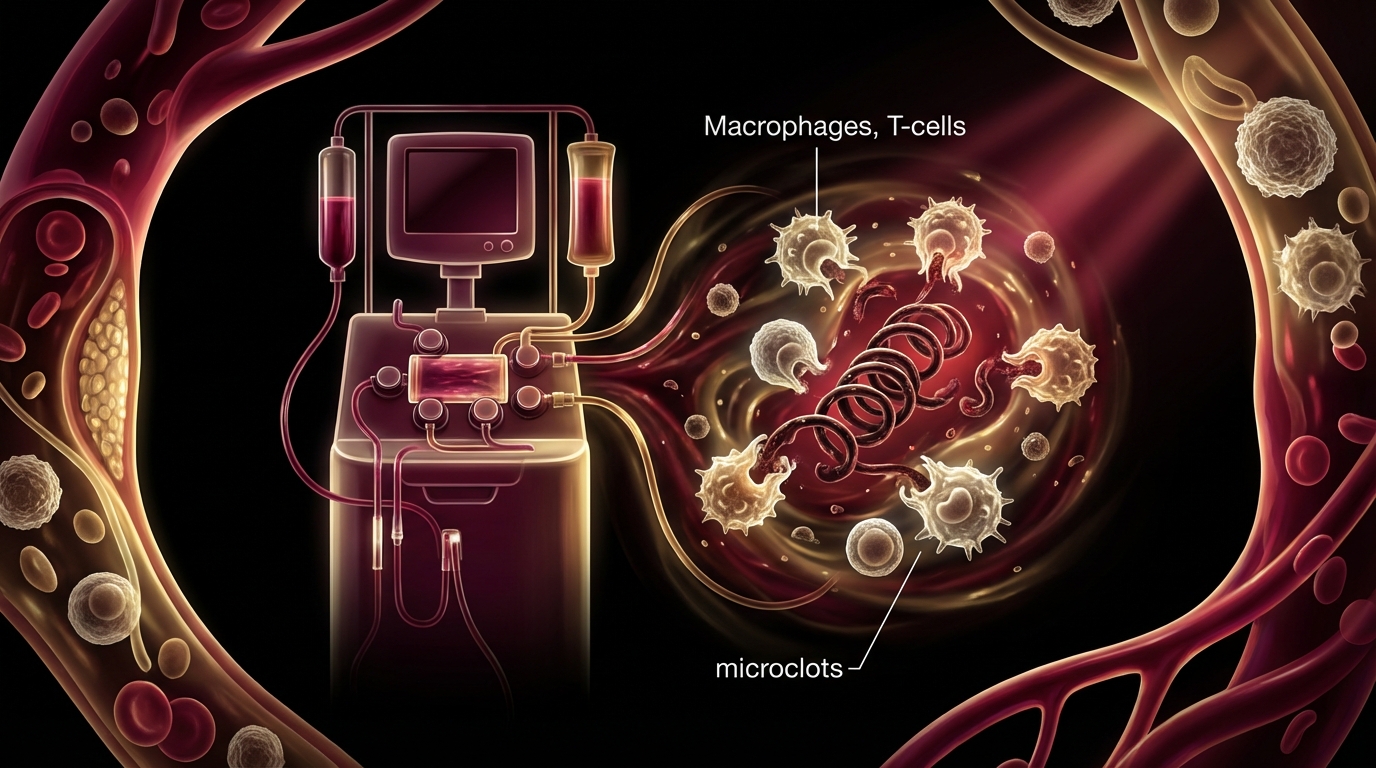
Endothelial damage. Chronic infections can damage blood vessel linings, impairing microcirculation. This is particularly relevant in post-COVID, where Dr. Beate Jaeger’s research on microclots and endothelial dysfunction has provided important insights into the mechanism of persistent symptoms.
Neuroinflammation. Many chronic pathogens — Borrelia, Bartonella, EBV, SARS-CoV-2 — can trigger neuroinflammation directly or indirectly, producing the cognitive symptoms (“brain fog”) that patients find so distressing.
A Physician’s Approach
After decades of treating complex infectious patients — first alongside my late father, Dr. Friedrich Douwes, who was a pioneer in integrative infectiology, and now leading these programs myself — I have developed an approach that differs from both conventional infectious disease practice and purely alternative medicine.
Diagnostic Thoroughness
I do not rely on a single test. My evaluation of a patient with suspected chronic infection includes:
- Comprehensive serological testing with awareness of test limitations
- Specialized testing where available (Elispot/LTT for cellular immune response, advanced PCR, dark-field microscopy)
- Assessment of co-infections — patients with one tick-borne infection frequently carry others (see co-infections overview)
- Evaluation of immune function — not just whether the immune system is fighting the infection, but how effectively
- Assessment of the terrain — mitochondrial function, nutritional status, hormonal balance, toxic burden. The infection exists within a host, and the host’s condition determines the trajectory.
Multimodal Treatment
In my clinical experience, chronic infections rarely respond to a single modality. The most effective treatment programs combine:
- Targeted antimicrobial therapy — antibiotics, antivirals, or antifungals selected based on identified pathogens and their susceptibility
- Biofilm disruption — because biofilm-encased organisms are resistant to antibiotics at standard concentrations
- Immune modulation — supporting the patient’s immune response rather than relying solely on antimicrobials
- Detoxification support — managing the inflammatory and toxic burden from both the infection and its treatment
- Herxheimer reaction management — the intensification of symptoms that can occur when pathogens are killed faster than the body can clear the debris (see Herxheimer article)
- Supportive care — nutritional optimization, mitochondrial support, sleep improvement, stress reduction
Honest Expectations
I want to be direct with patients and readers: chronic infections are treatable, but treatment is often prolonged, non-linear, and requires patience. Some patients achieve complete resolution. Others achieve significant improvement with some residual symptoms. A minority improve slowly or require ongoing management.
The factors that most influence outcome, in my experience:
- Duration of illness before treatment (earlier is better)
- Number and type of co-infections
- Degree of immune compromise
- The patient’s overall health, nutritional status, and capacity for self-care
- Quality and comprehensiveness of the treatment program
What This Series Covers
The articles in this infectiology series address the conditions and concepts that matter most for patients dealing with chronic infectious disease:
- Lyme disease and why patients travel internationally for treatment
- Co-infections (Bartonella, Babesia, Ehrlichia, Mycoplasma, and others)
- Biofilms and persistence mechanisms
- Post-COVID syndrome, including the microclot hypothesis
- Reactivated viruses (EBV, CMV, HHV-6)
- Mold illness and CIRS
- Treatment considerations including Herxheimer reactions, antibiotic resistance, and apheresis
Each article presents the evidence honestly, distinguishes between what we know and what we are still learning, and reflects both published research and the clinical experience accumulated at our facility over decades.
References
- Hodzic E, et al. Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrobial Agents and Chemotherapy. 2008;52(5):1728-1736.
- Marques AR. Laboratory diagnosis of Lyme disease: advances and challenges. Infectious Disease Clinics of North America. 2015;29(2):295-307.
- Bjornevik K, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022;375(6578):296-301.
This content is educational and does not constitute medical advice. Chronic infections require comprehensive evaluation and treatment by a qualified physician experienced in complex infectious disease.