At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate (strong mechanistic data, growing human trials) |
| Primary Use | Metabolic health, biological age reduction, autophagy activation |
| Key Mechanism | Nutrient deprivation triggers AMPK, sirtuins, and autophagy pathways |
| Recommended Protocol | 16:8 or 18:6 time-restricted eating as foundation; periodic extended fasts individualized |
| Who Should Avoid | Underweight patients, active eating disorders, pregnancy, uncontrolled diabetes |
Why Does Everyone Keep Talking About Fasting?
Patients ask me about intermittent fasting more than almost any other longevity intervention. Usually the question comes in one of two forms: “Should I be doing it?” or “I’ve been doing 16:8 for six months — is it actually helping?”
Here is what the evidence shows. Intermittent fasting is not a fad. The biological pathways it activates are among the most well-characterized in aging research. But the gap between what we know mechanistically and what we can prove in human longevity trials is still significant, and that nuance matters.
Let me walk through what we actually know, what remains uncertain, and how I apply this in clinical practice.
The Biology: What Happens When You Stop Eating
When food intake stops, the body undergoes a predictable sequence of metabolic shifts. Understanding this timeline is essential for understanding why fasting duration matters.
0-12 hours: Glycogen stores in the liver are gradually depleted. Insulin levels fall. Glucagon rises. The body transitions from glucose-dominant to increasingly fat-dominant fuel metabolism.
12-18 hours: With glycogen largely depleted, hepatic ketogenesis accelerates. Beta-hydroxybutyrate (BHB) levels rise. BHB is not merely an alternative fuel — it is a signaling molecule that inhibits HDAC enzymes, modulates gene expression, and has direct anti-inflammatory properties [1].
18-24 hours: Autophagy becomes significantly upregulated. AMPK activation is robust. Sirtuins — particularly SIRT1 and SIRT3 — are activated, supporting mitochondrial function and DNA repair. mTOR pathway and longevity activity is suppressed, shifting the cellular program from growth toward maintenance and repair [2].
24-48 hours: Autophagy deepens. In animal models, this is where measurable clearance of damaged organelles, misfolded proteins, and dysfunctional mitochondria becomes most pronounced. Growth hormone secretion increases — a counterintuitive but well-documented response that helps preserve lean mass during nutrient deprivation [3].
Beyond 48 hours: Immune system remodeling begins. Valter Longo’s research at USC has shown that prolonged fasting (48-72 hours) triggers regeneration of hematopoietic stem cells and a form of immune system “reset” [4]. This is compelling data, but prolonged fasts carry real risks and should only be undertaken with medical supervision.
The critical point: the longevity-relevant benefits of fasting — autophagy, mitochondrial quality control, reduced inflammation, improved insulin sensitivity — do not require starvation. They begin to activate in the 16-24 hour window that most intermittent fasting protocols target.
The Evidence for Longevity
What We Know From Animal Studies
Caloric restriction has been the most consistently replicated intervention for extending lifespan in laboratory animals. Across species — yeast, worms, flies, mice, rats — reducing caloric intake by 20-40% extends lifespan and delays the onset of age-related disease. This has been demonstrated in hundreds of studies spanning decades [5].
Intermittent fasting, independent of total caloric reduction, produces many of the same benefits. Mice on intermittent fasting protocols live longer, have lower rates of cancer, better glucose regulation, and reduced neurodegeneration compared to ad libitum-fed controls — even when total caloric intake is similar between groups [6].
This is an important distinction. It suggests that the timing of food intake matters independently of how much you eat. The metabolic switching between fed and fasted states appears to be beneficial in itself.
The NIA Interventions Testing Program — one of the most rigorous multi-site programs in aging research — has confirmed lifespan extension with caloric restriction in genetically diverse mouse populations, adding confidence that the effect is robust rather than strain-specific [7].
What We Know From Human Data
Let me be direct: we do not have a completed randomized controlled trial demonstrating that intermittent fasting extends human lifespan. Such a trial would take decades and faces obvious practical challenges. What we have instead is a combination of mechanistic data, metabolic biomarker studies, and observational research.
The CALERIE trial is the most rigorous human caloric restriction study completed to date. Participants who maintained approximately 12% caloric restriction over two years showed a significant reduction in the pace of biological aging as measured by the DunedinPACE epigenetic clock [8]. While this was caloric restriction rather than intermittent fasting specifically, it demonstrates that dietary interventions can measurably slow the pace of human aging at the epigenetic level.
Time-restricted eating (TRE) studies in humans consistently show improvements in metabolic parameters. A 2022 meta-analysis of 27 randomized controlled trials found that TRE improved fasting glucose, insulin resistance (HOMA-IR), triglycerides, and inflammatory markers compared to unrestricted eating [9]. These are not longevity endpoints, but they are established risk factors for the diseases that kill most people.
The TREAT trial, a randomized controlled study of 16:8 TRE, showed modest weight loss but raised concern about lean mass reduction. This finding has been debated — the study had limitations in protein intake assessment and exercise control — but it underscores an important point: fasting protocols must be combined with adequate protein intake and resistance training to preserve muscle mass. In my longevity patients, I am explicit about this.
What I See in Practice
In clinical practice, intermittent fasting is one of the most accessible and consistently beneficial interventions for metabolic health and biological age optimization. At our clinic, we observe the following patterns across patients:
Patients who adopt a consistent 16:8 or 18:6 eating pattern typically show improvements in fasting insulin, HOMA-IR, triglycerides, and inflammatory markers (hsCRP, IL-6) within 8-12 weeks. These improvements are often measurable before significant weight loss occurs, suggesting metabolic benefits independent of body composition changes.
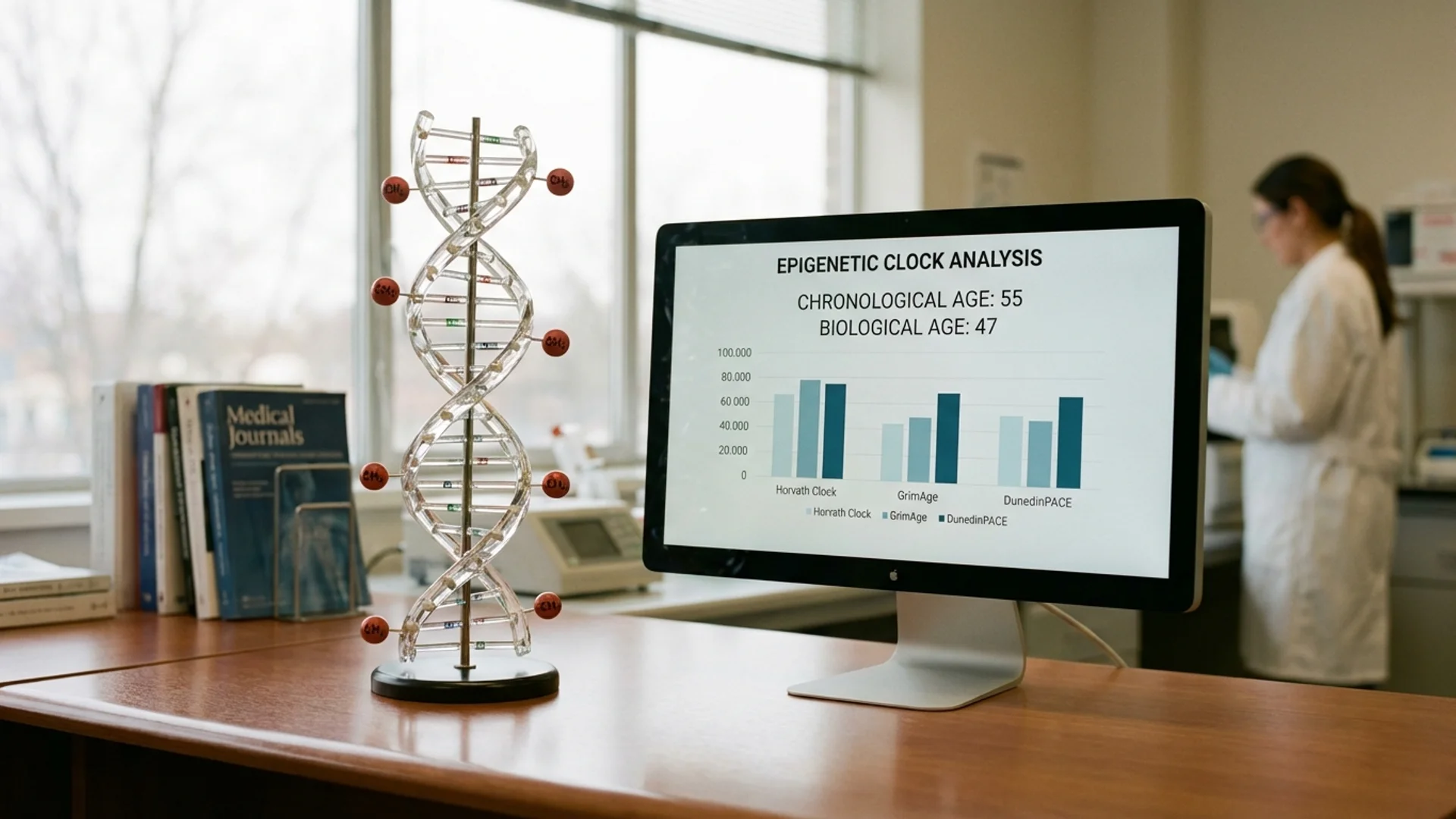
In patients undergoing serial biological age testing — using epigenetic clocks such as GrimAge or DunedinPACE — those who combine time-restricted eating with other longevity interventions consistently show more favorable biological aging trajectories than those who do not.
I have also observed patients for whom fasting is clearly counterproductive: those with existing adrenal dysfunction, underweight patients, patients with a history of eating disorders, and some women in perimenopause who experience worsened hormonal symptoms with extended fasting windows. Fasting is a tool, not a religion. It must be individualized.
Practical Application
What I Recommend to My Patients
Foundation protocol — Time-restricted eating (16:8 or 18:6):
This is the simplest and most sustainable approach. Eat within an 8-hour window (e.g., 10:00 to 18:00) or a 6-hour window for those who tolerate it well. The remaining hours are a fasting window in which only water, black coffee, or unsweetened tea are consumed.
I tell my patients: consistency matters more than perfection. Five days per week of 16:8 is more valuable than occasional 24-hour fasts followed by weeks of unrestricted eating.
Protein prioritization:
This is non-negotiable. In every fasting protocol, I require patients to maintain adequate protein intake — minimum 1.2 g/kg body weight, preferably 1.6 g/kg — within their eating window. The longevity benefit of fasting is substantially undermined if you lose muscle mass in the process. Sarcopenia is a major driver of mortality in older adults, and any longevity strategy that accelerates muscle loss is self-defeating.
Periodic extended fasts (optional, supervised):
For motivated patients with appropriate health status, I occasionally recommend 24-36 hour water fasts once or twice monthly. These deeper fasts appear to activate autophagy more robustly than daily TRE alone. I require blood glucose monitoring, adequate hydration with electrolytes, and clear stop criteria for any extended fast.
What to eat — the feeding window matters:
Fasting is not a license to eat poorly during the feeding window. The metabolic benefits of TRE are amplified when combined with a nutrient-dense diet: adequate protein, healthy fats, abundant vegetables, and limited refined carbohydrates. A patient doing 16:8 but consuming processed food during the feeding window will see diminished returns.
Combining Fasting With Other Longevity Interventions
Intermittent fasting synergizes with several other longevity strategies:
- Exercise: Fasted training (particularly Zone 2 aerobic work) appears to enhance mitochondrial adaptations. However, high-intensity sessions benefit from pre-workout fueling. I recommend fasted Zone 2 training in the morning and fueled strength training later in the day.
- NAD+ support: Fasting activates sirtuins, which require NAD+ as a cofactor. Ensuring adequate NAD+ status may amplify the benefits of fasting.
- [Senolytic protocols](/longevity/senolytic therapy for agings/): Some emerging evidence suggests that fasting may enhance senolytic efficacy by sensitizing senescent cells to clearance.
- Sleep optimization: Finishing the last meal 3-4 hours before sleep improves sleep quality, which in turn supports the overnight repair processes that fasting facilitates.
Safety and Considerations
Intermittent fasting is generally safe for healthy adults, but it is not appropriate for everyone.
Contraindications:
- Active eating disorders or history of disordered eating
- Underweight (BMI < 18.5) or significant muscle wasting
- Pregnancy or breastfeeding
- Type 1 diabetes or insulin-dependent diabetes without medical supervision
- Children and adolescents
Precautions:
- Women in perimenopause may need shorter fasting windows (14:10 rather than 18:6) — extended fasting can worsen cortisol dysregulation in some women
- Patients on diabetes medications (metformin for longevity, sulfonylureas, insulin) require dose adjustment and monitoring
- Patients with adrenal insufficiency or severe chronic fatigue should approach fasting cautiously
- Hydration and electrolyte balance must be maintained, particularly during extended fasts
Side effects in the first 1-2 weeks: Headaches, irritability, difficulty concentrating, and mild hunger are common during adaptation. They typically resolve. If they persist beyond two weeks, the protocol needs adjustment.
Common Misconceptions
“Fasting puts you in starvation mode.” The metabolic slowdown associated with chronic caloric restriction (reduced resting metabolic rate, hormonal suppression) is well-documented. But intermittent fasting — particularly time-restricted eating — does not produce the same effect because total caloric intake is maintained. The metabolic response to 16 hours of fasting followed by adequate feeding is fundamentally different from weeks of sustained caloric deficit [10].
“You need to eat breakfast to be healthy.” The observational data associating breakfast skipping with poor health outcomes is confounded by the fact that people who skip breakfast tend to have worse overall dietary habits, higher rates of smoking, and less physical activity. When these confounders are controlled for, the association weakens substantially. The quality and timing of your overall dietary pattern matters far more than whether you eat within 30 minutes of waking.
“Longer fasts are always better.” They are not. For most people, the practical benefit-to-risk ratio favors daily TRE (16:8) with occasional extended fasts, not chronic multi-day fasting. Prolonged fasting without medical supervision carries real risks: electrolyte imbalances, muscle catabolism, refeeding syndrome, and psychological distress.
The Bottom Line
Intermittent fasting activates cellular repair mechanisms — autophagy, mitochondrial quality control, sirtuin activation — that are directly relevant to biological aging. The human metabolic data is strong, and emerging epigenetic data suggests measurable slowing of the aging process. We do not yet have human lifespan data, and we may never have a perfect trial, but the convergence of mechanistic, animal, and human biomarker evidence makes intermittent fasting one of the most evidence-supported longevity interventions available.
What I tell my patients: start with 16:8. Prioritize protein. Combine it with exercise and adequate sleep. Do not make it more complicated than it needs to be. The most effective fasting protocol is one you can sustain for years, not the most extreme one you can tolerate for a week.
References
- Shimazu T, Hirschey MD, Newman J, et al. Suppression of oxidative stress by beta-hydroxybutyrate, an endogenous histone deacetylase inhibitor. Science. 2013;339(6116):211-214. PMID: 23223453.
- Bagherniya M, Butler AE, Barreto GE, Sahebkar A. The effect of fasting or calorie restriction on autophagy induction: A review of the literature. Ageing Res Rev. 2018;47:183-197. PMID: 30172870.
- Hartman ML, Veldhuis JD, Johnson ML, et al. Augmented growth hormone secretory burst frequency and amplitude mediate enhanced GH secretion during a two-day fast in normal men. J Clin Endocrinol Metab. 1992;74(4):757-765. PMID: 1548337.
- Cheng CW, Adams GB, Perin L, et al. Prolonged fasting reduces IGF-1/PKA to promote hematopoietic-stem-cell-based regeneration and reverse immunosuppression. Cell Stem Cell. 2014;14(6):810-823. PMID: 24905167.
- Fontana L, Partridge L, Longo VD. Extending healthy life span — from yeast to humans. Science. 2010;328(5976):321-326. PMID: 20395504.
- Mattson MP, Longo VD, Harvie M. Impact of intermittent fasting on health and disease processes. Ageing Res Rev. 2017;39:46-58. PMID: 28235195.
- Harrison DE, Strong R, Allison DB, et al. Acarbose, 17-alpha-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males. Aging Cell. 2014;13(2):273-282. PMID: 24245565.
- Waziry R, Ryan CP, Corcoran DL, et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging: CALERIE trial analysis. Nat Aging. 2023;3(3):248-257. PMID: 37118425.
- Patikorn C, Roubal K, Veettil SK, et al. Intermittent fasting and obesity-related health outcomes: An umbrella review of meta-analyses of randomized clinical trials. JAMA Netw Open. 2021;4(12):e2139558. PMID: 34919135.
- Heilbronn LK, Smith SR, Martin CK, et al. Alternate-day fasting in nonobese subjects: effects on body weight, body composition, and energy metabolism. Am J Clin Nutr. 2005;81(1):69-73. PMID: 15640462.