At a Glance
| Property | Value |
|---|---|
| Session Duration | 2-3 hours |
| Sessions Typically Required | 2-5 depending on indication |
| Session Spacing | Every 2-3 days |
| Setting | Outpatient apheresis suite (no overnight stay required) |
| Pain Level | Minimal (two needle insertions, similar to a standard blood draw) |
| Immediate Side Effects | Mild fatigue, occasional light-headedness, transient coolness |
| Return to Normal Activity | Most patients resume light activity same day |
This Is Simpler Than You Think
Many patients arrive for their first apheresis session imagining something dramatic — machines, tubes, alarms. The reality is remarkably calm. You sit in a comfortable recliner. You have a needle in each arm. Blood flows out one side, through a machine that quietly does its work, and back in the other side. Most patients read, answer emails, watch something on their phone, or simply doze off.
If the idea of blood filtration makes you uneasy, I want to reassure you: this is one of the most straightforward medical procedures we perform. The technology has been in clinical use for decades, and our team at Klinik St. Georg has performed thousands of apheresis sessions across seven different modalities. You are in experienced hands.
Before Your First Session
Pre-Apheresis Assessment
Before we begin any apheresis treatment, we conduct a thorough assessment. This is usually completed as part of your overall intake at the hospital, but if you are coming specifically for apheresis, here is what we evaluate:
- Baseline laboratory panel: Complete blood count, coagulation studies (PT, aPTT, fibrinogen), lipid panel, CRP, liver and kidney function, and electrolytes. These values help us determine the optimal apheresis protocol and number of sessions.
- Vascular access assessment: We examine the veins in both arms. H.E.L.P. apheresis requires two venous access points — one for blood withdrawal and one for return. Most patients have adequate peripheral veins. In rare cases where venous access is challenging, we may need to use a central venous catheter, but this is uncommon.
- Medication review: Certain medications — particularly anticoagulants — require adjustment before apheresis. Blood thinners can interfere with the heparin used in the procedure. ACE inhibitors may need to be paused on the day of treatment, as they can interact with the precipitation process and cause a drop in blood pressure.
- Hydration optimization: We ask patients to drink plenty of fluids in the 24 hours before their session and to eat a normal breakfast on the morning of treatment. Arriving dehydrated makes venous access more difficult and increases the likelihood of feeling light-headed during the procedure.
What to Bring
- Comfortable clothing with sleeves that can be easily rolled above the elbow
- Something to keep you occupied for 2-3 hours (book, tablet, headphones)
- A light snack and water for immediately after the session
- A companion for your first session, if possible — not required, but some patients appreciate having someone there the first time
The Day of Treatment: Step by Step
Arrival and Setup (15-20 minutes)
You arrive at the apheresis suite, which is a quiet, climate-controlled room with reclining chairs, each with its own apheresis machine. Our specialized apheresis nurses will greet you and get you settled.
What happens:
- Vital signs check (blood pressure, heart rate, temperature)
- Brief discussion of how you are feeling and any concerns
- Positioning in the recliner — you can adjust the angle for maximum comfort
- Venous access: two peripheral IV needles are placed, one in each arm. The insertion feels like a standard blood draw. Once the needles are in place, they are taped securely and should not cause discomfort during the procedure
A note about the needles: The gauge used for apheresis is slightly larger than a standard blood draw needle, because blood needs to flow at a sufficient rate. Some patients notice this difference. If you are anxious about needles, tell our nursing staff — they are experienced at making this as comfortable as possible, and we can apply topical numbing cream in advance if you request it.
The Filtration Process (2-2.5 hours)
Once access is established, the machine begins. Here is what is happening inside the circuit, explained in terms you can actually observe:
What you see: Blood flows out of one arm through a transparent tube into the machine. The machine hums quietly. Occasionally you hear a soft pump sound. Blood returns through a tube in your other arm. That is essentially it from your perspective.
What is happening inside the machine:
-
Blood separation. Your whole blood enters a centrifuge that separates it into two fractions: plasma (the liquid part containing proteins, fats, and inflammatory mediators) and blood cells (red cells, white cells, platelets). Your blood cells are never exposed to the filtration chemistry — they are held in the circuit and returned to you continuously.
-
Heparin precipitation. Your plasma is mixed with heparin and an acetate buffer at a precisely controlled pH of 5.12. At this acidity, the target molecules — LDL cholesterol, Lp(a), fibrinogen, CRP, and other inflammatory proteins — become insoluble and clump together into visible precipitates.
-
Filtration. The precipitate-laden plasma passes through a polycarbonate filter. The clumped pathological molecules are trapped. Clean plasma passes through.
-
pH correction and heparin removal. The filtered plasma is dialyzed against a bicarbonate buffer to restore normal pH (7.4) and remove the excess heparin.
-
Reconstitution and return. The cleaned plasma is recombined with your blood cells and returned to your other arm.
This entire cycle runs continuously. Your blood is being drawn, processed, and returned simultaneously — at any given moment, only a small volume of your blood is outside your body.
What You Will Feel During Treatment
Most patients feel very little. The procedure is not painful once the needles are in place. Here is what you might notice:
- Mild coolness: The returned blood is slightly below body temperature. Some patients notice a cool sensation in the return arm or feel generally slightly cool. We keep blankets available.
- Tingling around the lips or fingertips: This can occasionally occur due to transient calcium shifts from the citrate anticoagulant used in the circuit. It is harmless and typically resolves on its own. If it persists, we administer IV calcium, which resolves it within minutes.
- A need to use the bathroom: The procedure takes 2-3 hours, and you have been drinking fluids. We can pause the machine briefly for bathroom breaks without any issue.
- Mild drop in blood pressure: Some patients experience a slight decrease in blood pressure, which can cause light-headedness. This is managed by slowing the flow rate and administering IV fluids. It is more common in patients who are dehydrated or have naturally low blood pressure.
What you will not feel: Pain in the arms (beyond the initial needle insertion), nausea, or any sensation from the blood being processed. The machine does all the work silently while you relax.
Completion and Needle Removal (10-15 minutes)
When the target volume of plasma has been processed, the machine completes its cycle and returns any remaining blood in the circuit to your body. The needles are removed and pressure is applied to the puncture sites for several minutes. Bandages are applied.
You remain in the recliner for 10-15 minutes while we check your blood pressure and ensure you feel well.
After the Session: The First 48 Hours
Immediately After (First 2-4 hours)
Most patients feel fine immediately after apheresis. Some feel light-headed when they first stand up — this is positional and resolves quickly. We recommend:
- Drink a glass of water and have your snack before leaving the apheresis suite
- Take it easy for the rest of the day — no intense exercise or heavy lifting
- Stay well hydrated for the remainder of the day (at least 2-3 liters of fluids)
The Evening After Treatment
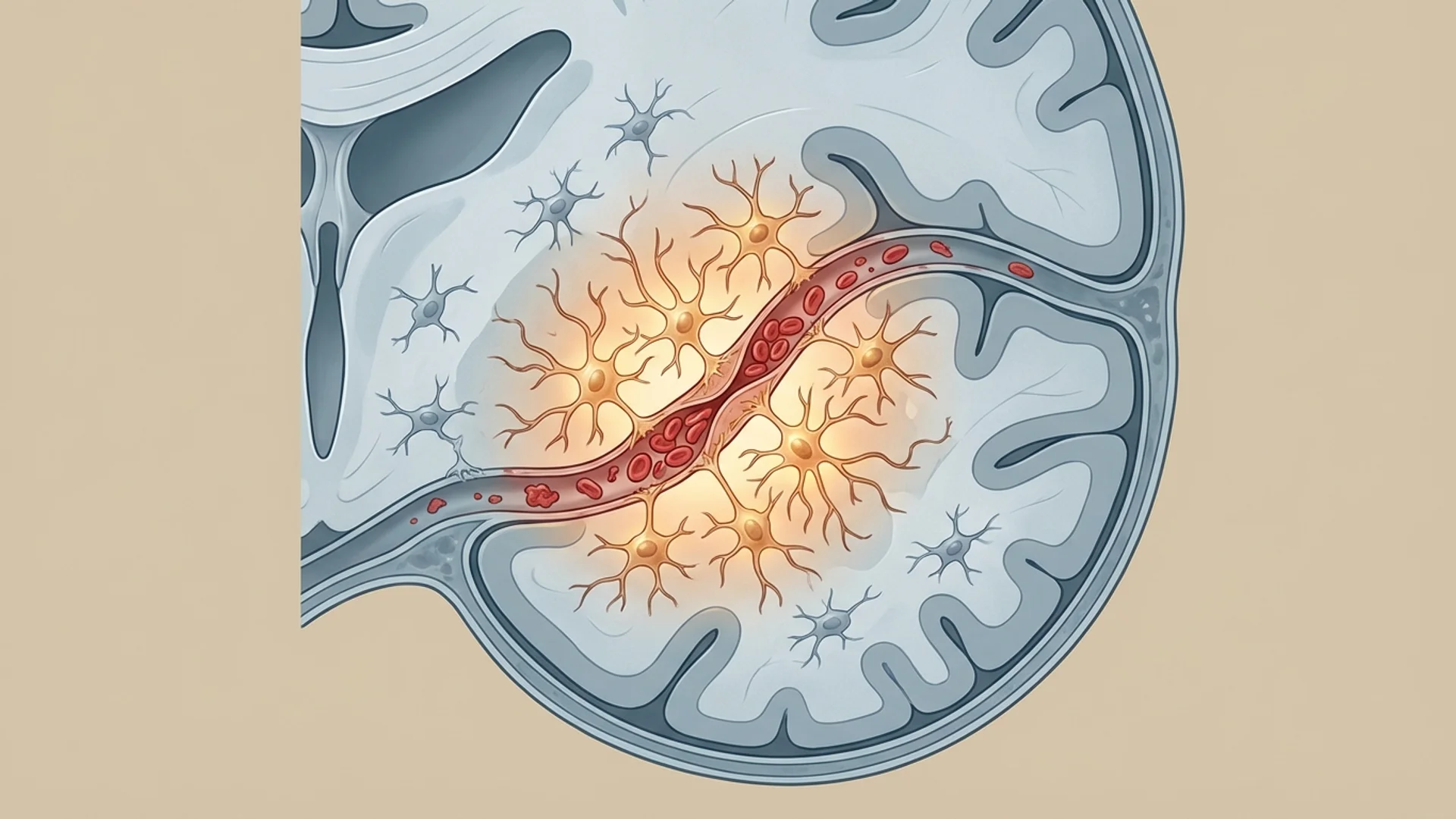
Many patients report an interesting phenomenon: they feel noticeably clearer or lighter on the evening after their first session. This is not placebo — we have just physically removed a significant quantity of inflammatory mediators, fibrinogen, and pathological lipoproteins from your bloodstream. The effect is tangible and immediate for many patients, particularly those with high baseline inflammatory burden.
Some patients, conversely, feel more tired than usual on the evening of treatment. Both responses are normal.
The Following Day
- Mild fatigue is the most common residual effect and typically resolves within 24-48 hours
- The needle sites may be mildly sore or bruised — this is normal
- Appetite is usually unaffected
- You can resume normal daily activities, including light exercise
- We recommend avoiding alcohol for 24 hours after treatment
Between Sessions
If you are receiving a series of sessions (which most patients do), they are typically spaced every 2-3 days. This interval allows your body to equilibrate between treatments while maintaining therapeutic momentum. During the days between sessions, you continue your normal routine. No special restrictions apply beyond staying well hydrated.
How Many Sessions Will You Need?
The number of sessions depends on your indication and your response:
| Indication | Typical Sessions | Rationale |
|---|---|---|
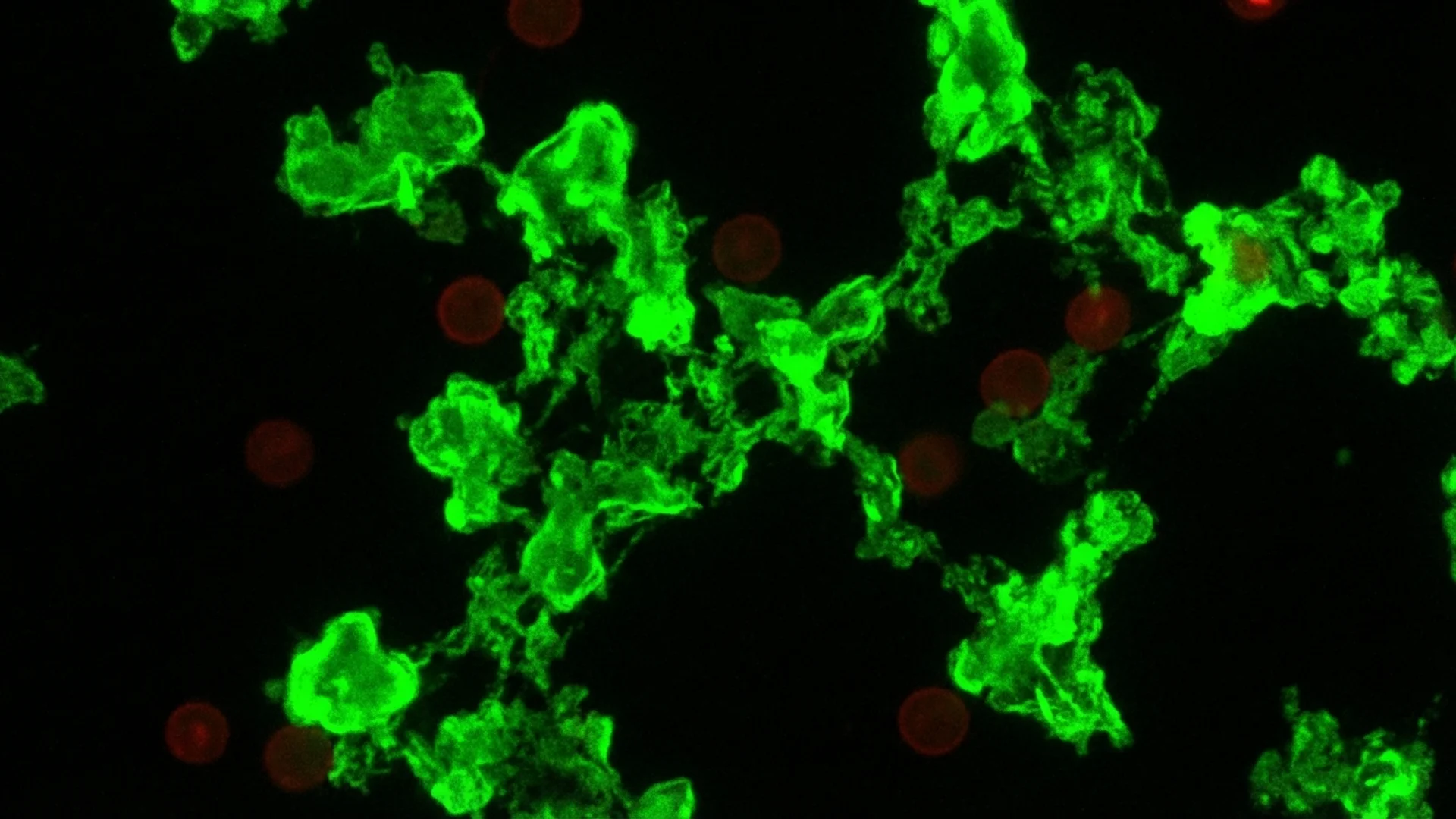
| Post-COVID / Long COVID | 3-5 | Clearing microclots, spike protein, and inflammatory mediators |
| Chronic Lyme disease (adjunctive) | 2-4 | Removing endotoxins, immune complexes, and inflammatory load |
| Hyperlipidemia / elevated Lp(a) | 2-3 initially, then periodic | Direct removal of pathological lipoproteins |
| Chronic inflammatory conditions | 3-5 | Reducing systemic inflammatory mediator burden |
We assess your response after each session with targeted laboratory testing. CRP, fibrinogen, and lipid panels are checked to track objective improvement. This data guides the decision about whether additional sessions are needed.
The Seven Apheresis Modalities at St. Georg
H.E.L.P. apheresis is our most commonly used modality, but it is not the only one. Klinik St. Georg offers seven distinct apheresis techniques, and the choice of modality depends on what we need to remove from your blood:
- H.E.L.P. apheresis — LDL, Lp(a), fibrinogen, CRP, inflammatory proteins
- Therapeutic Plasma Exchange (TPE) — complete plasma replacement for severe autoimmune conditions
- Double Cascade Filtration — selective plasma filtration by molecular weight
- Evaflux a3/a5 — targeted removal of specific immunoglobulins and inflammatory mediators
- INUSpheresis — broad-spectrum environmental toxin removal
- Immunoadsorption — selective removal of pathogenic antibodies
- Leukapheresis — white blood cell removal for specific hematological conditions
Your treating physician will determine which modality — or combination of modalities — is appropriate for your situation. Some patients receive more than one type of apheresis during their treatment course.
Common Concerns Addressed
“Will I feel weak from losing blood?” You are not losing blood. Your blood cells are returned to you continuously throughout the procedure. The volume removed consists of pathological molecules — LDL, fibrinogen, CRP — that your body will partially regenerate over the following days. The net effect on blood volume is minimal, which is why most patients feel fine afterward.
“Is the heparin dangerous?” The heparin used in the circuit is removed by dialysis before your plasma is returned to you. You are not systemically anticoagulated. However, we do monitor coagulation parameters, and patients who are already on blood thinners require dose adjustment.
“Will my immune system be weakened?” Unlike total plasma exchange, H.E.L.P. apheresis is selective. Your albumin, immunoglobulins (antibodies), and other protective proteins are returned to you. The molecules removed are pathological or inflammatory — removing them strengthens your body’s ability to recover, rather than weakening it.
“Can I drive myself home?” After your first session, we recommend having someone available to drive you, as we do not know how you will respond. After subsequent sessions, most patients are comfortable driving themselves if they feel well.
Clinical Perspective — Julian Douwes M.D. Apheresis is one of the most satisfying treatments I offer because the results are often visible in the laboratory within hours. When a patient arrives with a CRP of 15 and a fibrinogen of 500, and we measure those values after a single H.E.L.P. session and see a CRP of 3 and fibrinogen of 180, there is no ambiguity about what just happened. We physically removed the molecules driving their inflammation. For patients with Long COVID who have been told their labs are “normal” despite feeling terrible, this kind of objective, measurable change is profoundly validating. The machine does not lie, and neither do the lab results.
Key Takeaways
- H.E.L.P. apheresis is a 2-3 hour outpatient procedure that is not painful beyond the initial needle insertion
- You remain awake and comfortable throughout the entire session — no sedation is required
- The procedure selectively removes LDL, fibrinogen, CRP, and inflammatory mediators while preserving your protective blood components
- Most patients notice improvement — sometimes dramatic improvement — within hours to days of their first session
- Mild fatigue and light-headedness are the most common side effects, resolving within 24-48 hours
- A typical treatment course involves 2-5 sessions spaced every 2-3 days
- Klinik St. Georg offers seven distinct apheresis modalities, selected based on your specific condition and needs
References
- Bosch T, Schmidt B, Blumenstein M, Gurland HJ. Lipid apheresis by hemoperfusion: in vitro efficacy and ex vivo biocompatibility of a new low-density lipoprotein adsorber compatible with human whole blood. Artif Organs. 1993;17(7):640-652. PMID: 8215879.
- Jaeger BR, Richter Y, Nagel D, et al. Longitudinal cohort study on the effectiveness of lipid apheresis treatment to reduce high lipoprotein(a) levels and prevent major adverse coronary events. Nat Clin Pract Cardiovasc Med. 2009;6(3):229-239. PMID: 19234501.
- Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172. PMID: 34425843.