At a Glance
| Property | Value |
|---|---|
| Evidence Level | Strong (large epidemiological studies, exercise physiology RCTs) |
| Primary Use | Mitochondrial biogenesis, cardiovascular longevity, metabolic health |
| Key Mechanism | Selective recruitment of Type I muscle fibers, mitochondrial density increase, fat oxidation |
| Recommended Volume | 150-200 minutes per week (3-4 sessions of 40-60 minutes) |
| Heart Rate Target | Approximately 60-70% of max HR, or the highest intensity at which you can sustain a conversation |
The Exercise Most People Get Wrong
If I had to choose one exercise modality for a patient who wanted to live longer, it would not be high-intensity interval training. It would not be CrossFit. It would not be marathon running. It would be Zone 2 training — and it would not be close.
This is counterintuitive for many patients. Zone 2 feels easy. It feels like you are not working hard enough. Patients come to me having spent years doing intense bootcamps and HIIT classes, exhausted and injured, and they are skeptical when I tell them to slow down. But the evidence is clear: the aerobic base built through Zone 2 training is the single most important determinant of cardiovascular longevity, and most people are profoundly undertrained in this zone.
What Zone 2 Actually Is
Exercise physiologists divide training intensity into zones based on metabolic thresholds. The specific numbering varies by system, but the concept is consistent.
Zone 2 is the highest intensity at which your body can primarily rely on fat oxidation for fuel, with lactate production remaining at or near baseline (below approximately 2 mmol/L). It represents the intensity at which Type I (slow-twitch) muscle fibers are preferentially recruited and mitochondrial fat oxidation is maximized [1].
Practically, Zone 2 is the pace at which you can sustain a conversation — not effortlessly, but without gasping. If you are speaking in full sentences comfortably, you may be in Zone 1. If you can only manage a few words between breaths, you have crossed into Zone 3.
For most people, Zone 2 corresponds to approximately 60-70% of maximum heart rate, though this varies with fitness level, age, and individual physiology. A lactate meter provides the most precise determination, but the talk test is remarkably reliable for practical purposes.
The Mitochondrial Argument
Here is why Zone 2 matters for longevity, and why it is fundamentally different from higher-intensity training.
Zone 2 exercise selectively stresses Type I muscle fibers — the oxidative, mitochondria-rich fibers that rely on aerobic metabolism. When you train these fibers at appropriate intensity and sufficient volume, you trigger a cascade of adaptations [2]:
Mitochondrial biogenesis: PGC-1alpha, the master regulator of mitochondrial production, is activated. Over weeks and months, the mitochondrial density within Type I fibers increases. More mitochondria means greater capacity to produce ATP from fat oxidation — the most efficient and sustainable energy pathway.
Improved fat oxidation: As mitochondrial density increases, the capacity to utilize fatty acids as fuel improves. This spares glycogen, reduces lactate accumulation at any given workload, and fundamentally shifts metabolic efficiency. A well-trained aerobic system burns fat at intensities where an untrained system would already be relying on glucose.
Capillary density: Zone 2 training stimulates angiogenesis — the formation of new capillaries in trained muscle. Greater capillary density means improved oxygen delivery, better nutrient exchange, and enhanced waste removal at the tissue level.
Cardiac efficiency: Sustained moderate-intensity training increases stroke volume — the amount of blood the heart ejects per beat. This reduces resting heart rate and means the heart works less for the same cardiac output. Resting heart rate is an independent predictor of cardiovascular mortality [3].
Higher-intensity training (Zone 4, Zone 5) preferentially recruits Type II (fast-twitch) fibers, which are glycolytic rather than oxidative. These fibers have fewer mitochondria and rely on anaerobic metabolism. HIIT produces cardiovascular benefits and improves VO2 max through different mechanisms (primarily central cardiac adaptations and anaerobic capacity), but it does not produce the same mitochondrial density improvements in Type I fibers that Zone 2 training does.
This is not an argument against high-intensity training. It is an argument that Zone 2 must come first, and it must comprise the majority of training volume. The 80/20 principle observed in elite endurance athletes — 80% of training at low intensity, 20% at high intensity — is not an accident. It is the distribution that maximizes aerobic development while allowing recovery [4].
The Longevity Evidence
Cardiovascular Fitness and Mortality
The relationship between cardiorespiratory fitness (CRF) and all-cause mortality is among the most robust findings in all of preventive medicine. Multiple large prospective studies have demonstrated a dose-response relationship: higher fitness equals lower mortality, with no observed upper ceiling of benefit in the general population.
The HUNT study, following over 55,000 adults for more than 15 years, found that individuals in the highest fitness tertile had approximately 50% lower all-cause mortality compared to those in the lowest tertile [5]. The Cleveland Clinic study by Mandsager et al., analyzing over 122,000 exercise stress tests, found that extreme fitness was associated with the lowest mortality risk, and that low fitness was a stronger predictor of death than diabetes, smoking, or coronary artery disease [6].
Zone 2 training is the primary driver of the aerobic base that determines CRF. While VO2 max — the gold standard measure of CRF — is influenced by both central (cardiac) and peripheral (muscular) factors, the peripheral adaptations driven by Zone 2 training are essential for both VO2 max and for the metabolic efficiency that sustains cardiovascular health over decades.
Metabolic Health
Zone 2 training directly improves the metabolic parameters most associated with longevity:
Insulin sensitivity: Regular Zone 2 exercise improves insulin sensitivity through both acute (GLUT4 translocation) and chronic (improved mitochondrial fat oxidation, reduced ectopic fat) mechanisms. This effect is independent of weight loss [7].
Lipid profile: Consistent aerobic training reduces triglycerides, increases HDL cholesterol, and shifts LDL particle size toward the less atherogenic large buoyant phenotype.
Blood pressure: Moderate-intensity aerobic exercise produces clinically meaningful reductions in both systolic and diastolic blood pressure, with effects comparable to single-agent antihypertensive medication in mild hypertension [8].
Body composition: While Zone 2 is not the most efficient exercise for acute fat loss, it is the most sustainable and produces cumulative effects on body composition through improved fat oxidation capacity and metabolic rate.
Cognitive Protection
Aerobic fitness is strongly associated with cognitive function and reduced risk of dementia. The mechanisms include increased cerebral blood flow, enhanced BDNF production, improved glucose metabolism in the brain, and reduced neuroinflammation. A 2020 meta-analysis found that aerobic exercise reduced the risk of dementia by approximately 28% and Alzheimer’s disease by approximately 45% [9].
What I Tell My Patients
How to Determine Your Zone 2
The simplest method is the talk test: exercise at an intensity where you can speak in full sentences but would rather not sing. If you use a heart rate monitor, start with 180 minus your age as a rough upper limit (the Maffetone formula), and adjust based on how the talk test feels.
For patients who want precision, I recommend a lactate meter. Exercise at increasing intensities and measure blood lactate at each step. Zone 2 is the highest intensity at which lactate remains below approximately 2 mmol/L. In my experience, patients are often surprised — their Zone 2 pace is typically slower than they expect.
This is important. Many patients think they are doing Zone 2 when they are actually in Zone 3 or higher. Training too hard eliminates the specific mitochondrial adaptations that make Zone 2 valuable. Slower is not lazier — it is more precise.
Programming Recommendations
Minimum effective dose: 150 minutes per week of Zone 2 training, spread across at least 3 sessions. This aligns with WHO physical activity guidelines and produces measurable cardiovascular and metabolic benefits.
Optimal dose for longevity: 180-240 minutes per week. This is the range I prescribe for patients focused on longevity and biological age optimization. Four sessions of 45-60 minutes is a practical structure.
Modality: Walking (uphill or brisk), cycling, swimming, rowing, or elliptical. The specific activity matters less than the intensity and duration. I encourage patients to choose activities they enjoy and can sustain year-round. Cycling and walking are particularly well-suited because they allow precise heart rate control.
Progression: Start where you are. If 30 minutes of walking at Zone 2 heart rate is your current capacity, begin there and add 5-10 minutes per week. Do not increase intensity — increase duration. The aerobic base takes months to build, and patience pays dividends.
Integration with strength training: Zone 2 and resistance training are complementary, not competing. I recommend 3-4 Zone 2 sessions and 2-3 strength sessions per week for comprehensive longevity programming. Strength training preserves muscle mass and bone density — both critical for healthspan — while Zone 2 builds the cardiovascular and metabolic foundation.
Common Mistakes
Training too intensely: This is the most common error. Patients equate suffering with effectiveness. Zone 2 should feel sustainable, even boring. If you finish a session exhausted, you were not in Zone 2.
Not enough volume: A 20-minute Zone 2 session once a week produces minimal adaptation. The dose-response curve favors consistent, moderate-duration sessions. Three to four sessions per week of 40-60 minutes is the target.
Ignoring progression over months: The beauty of Zone 2 training is that your pace at the same heart rate gradually increases. After six months of consistent training, you will be walking or cycling significantly faster at the same Zone 2 heart rate. This reflects genuine mitochondrial and cardiovascular adaptation — and it is one of the most satisfying biomarkers to track.
Neglecting strength training: Zone 2 alone is not a complete longevity exercise program. Without resistance training, you will lose muscle mass with age, and sarcopenia is a major driver of disability and mortality. Both modalities are essential.
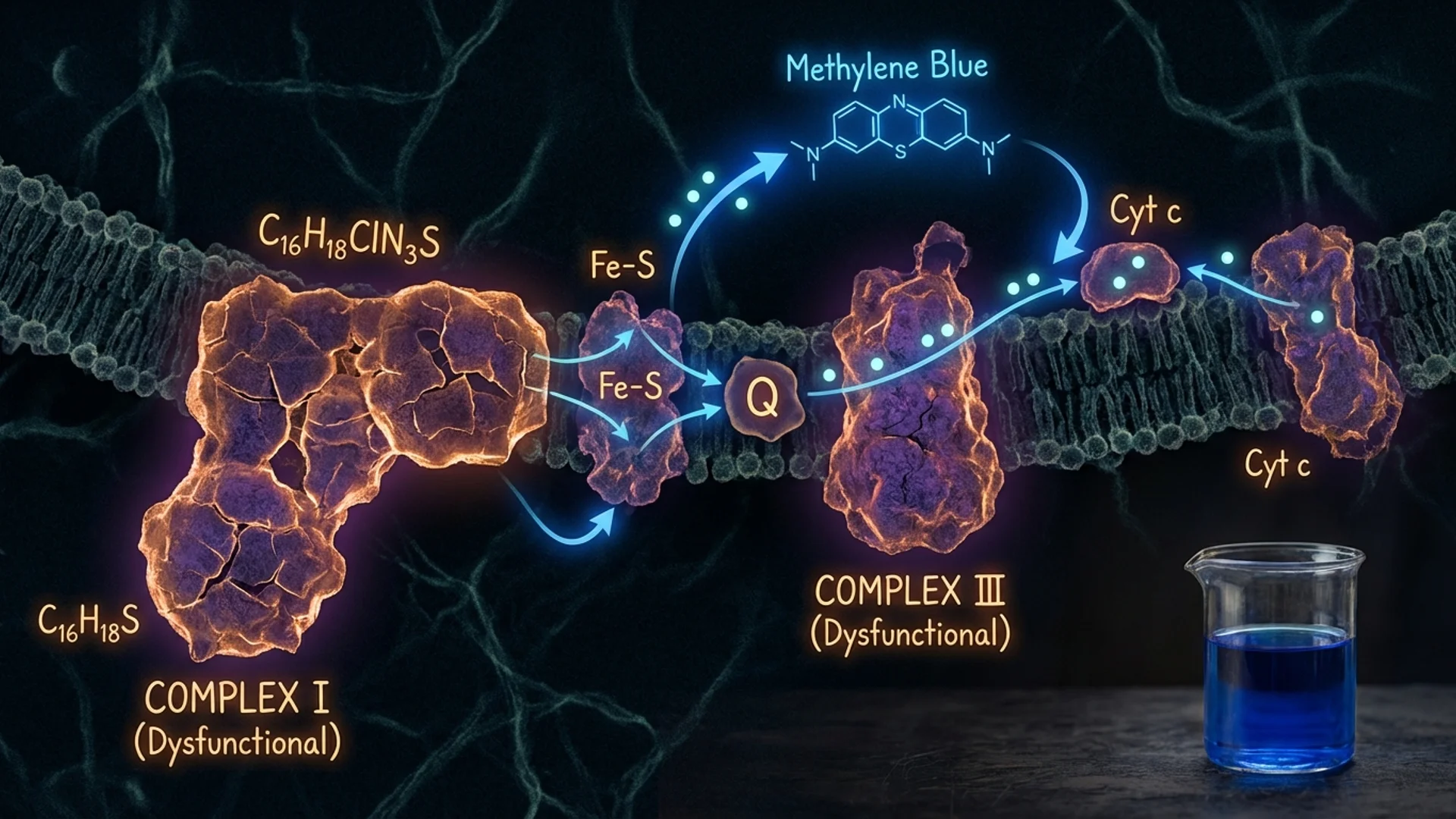
Zone 2 and Mitochondrial Health
The connection between Zone 2 training and mitochondrial function deserves emphasis. In patients with chronic fatigue, post-COVID syndrome, or documented mitochondrial dysfunction and cellular energy, Zone 2 training is both a diagnostic tool and a therapeutic intervention.
Diagnostically, a patient who cannot sustain a conversation at even low exercise intensities — whose lactate rises above 2 mmol/L at minimal workloads — has objective evidence of impaired oxidative metabolism. This is clinically useful information.
Therapeutically, gentle Zone 2 training (even if it means very slow walking initially) stimulates the very pathways that rebuild mitochondrial capacity. For these patients, I often combine Zone 2 training with IHHT and targeted mitochondrial support (CoQ10 for mitochondrial support, NAD+ precursors, B vitamins) to address mitochondrial dysfunction from multiple angles.
In my clinical experience, patients who commit to consistent Zone 2 training — even when starting from a severely deconditioned state — show meaningful improvements in lactate threshold, exercise tolerance, and subjective energy over 8-16 weeks. The progress is gradual, but it is real and measurable.
Safety and Considerations
Zone 2 training is among the safest forms of exercise. The intensity is moderate, the cardiovascular stress is manageable, and the injury risk is low. However:
- Patients with known cardiovascular disease should undergo exercise testing and receive clearance before beginning a training program
- Patients on beta-blockers cannot rely on heart rate to determine Zone 2 — perceived exertion and the talk test become primary guides
- Patients with orthopedic limitations may need to select low-impact modalities (cycling, swimming, or pool walking rather than running)
- In severely deconditioned patients, even slow walking may initially exceed Zone 2 — starting with very short sessions and building gradually is appropriate
The Bottom Line
Zone 2 training is the foundation of cardiovascular longevity. It builds mitochondrial density, improves fat oxidation, enhances cardiac efficiency, and directly addresses the metabolic dysfunction that drives cardiovascular disease, diabetes, and cognitive decline. The evidence linking cardiorespiratory fitness to reduced all-cause mortality is among the strongest in all of medicine.
What I tell my patients: if you are only going to do one type of exercise, make it Zone 2. It should feel easy. It should be sustainable. And you need more of it than you think. Three to four sessions per week, 45-60 minutes each, at a conversational pace. That is the prescription. It is simple, and it works.
References
- San-Millan I, Brooks GA. Assessment of metabolic flexibility by means of measuring blood lactate, fat, and carbohydrate oxidation responses to exercise in professional endurance athletes and less-fit individuals. Sports Med. 2018;48(2):467-479. PMID: 28623613.
- Hood DA, Memme JM, Oliveira AN, Triolo M. Maintenance of skeletal muscle mitochondria in health, exercise, and aging. Annu Rev Physiol. 2019;81:19-41. PMID: 30216742.
- Zhang D, Shen X, Qi X. Resting heart rate and all-cause and cardiovascular mortality in the general population: A meta-analysis. CMAJ. 2016;188(3):E53-E63. PMID: 26598376.
- Seiler S. What is best practice for training intensity and duration distribution in endurance athletes? Int J Sports Physiol Perform. 2010;5(3):276-291. PMID: 20861519.
- Nes BM, Vatten LJ, Nauman J, Janszky I, Wisloff U. A simple nonexercise model of cardiorespiratory fitness predicts long-term mortality. Med Sci Sports Exerc. 2014;46(6):1159-1165. PMID: 24576863.
- Mandsager K, Harb S, Cremer P, et al. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1(6):e183605. PMID: 30646252.
- Bird SR, Hawley JA. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc Med. 2017;2(1):e000143. PMID: 28879026.
- Cornelissen VA, Smart NA. Exercise training for blood pressure: A systematic review and meta-analysis. J Am Heart Assoc. 2013;2(1):e004473. PMID: 23525435.
- Xu W, Wang HF, Wan Y, et al. Leisure time physical activity and dementia risk: A dose-response meta-analysis of prospective studies. BMJ Open. 2017;7(10):e014706. PMID: 29025833.