At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate |
| Primary Use | Patient education and treatment expectation management |
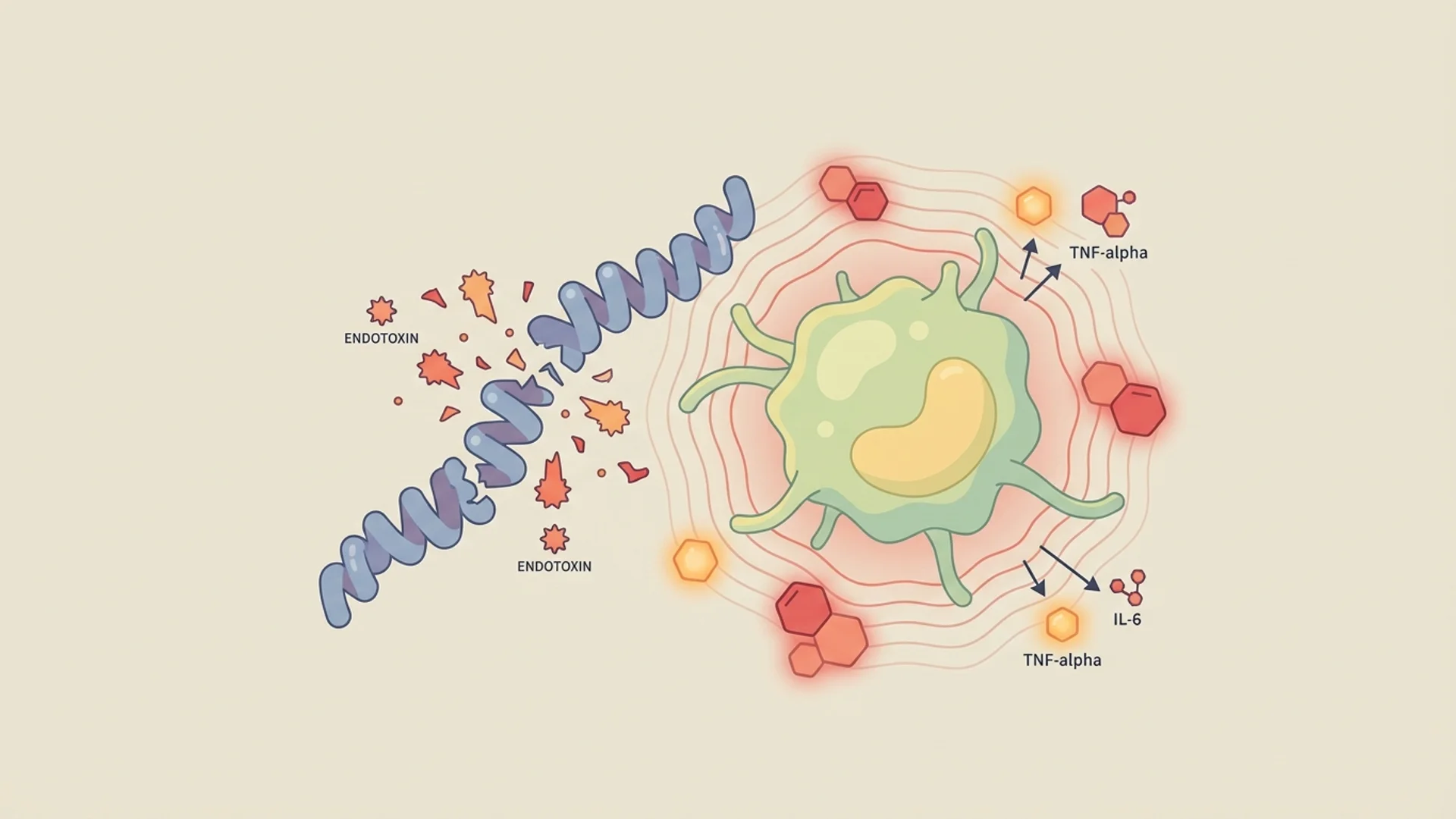
| Key Mechanism | Cytokine cascade from endotoxin release during pathogen death; reflects antimicrobial biological activity |
The Question Behind the Question
When a patient asks “is Herxing a good sign?” they are really asking something deeper: “Is my treatment working, and does the suffering have a purpose?”
Let me give you the direct answer, and then explain the nuance.
Yes — a Herxheimer reaction is a sign that your antimicrobial therapy has biological activity against the targeted organisms. Pathogens are being killed, releasing endotoxins and inflammatory mediators, and your immune system is responding to that release. This is evidence of treatment effect.
But — and this is where the common understanding goes wrong — the severity of the Herxheimer reaction does not correlate with the effectiveness of treatment. A severe Herx is not better than a mild one. More suffering does not equal more healing. And the belief that it does — a belief pervasive in Lyme disease communities — can cause real harm.
Here is what the evidence actually shows.
What the Herxheimer Reaction Tells You
It Confirms Antimicrobial Activity
A Herxheimer reaction tells you that:
- The antimicrobial is reaching the target organisms (bioavailability is adequate)
- The organisms are susceptible to the agent (they are being killed)
- The immune system is recognizing and responding to the released microbial components (immune function is at least partially intact)
This is useful information. If you start a new antibiotic and experience no change whatsoever — no improvement and no Herx — it raises questions about whether the drug is reaching the organisms, whether the organisms are susceptible, or whether the diagnosis is correct.
In our clinical experience, a mild to moderate Herxheimer reaction within the first 1-2 weeks of treatment is the most common pattern in patients with confirmed tick-borne infections. Its absence does not definitively mean treatment is failing (some patients have mild infections, efficient detoxification, or simply tolerate die-off well), but its presence is reassuring.
It Does NOT Tell You These Things
It does not measure treatment completeness. A Herx reaction does not tell you how much of the infection has been cleared. It tells you that some organisms are dying. Patients can Herx repeatedly throughout a treatment course as new populations are exposed — through biofilm disruption, through reaching new tissue compartments, or through targeting different morphological forms.
It does not correlate with total pathogen burden. A patient with a severe Herx may have a smaller total infection than a patient with a mild Herx. The reaction intensity depends on multiple factors beyond pathogen load, including:
- Individual cytokine response (genetic variation in TNF-alpha, IL-6 production)
- Detoxification capacity (liver function, glutathione reserves, methylation status)
- Concurrent inflammatory burden (mold/CIRS, autoimmunity, other infections)
- Autonomic nervous system state (sympathetic dominance amplifies inflammatory perception)
It does not mean the worse you feel, the sicker you were. This is the most dangerous misconception. I see patients in online forums encouraging each other to “push through” severe Herx reactions on the theory that more die-off means more healing. This is physiologically wrong and clinically harmful.
Why Maximizing Herx Is a Mistake
The Inflammatory Cascade Has Consequences
TNF-alpha, IL-6, and IL-1beta — the primary cytokines driving Herxheimer reactions — are not benign molecules [1]. At moderate levels, they facilitate pathogen clearance and immune activation. At excessive levels, they cause:
- Neuroinflammation: Worsening brain fog, cognitive dysfunction, and potential neurotoxicity
- Mitochondrial damage: Excessive TNF-alpha impairs mitochondrial electron transport chain function, depleting cellular energy — making fatigue worse, not just symptomatically but at the cellular level
- Endothelial damage: High cytokine levels damage blood vessel walls, impairing microcirculation
- Adrenal stress: Sustained inflammatory surges tax the HPA axis, worsening the cortisol dysregulation already common in chronic illness
- Autoimmune activation: Intense inflammatory episodes can trigger molecular mimicry and autoimmune cross-reactivity in genetically susceptible individuals
The Detoxification System Has Capacity Limits
Your liver processes endotoxins through Phase I (oxidation via cytochrome P450 enzymes) and Phase II (conjugation with glutathione, glucuronic acid, sulfate, etc.) pathways. Both phases have finite capacity. When endotoxin release exceeds detoxification capacity, the excess circulates systemically, prolonging and intensifying the inflammatory response.
This is not a theoretical concern. In our clinical experience, patients who push through severe Herx reactions without adequate management support — hydration, binders, anti-inflammatory agents, dose pacing — often deteriorate rather than improve. Some develop what appears to be post-inflammatory sensitization: a state where the nervous system becomes hyperresponsive to stimuli, making recovery more difficult even after the infection is controlled.
Controlled Burn vs. Wildfire
What I tell my patients: think of pathogen clearance like a controlled burn in forestry. The goal is to remove the dead wood (the pathogens) in a way that the ecosystem (your body) can manage. A controlled burn clears the land and promotes new growth. A wildfire destroys everything.
The same antimicrobial at the same dose can produce a controlled burn (with proper support) or a wildfire (without support) depending on how the die-off is managed.

The Evidence
What We Know (Human Data)
The Jarisch-Herxheimer reaction was originally characterized in syphilis treatment, where it occurs in 70-90% of patients receiving their first dose of penicillin for secondary syphilis. In this context, the reaction is typically self-limiting (24-48 hours), well-tolerated, and indeed a sign of effective treatment [2].
In Lyme disease, the picture is more complex. The Herxheimer reaction occurs less predictably, varies more in duration and intensity, and occurs against a background of chronic illness that makes it harder to distinguish from baseline symptoms. Published data from treatment studies report Herx-like reactions in 20-50% of treated Lyme patients, though the true incidence is likely higher in patients with chronic/disseminated disease [1].
Critically, no study has demonstrated a correlation between Herxheimer reaction severity and treatment outcome. This absence of correlation is significant: if worse Herx meant better outcomes, we would see it in the data. We do not.
What We See in the Lab (Preclinical)
Animal models of spirochetal infection show that the Herxheimer reaction is driven by the innate immune response to lipoproteins released from killed organisms — primarily through Toll-like receptor 2 (TLR2) activation [3]. The intensity of the response depends on:
- The rate of organism killing (dose-dependent)
- The quantity of lipoproteins released per organism (species-dependent)
- The host inflammatory response capacity (genetically variable)
Importantly, in animal models where the inflammatory response is partially attenuated (through anti-TNF or anti-inflammatory agents), antimicrobial efficacy is not reduced. The organisms are killed just as effectively whether the inflammatory response is severe or modulated. This supports the clinical principle that managing the Herx does not compromise treatment.
What I See in Practice
In our clinical experience, the patients with the best long-term outcomes are not those who had the most severe Herxheimer reactions. They are the patients who maintained consistent, sustainable treatment over an adequate duration — with managed die-off reactions that allowed them to stay on therapy.
The patients who do worst are those who:
- Push through severe Herx without management (causing inflammatory damage and treatment dropout)
- Stop treatment at the first sign of Herx (mistaking treatment effect for harm)
Both extremes are problematic. The optimal path is the middle: recognize the Herx as a sign of treatment activity, manage it proactively, and communicate with your physician about pacing.
Practical Application
How to Interpret Your Herx Reaction
Mild Herx (tolerable — you can function):
- Treatment is active
- Your detoxification capacity is handling the load
- Continue treatment and monitoring
- Implement basic support (hydration, anti-inflammatory)
Moderate Herx (uncomfortable — reduced function for 3-7 days):
- Treatment is active with significant pathogen kill
- Implement full Herx management protocol
- Contact physician if lasting more than 10 days
- Consider dose adjustment at next visit
Severe Herx (debilitating — unable to function for more than 3 days):
- Treatment is active but die-off rate exceeds detoxification capacity
- Reduce antimicrobial dose (with physician guidance)
- Implement aggressive binder and anti-inflammatory support
- Evaluate detoxification pathway function (liver, kidney)
- Consider underlying factors: mold/CIRS, methylation issues, concurrent inflammation
No Herx:
- Does not necessarily mean treatment failure
- Possible explanations: low pathogen burden, efficient detoxification, adequate immune clearance
- Reassess after 4-6 weeks if no clinical improvement
- Consider testing to verify diagnosis if no Herx AND no clinical improvement
The Myth of “Not Herxing Enough”
I encounter this regularly in my practice: patients who feel they are not Herxing enough and therefore their treatment is not working. Some even request higher doses or additional agents to provoke a Herx.
Let me be direct: if you are improving clinically — less fatigue, better cognition, reduced pain — without a discernible Herx reaction, that is the best possible scenario. It means the organisms are being cleared at a rate your body can manage without inflammatory overload. Do not seek suffering to validate your treatment.

Safety and Considerations
- Severe Herxheimer reactions can mimic sepsis. High fever, hypotension, and tachycardia require medical evaluation regardless of suspected cause.
- The absence of Herx does not rule out effective treatment. Some patients have efficient detoxification and robust immune clearance without significant inflammatory symptoms.
- Some conditions that mimic Herx (adverse drug reactions, allergic reactions, concurrent infections) require different management. Distinguishing Herx from disease flare is essential.
- Patients on immunosuppressive therapy may have attenuated Herx reactions despite active pathogen kill.
- Online communities often reinforce the “worse is better” narrative. This is well-intentioned but not medically accurate. Follow your physician’s guidance, not forum advice.
The Bottom Line
A Herxheimer reaction is a sign that your antimicrobial therapy has biological activity — yes, it indicates treatment effect. But the common belief that more severe Herx equals better treatment is a physiological error. Excessive die-off overwhelms detoxification capacity, causes collateral inflammatory damage, and can worsen rather than improve your trajectory. The goal is controlled, sustainable pathogen clearance with active management of die-off symptoms. In my clinical experience, the patients who do best are those who pace their treatment, support their detoxification pathways, and communicate openly with their physician about what they are experiencing.
References
- Butler T. The Jarisch-Herxheimer reaction after antibiotic treatment of spirochetal infections: a review of recent cases and our understanding of pathogenesis. Am J Trop Med Hyg. 2017;96(1):46-52. PMID: 28077740
- Young EJ, Weingarten NM, Baughn RE, Duncan WC. Studies on the pathogenesis of the Jarisch-Herxheimer reaction: development of an animal model and evidence against a role for classical endotoxin. J Infect Dis. 1982;146(5):606-615. PMID: 6815281
- Pound MW, May DB. Proposed mechanisms and preventative options of Jarisch-Herxheimer reactions. J Clin Pharm Ther. 2005;30(3):291-295. PMID: 15896244
- Belum GR, Belum VR, Chaitanya Arudra SK, Reddy BS. The Jarisch-Herxheimer reaction: revisited. Travel Med Infect Dis. 2013;11(4):231-237. PMID: 23632012