If you are researching NAD+ supplementation, you have probably encountered three options: direct NAD+ IV infusion, NMN (nicotinamide mononucleotide), and NR (nicotinamide riboside). The internet is full of passionate advocates for each one. Social media influencers push NMN capsules. Longevity clinics market NAD+ IVs as the gold standard. Supplement companies point to NR’s published human data.
Here is what the evidence actually says — and what I recommend in clinical practice based on treating patients who are serious about optimizing their NAD+ levels.
At a Glance
| Property | NAD+ IV | NMN (Oral) | NR (Oral) |
|---|---|---|---|
| Evidence Level | Moderate (clinical observation, limited RCTs) | Moderate (growing human trial data) | Moderate (most published human RCTs) |
| Bioavailability | ~100% (direct systemic) | Variable (30-50% estimated, route debated) | ~30-50% (hepatic first-pass metabolism) |
| Peak NAD+ Elevation | Highest (supraphysiological) | Moderate | Moderate |
| Onset | Minutes to hours | Hours to days | Hours to days |
| Cost | $250-1,000 per session | $50-150/month | $40-120/month |
| Convenience | Requires clinical setting | Daily oral capsule | Daily oral capsule |
| Best For | Acute restoration, intensive protocols | Daily maintenance, research-oriented users | Daily maintenance, conservative users |
Why NAD+ Matters — A Quick Refresher
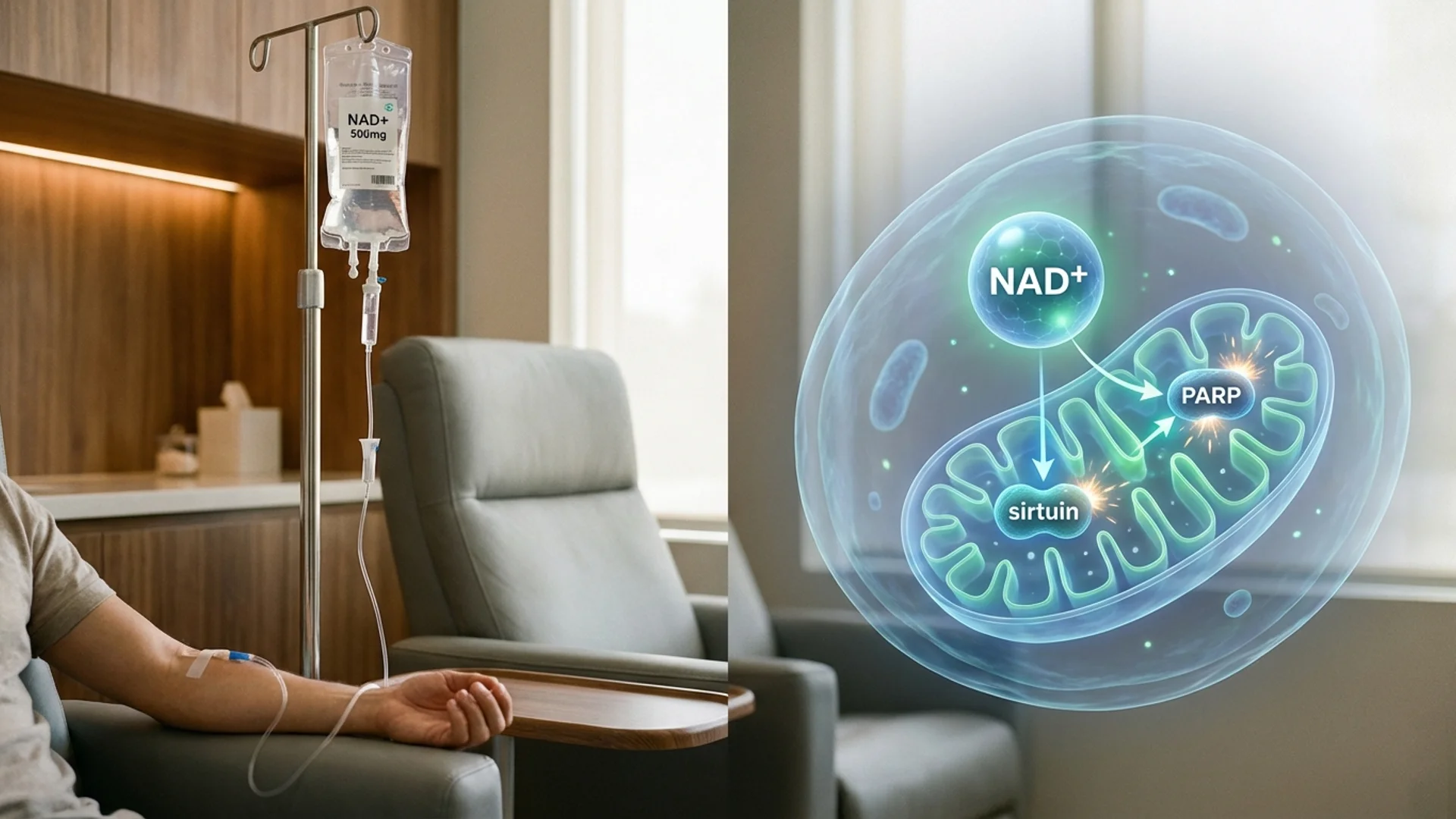
I covered the biochemistry of NAD+ in depth in my NAD+ IV therapy article, but the essential point bears repeating: NAD+ is a coenzyme required for over 500 enzymatic reactions including mitochondrial energy production, sirtuin-mediated DNA repair, and PARP-dependent genomic maintenance. By age 50, intracellular NAD+ levels may decline by approximately 50% [1].
The clinical question is not whether NAD+ decline matters — it does. The question is what the most effective, evidence-based approach to restoring NAD+ levels is. That is where the three options diverge.
NAD+ IV: Direct Delivery
How It Works
Intravenous NAD+ delivers the molecule directly into the bloodstream, bypassing gastrointestinal absorption entirely. There is no first-pass hepatic metabolism, no intestinal degradation, and no debate about whether the molecule survives transit. What goes into the vein reaches systemic circulation.
A typical infusion protocol delivers 250-1,000 mg of NAD+ over 2-4 hours. The infusion rate matters — pushing it too fast causes uncomfortable flushing, nausea, and chest tightness. In my practice, we titrate carefully, starting slowly and increasing as tolerated.
The Evidence
Let me be direct about the evidence landscape. Most published research on NAD+ repletion in humans has used oral precursors (NMN or NR), not direct IV NAD+. The clinical evidence for IV NAD+ specifically comes primarily from:
- Addiction and withdrawal studies: IV NAD+ has been used in addiction medicine for decades, with clinical reports suggesting reduced withdrawal symptoms and improved cognitive clarity [2]. These studies are largely observational and methodologically limited, but they provide safety data and proof of concept for tolerability.
- Clinical observation: In my experience, patients receiving IV NAD+ report consistent improvements in mental clarity, energy, and subjective wellbeing within hours of infusion. This is anecdotal, and I am transparent about that distinction — but when you observe the same pattern in hundreds of patients, it becomes a clinically relevant observation.
- Pharmacokinetic data: IV delivery achieves plasma NAD+ concentrations that oral precursors simply cannot match. Whether these supraphysiological peaks are necessary for clinical benefit has not been determined in controlled trials.
Advantages
The primary advantage is certainty of delivery. There is no absorption question, no bioavailability debate, and no uncertainty about whether the molecule reaches the bloodstream intact. Peak levels are higher and onset is faster than any oral approach.
For patients presenting with significant fatigue, cognitive decline, or those undergoing intensive treatment protocols for conditions like post-COVID or chronic infections, IV NAD+ provides a rapid, reliable restoration that oral supplements cannot match on the same timeline.
Limitations
Cost is the obvious barrier. A single IV NAD+ session costs between $250 and $1,000 depending on the dose and the clinic. It requires a clinical setting, trained staff, and 2-4 hours per session. This is not a daily intervention — it is a periodic intensive one.
The infusion itself can be uncomfortable. Flushing, nausea, abdominal cramping, and a distinctive chest pressure are common when the rate is too high. These are not dangerous, but they require an experienced clinical team that knows how to manage infusion rates.
NMN: The Rising Contender
How It Works
Nicotinamide mononucleotide (NMN) is a direct precursor to NAD+. The enzyme that converts NMN to NAD+ — nicotinamide mononucleotide adenylyltransferase (NMNAT) — is present in every cell. In theory, providing NMN bypasses the rate-limiting step of NAD+ synthesis (the conversion of NAM to NMN by NAMPT) and allows rapid NAD+ production.
The bioavailability question has been debated intensely. For years, scientists questioned whether NMN could cross the intestinal barrier intact. In 2019, the discovery of the Slc12a8 transporter suggested a direct uptake pathway in the small intestine [3], though this finding has been challenged. More recently, human pharmacokinetic studies have confirmed that oral NMN does increase blood and tissue NAD+ levels in a dose-dependent manner [4].
The Evidence
NMN has accumulated meaningful human trial data in recent years:
- Yi et al. (2023): A randomized, double-blind, placebo-controlled trial in middle-aged adults demonstrated that 300 mg/day NMN for 60 days significantly increased blood NAD+ levels and improved physical performance metrics [4].
- Liao et al. (2021): A human RCT showed that oral NMN supplementation (250 mg/day) increased NAD+ metabolite levels and was well tolerated over 12 weeks [5].
- Igarashi et al. (2022): A study in older men demonstrated that 250 mg NMN daily improved muscle insulin sensitivity and remodeling, though the sample size was small (n=25) [6].
- Kim et al. (2022): NMN supplementation improved sleep quality and reduced drowsiness in older adults in a randomized controlled trial [7].
The evidence is moderate and growing. Multiple human RCTs confirm that oral NMN raises NAD+ levels. What remains less clear is whether these elevations translate to clinically meaningful improvements in aging outcomes over the long term. We do not yet have multi-year human longevity data.
Advantages
Convenience and cost are the primary advantages. NMN is taken orally, once daily, at home. No clinical visit required. Monthly costs range from $50 to $150 depending on the brand and dose.
The research trajectory is favorable. More human trials are published every year, and the mechanistic rationale is sound. NMN also has strong preclinical data — David Sinclair’s laboratory at Harvard has published extensively on NMN’s effects in animal models, demonstrating improvements in vascular health, exercise capacity, and metabolic function [8].
Limitations
Bioavailability remains an area of active research. Not all NMN that reaches the gut is absorbed intact, and the fraction that survives first-pass hepatic metabolism to reach target tissues is uncertain. This matters because the doses used in animal studies, when scaled to humans, suggest that much higher doses may be needed for equivalent tissue effects.
Quality control is a real concern. NMN is sold as a supplement, which means manufacturing standards vary enormously. I have seen patients taking products that, upon independent testing, contained significantly less NMN than advertised — or included contaminants. If you choose oral NMN, third-party testing verification is not optional.
The regulatory landscape is also uncertain. The FDA briefly considered classifying NMN as a drug rather than a supplement, which caused market disruption and continues to create uncertainty about long-term availability.
NR: The Most Studied Oral Precursor
How It Works
Nicotinamide riboside (NR) is converted to NMN by NR kinases (NRK1 and NRK2), and then NMN is converted to NAD+ by NMNAT enzymes. It requires one additional enzymatic step compared to NMN, but the pathway is well characterized and NRK enzymes are widely expressed.
NR has been commercially available longer than NMN and has benefited from earlier and more extensive clinical research, partly due to patent protection and pharmaceutical investment (ChromaDex’s Niagen brand funded several of the key human trials).
The Evidence
NR has the largest body of published human clinical data among oral NAD+ precursors:
- Martens et al. (2018): A crossover RCT demonstrated that NR (1,000 mg/day for 6 weeks) raised NAD+ metabolites by approximately 60% and tended to reduce systolic blood pressure and aortic stiffness in healthy middle-aged and older adults [9].
- Elhassan et al. (2019): NR supplementation (1,000 mg/day) increased skeletal muscle NAD+ metabolites and altered the muscle transcriptome in favor of mitochondrial and anti-inflammatory pathways in older men [10].
- Dollerup et al. (2018): An RCT in obese men showed that NR (2,000 mg/day for 12 weeks) increased NAD+ metabolites but did not significantly alter insulin sensitivity or body composition [11].
- Remie et al. (2020): NR supplementation in healthy overweight adults showed modest metabolic benefits including reduced hepatic lipid accumulation [12].
The data pattern is consistent: NR reliably raises NAD+ levels in humans. The functional benefits, however, are more modest than animal models predicted. This is an important nuance that the supplement industry tends to gloss over.
Advantages
NR has the most regulatory clarity — it has GRAS (Generally Recognized as Safe) status in the United States and a well-established safety profile from multiple clinical trials. For patients who prioritize evidence quantity and regulatory certainty, NR is the most conservative choice.
The safety data is extensive. Side effects in human trials are minimal — mild nausea, fatigue, and headache have been reported, but serious adverse events are rare. This matters when you are recommending something a patient will take daily for years.
Limitations
The additional enzymatic step (NR to NMN to NAD+) may represent a rate limitation, though this has not been conclusively demonstrated in vivo. Some researchers hypothesize that NMN, being one step closer to NAD+, may be more efficient — but head-to-head human comparisons are lacking.
Like NMN, the magnitude of NAD+ elevation achieved with oral NR may not match what IV delivery provides. And the same quality concerns apply to any supplement — though NR has somewhat better standardization due to the dominant branded ingredient (Niagen).
Head-to-Head: What the Comparison Reveals
Bioavailability and Peak Levels
This is where the three approaches diverge most clearly:
NAD+ IV achieves the highest peak plasma NAD+ levels because there is no absorption barrier and no metabolic conversion required. The molecule goes directly into the bloodstream. Peak levels are supraphysiological — meaning they exceed what the body would normally produce on its own.
NMN oral raises blood NAD+ levels dose-dependently, but the absolute elevation is lower than IV delivery. Pharmacokinetic studies suggest measurable increases within 2-4 hours of oral dosing, with sustained elevation over the supplementation period [4].
NR oral produces comparable NAD+ metabolite elevations to NMN at equivalent doses, though direct head-to-head data is limited. The additional enzymatic conversion step has not been shown to be a significant bottleneck in human studies.
Speed of Response
IV NAD+ produces noticeable effects within hours — often during the infusion itself. In my clinical experience, patients consistently report improved mental clarity and energy within the first session.
Oral NMN and NR require days to weeks of consistent supplementation before steady-state NAD+ elevation is achieved. Patients should not expect to feel a difference on day one.
Duration and Sustainability
This is where oral precursors have an advantage. IV NAD+ provides a powerful but transient boost. Without repeated infusions, the benefit diminishes. Oral NMN and NR, taken daily, maintain steady-state NAD+ elevation indefinitely.
The pragmatic approach — and what I recommend in practice — is to combine both strategies.
Cost Comparison
| Approach | Monthly Cost (Typical) | Annual Cost |
|---|---|---|
| NAD+ IV (2x/month) | $500-2,000 | $6,000-24,000 |
| NMN (500 mg/day) | $60-150 | $720-1,800 |
| NR (1,000 mg/day) | $40-120 | $480-1,440 |
| Combination (IV quarterly + daily oral) | ~$200-300 | ~$2,400-3,600 |
What I Use in Clinical Practice
Let me be direct about what I recommend and why.
For acute restoration: I use NAD+ IV. When a patient presents with significant fatigue, cognitive decline, or is undergoing an intensive treatment protocol — whether for post-COVID recovery, chronic Lyme disease, or as part of a longevity optimization program — IV NAD+ provides the most reliable and rapid restoration.
For daily maintenance: I recommend oral NMN or NR. Both are reasonable choices. I have a slight preference for NMN based on its more direct conversion pathway and the trajectory of recent clinical data, but I do not consider NR an inferior choice. What matters more than the specific precursor is consistency of dosing, product quality, and realistic expectations.
My standard protocol:
- Initial loading: 3-5 IV NAD+ sessions (500-1,000 mg per session) over 1-2 weeks
- Transition to oral maintenance: NMN 500-1,000 mg/day or NR 1,000 mg/day
- Periodic IV boosts: Every 3-6 months, particularly during periods of high stress, illness, or intensive treatment
This is a clinical protocol based on my experience and observation. It is not derived from a randomized controlled trial comparing combination approaches to monotherapy. I want to be transparent about that distinction.
Who Benefits Most from Each Approach
NAD+ IV is best for:
- Patients with significant baseline depletion (chronic fatigue, post-COVID, chronic infections)
- Those undergoing intensive treatment protocols
- Patients who want rapid, measurable restoration
- Individuals who can afford periodic clinical visits
NMN is best for:
- Daily maintenance supplementation
- Patients who want the most direct oral precursor pathway
- Research-oriented individuals following the latest trial data
- Those comfortable with a supplement that has less regulatory certainty than NR
NR is best for:
- Conservative patients who prioritize the largest evidence base
- Those who value regulatory clarity (GRAS status)
- Patients on a tighter budget
- Long-term daily supplementation with minimal monitoring concerns
Safety and Considerations
All three approaches have favorable safety profiles based on available data. The most common concerns:
NAD+ IV: Infusion reactions (flushing, nausea, chest tightness) are dose-rate dependent and managed with careful titration. These are not allergic reactions and are not dangerous when properly managed. Rare cases of vein irritation or phlebitis can occur.
NMN: No serious adverse events reported in published human trials at doses up to 1,250 mg/day. Theoretical concern about NAM (nicotinamide) accumulation at very high doses, which could inhibit sirtuins — the opposite of the intended effect. This has not been demonstrated clinically at standard doses.
NR: Well-characterized safety profile from multiple trials. Mild GI symptoms (nausea, bloating) reported in a minority of participants. No serious adverse events at doses up to 2,000 mg/day in published data [11].
Important interactions: High-dose niacin-derived compounds can affect liver function tests. I monitor liver enzymes at baseline and periodically in patients on NAD+ optimization protocols, though clinically significant hepatotoxicity from NMN or NR at standard doses has not been reported.
The Quality Problem
This is what makes me angry about the supplement industry, and I need to say it clearly: the difference between a high-quality NAD+ precursor and a poorly manufactured one is enormous, and most consumers cannot tell the difference.
In my practice, I have seen independent lab analyses of NMN and NR products that showed:
- Products containing 40-60% of the labeled NMN content
- Contamination with nicotinamide (a much cheaper compound)
- Degradation products suggesting poor storage or old inventory
What I tell my patients: if you are going to spend money on oral NAD+ precursors, spend the extra money on a product that provides third-party certificates of analysis. The cheapest NMN on Amazon is not a bargain if it contains half of what the label claims.
For NR, the branded ingredient Niagen (ChromaDex) has the most consistent quality data because it is produced under pharmaceutical-grade conditions.
For NMN, look for products verified by independent labs such as NSF International, USP, or Informed Sport. The specific brand matters less than the verification.
The Bottom Line
NAD+ IV, NMN, and NR are not competing strategies — they are complementary tools for different clinical contexts. IV delivery provides the most powerful acute restoration. Oral precursors provide sustainable daily maintenance. The choice between NMN and NR is less important than product quality and consistent dosing.
The evidence supports NAD+ repletion as a legitimate longevity strategy. It does not yet support any specific protocol as definitively optimal. What I recommend is based on the best available evidence combined with clinical observation from treating patients who take this seriously — and I will update these recommendations as the evidence evolves.
Here is what the evidence shows: NAD+ matters, restoring it helps, and the route of administration should match the clinical context.
References
- Camacho-Pereira J, et al. CD38 dictates age-related NAD decline and mitochondrial dysfunction through an SIRT3-dependent mechanism. Cell Metabolism. 2016;23(6):1127-1139. PMID: 27304511.
- Braidy N, et al. Role of nicotinamide adenine dinucleotide and related precursors as therapeutic targets for age-related degenerative diseases. Antioxidants & Redox Signaling. 2019;30(2):251-294. PMID: 29634344.
- Grozio A, et al. Slc12a8 is a nicotinamide mononucleotide transporter. Nature Metabolism. 2019;1(1):47-57. PMID: 31131364.
- Yi L, et al. The efficacy and safety of beta-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience. 2023;45(1):29-43. PMID: 36482258.
- Liao B, et al. Nicotinamide mononucleotide supplementation enhances aerobic capacity in amateur runners: a randomized, double-blind study. Journal of the International Society of Sports Nutrition. 2021;18(1):54. PMID: 34238308.
- Igarashi M, et al. Chronic nicotinamide mononucleotide supplementation elevates blood nicotinamide adenine dinucleotide levels and alters muscle function in healthy older men. NPJ Aging. 2022;8(1):5. PMID: 36151108.
- Kim M, et al. Effect of 12-week intake of nicotinamide mononucleotide on sleep quality, fatigue, and physical performance in older Japanese adults. Nutrients. 2022;14(4):755. PMID: 35215405.
- Sinclair DA, et al. Declining NAD+ induces a pseudohypoxic state disrupting nuclear-mitochondrial communication during aging. Cell. 2013;155(7):1624-1638. PMID: 24360282.
- Martens CR, et al. Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications. 2018;9(1):1286. PMID: 29599478.
- Elhassan YS, et al. Nicotinamide riboside augments the aged human skeletal muscle NAD+ metabolome and induces transcriptomic and anti-inflammatory signatures. Cell Reports. 2019;28(7):1717-1728. PMID: 31412242.
- Dollerup OL, et al. A randomized placebo-controlled clinical trial of nicotinamide riboside in obese men: safety, insulin-sensitivity, and lipid-mobilizing effects. American Journal of Clinical Nutrition. 2018;108(2):343-353. PMID: 29992272.
- Remie CME, et al. Nicotinamide riboside supplementation alters body composition and skeletal muscle acetylcarnitine concentrations in healthy obese humans. American Journal of Clinical Nutrition. 2020;112(2):413-426. PMID: 32320006.