Methylene blue is one of the oldest synthetic drugs in medicine — first synthesized in 1876 and used to treat malaria before the development of modern antimalarials. It remains an FDA-approved treatment for methemoglobinemia and is on the WHO’s List of Essential Medicines.
Its recent resurgence of interest in the longevity and biohacking communities stems from its unusual property as an alternative electron carrier in the mitochondrial electron transport chain. This mechanism, along with its antimicrobial and potential neuroprotective properties, has generated considerable discussion.
I want to be upfront: methylene blue is one of the interventions where I use particularly conservative language, because the gap between its mechanistic promise and its clinical validation for longevity applications is significant.
Mechanism of Action
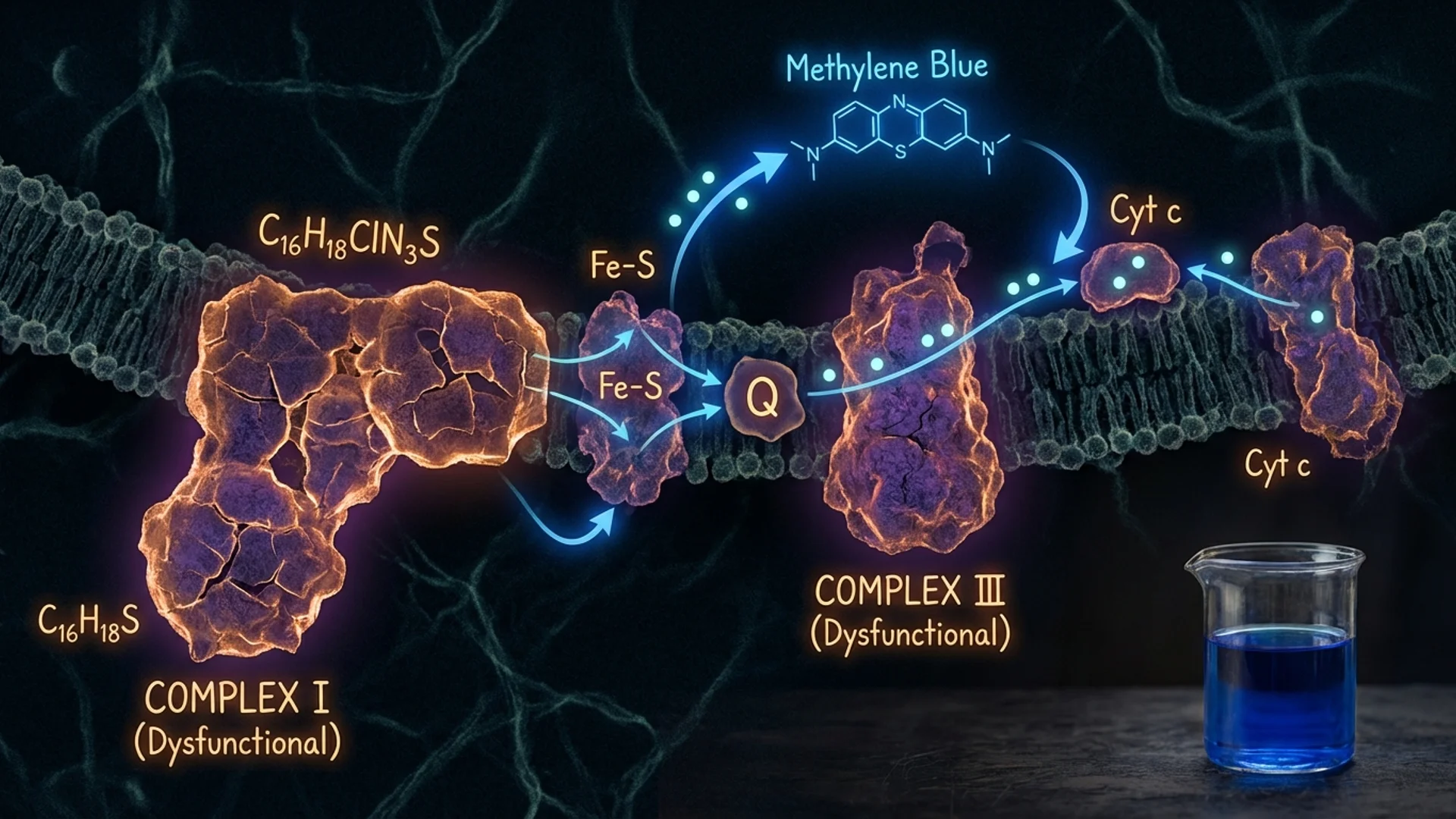
Methylene blue has a unique pharmacological property. It can accept and donate electrons at low doses, effectively functioning as an auxiliary component of the mitochondrial electron transport chain. Specifically, it can shuttle electrons from NADH to cytochrome c, bypassing Complex I and Complex III — the two sites most commonly impaired in mitochondrial dysfunction and most associated with age-related decline [1].
At low concentrations (0.5-4 mg/kg in animal studies, much lower in typical human supplementation), this electron shuttling:
- Increases ATP production in cells with compromised mitochondria
- Reduces reactive oxygen species (ROS) by providing an alternative pathway that avoids the ROS-generating steps
- Supports NAD+/NADH cycling
- May protect against oxidative stress at the mitochondrial level
At high concentrations, the effect reverses — methylene blue becomes a pro-oxidant. This hormetic dose-response is important and underscores the necessity of appropriate dosing.
What the Preclinical Data Shows
In animal models, low-dose methylene blue has demonstrated:
- Neuroprotection: Reduced tau aggregation and improved cognitive performance in Alzheimer’s disease mouse models. Improved outcomes in traumatic brain injury models.
- Lifespan extension: Extended lifespan in nematodes (C. elegans) and fruit flies. Mammalian lifespan data is limited.
- Antimicrobial activity: Effective against various pathogens including Plasmodium (malaria), methicillin-resistant Staphylococcus aureus (MRSA), and certain fungal species. This is well-established — methylene blue’s antimicrobial history predates its longevity interest.
- Mitochondrial support: Improved mitochondrial function in aged animal tissues.
These are preclinical findings. The consistent caveat applies: effects in nematodes, flies, and mice do not guarantee human efficacy.
Human Evidence
Established uses: Methylene blue is validated for methemoglobinemia, as an intraoperative dye, and has historical use as an antimalarial. These are not longevity applications, but they provide extensive human safety data.
Cognitive applications: A derivative, LMTM (leuco-methylthioninium bis(hydromethanesulphonate)), was tested in Phase III trials for Alzheimer’s disease. The results were disappointing — the drug did not meet its primary endpoints as an add-on therapy, though post-hoc analyses suggested possible benefit as monotherapy in a subset [2]. These results tempered enthusiasm for methylene blue as a cognitive enhancer.
Antimicrobial use: Methylene blue combined with photodynamic therapy (light activation) has demonstrated efficacy against oral pathogens and is used in some dental and wound care applications.
Longevity-specific human data: Does not exist in any meaningful form. No controlled human trial has evaluated methylene blue for longevity endpoints.
How I Approach Methylene Blue
In my practice, I consider methylene blue in specific clinical contexts:
- As a supportive mitochondrial agent in patients with documented mitochondrial dysfunction, typically as part of a broader mitochondrial support protocol
- For its antimicrobial properties in the context of chronic infection treatment programs
- Never as a standalone longevity intervention
Dosing in supplemental use is typically 0.5-2 mg/kg orally, which is substantially lower than therapeutic doses for methemoglobinemia. Even at these doses, patients should be aware of:
- Blue discoloration of urine and potentially stool. This is expected and harmless but startling if not anticipated.
- Serotonin syndrome risk. Methylene blue is a potent monoamine oxidase inhibitor (MAOI). It should not be combined with SSRIs, SNRIs, or other serotonergic medications. This is not a theoretical risk — cases of serotonin syndrome have been reported.
- G6PD deficiency. Methylene blue is contraindicated in patients with glucose-6-phosphate dehydrogenase deficiency, as it can cause hemolytic anemia.
- Photosensitivity. Methylene blue can increase skin sensitivity to light.
The Honest Assessment
Methylene blue has a fascinating pharmacology, a long history of medical use, and a plausible mechanistic rationale for mitochondrial support. The preclinical longevity data is interesting. The human longevity data is essentially absent.
This is an investigational agent for longevity purposes. It deserves continued research. But presenting it as a validated longevity intervention — as some corners of the supplement industry do — outpaces the evidence.
For patients who use it, pharmaceutical-grade sourcing is essential. Industrial methylene blue contains impurities (heavy metals and other contaminants) that make it unsuitable for human consumption.

References
- Atamna H, et al. Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB Journal. 2008;22(3):703-712.
- Gauthier S, et al. Efficacy and safety of tau-aggregation inhibitor therapy in patients with mild or moderate Alzheimer’s disease: a randomised, controlled, double-blind, parallel-arm, phase 3 trial. Lancet. 2016;388(10062):2873-2884.
This content is educational and does not constitute medical advice. Methylene blue has significant drug interactions (particularly with serotonergic medications) and contraindications. Its use should be supervised by a qualified physician. It is investigational for longevity purposes.