If you are researching therapeutic apheresis — particularly for post-COVID recovery, microclot reduction, or chronic inflammatory conditions — you have likely encountered two names: H.E.L.P. Apheresis and INUSpheresis. Both are blood filtration therapies available at German clinics and increasingly discussed in integrative medicine circles. Both are presented as treatments for similar conditions. And the confusion between them is understandable, because neither system’s marketing clearly explains how they differ.
Here is what the evidence shows, how each system actually works at a technical level, and how I think about recommending one versus the other.
At a Glance
| Feature | H.E.L.P. Apheresis | INUSpheresis |
|---|---|---|
| Full name | Heparin-induced Extracorporeal LDL Precipitation | INUSpheresis (INUS Medical) |
| Mechanism | Heparin-mediated precipitation of lipoproteins, fibrinogen, and CRP | Adsorption-based filtration using proprietary binding filters |
| Primary targets | LDL-C, Lp(a), fibrinogen, CRP, inflammatory mediators | Environmental toxins, inflammatory cytokines, spike protein, heavy metals |
| Regulatory status | CE-marked, well-established (30+ years) | CE-marked, newer system |
| Published studies | Extensive (cardiovascular, lipid disorders) | Limited (case series, post-COVID observational data) |
| Sessions typically needed | 5-10 (condition-dependent) | 3-6 (condition-dependent) |
| Session duration | 1.5-2.5 hours | 2-3 hours |
| Cost per session | EUR 1,500-3,000 | EUR 2,000-3,500 |
| Availability | Germany, Austria, select EU centers | Primarily Germany |
How H.E.L.P. Apheresis Works
H.E.L.P. Apheresis (Heparin-induced Extracorporeal LDL Precipitation) was developed in the 1980s by B. Braun Melsungen AG for the treatment of severe familial hypercholesterolemia. It has since found broader applications in cardiovascular disease, microcirculatory disorders, and more recently, post-COVID syndrome.
The technical process:
- Blood withdrawal: Blood is drawn from a peripheral vein and separated into plasma and cellular components using a standard plasma separator.
- Heparin addition: The plasma fraction is mixed with heparin at a specific concentration and acidic pH (approximately pH 5.12). At this pH, heparin forms insoluble complexes with LDL cholesterol, Lp(a), fibrinogen, and C-reactive protein (CRP). These precipitate out of solution.
- Filtration: The precipitate is removed by passage through a polycarbonate filter, trapping the heparin-lipoprotein-fibrinogen complexes.
- Bicarbonate dialysis: Excess heparin is removed from the filtered plasma through a dialysis step using bicarbonate buffer. This also restores physiological pH.
- Reconstitution: The cleaned plasma is recombined with the cellular components and returned to the patient.
What it removes (and by how much per session):
- LDL cholesterol: 55-70% reduction
- Lipoprotein(a): 55-70% reduction
- Fibrinogen: 55-65% reduction
- C-reactive protein: 50-60% reduction
- Various inflammatory mediators co-precipitated with the fibrinogen-lipoprotein complex
The cardiovascular evidence base:
H.E.L.P. Apheresis has the strongest evidence base of any apheresis system for cardiovascular indications. The landmark HELP-LDL-Apheresis Multicenter Study demonstrated significant reductions in cardiovascular events in patients with severe hypercholesterolemia refractory to drug therapy (Seidel et al., 1991). It has been used for over three decades in Germany for patients with familial hypercholesterolemia and elevated Lp(a) who do not achieve adequate control with statins.
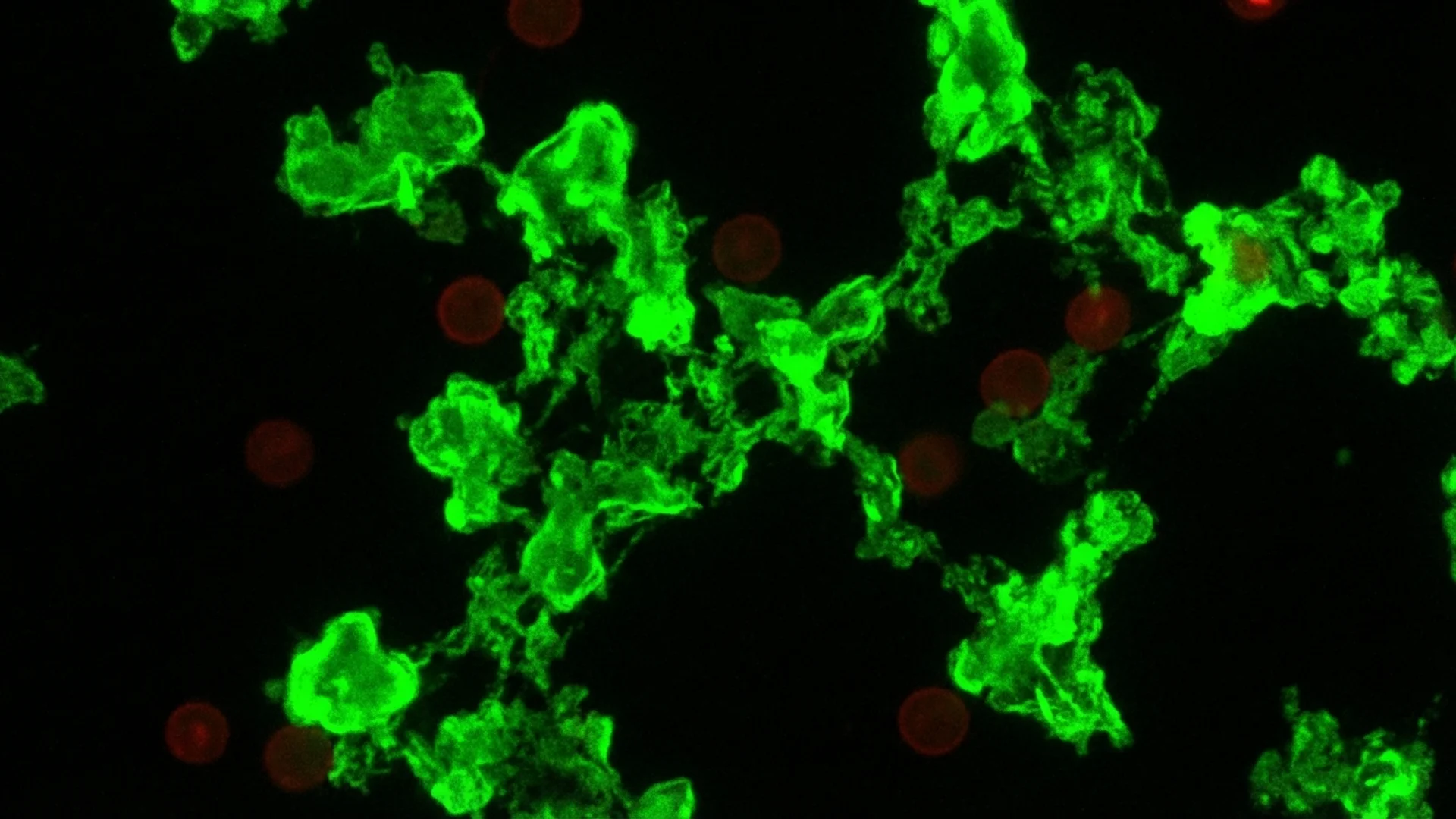
Why it is relevant for post-COVID: The connection to post-COVID syndrome came through the microclot hypothesis. Research by Etheresia Pretorius and colleagues demonstrated that patients with long COVID have persistent fibrin amyloid microclots in their circulation that trap inflammatory molecules and resist normal fibrinolysis. H.E.L.P. Apheresis dramatically reduces fibrinogen levels — the precursor to fibrin — and thereby reduces the substrate for microclot formation. Clinical observations at German apheresis centers reported symptomatic improvement in post-COVID patients following H.E.L.P. treatment, particularly in fatigue, cognitive function, and exercise tolerance.
How INUSpheresis Works
INUSpheresis was developed by INUS Medical GmbH as a therapeutic apheresis system with a broader filtration philosophy. Rather than targeting specific lipoproteins through chemical precipitation, INUSpheresis uses adsorption-based filters designed to capture a wider range of pathogenic substances.
The technical process:
- Blood withdrawal: Similar to H.E.L.P. — blood is drawn and separated into plasma and cellular components.
- Adsorption filtration: The plasma passes through a series of proprietary adsorption filters (the “INUS Filter” system). These filters contain binding media designed to attract and retain specific molecular classes through charge-based, hydrophobic, and affinity-based interactions.
- Multi-target filtration: Unlike H.E.L.P.’s specific heparin-precipitation mechanism, INUSpheresis claims to filter multiple substance categories simultaneously — environmental toxins, heavy metals, inflammatory cytokines, autoantibodies, and what the manufacturer describes as “pathogenic proteins” including SARS-CoV-2 spike protein.
- Plasma return: The filtered plasma is recombined with cellular components and returned to the patient.
What it claims to remove:
- Environmental toxins (pesticides, solvents, volatile organic compounds)
- Heavy metals (mercury, lead, cadmium — bound to plasma proteins)
- Inflammatory cytokines (TNF-alpha, IL-6, IL-1beta)
- Autoantibodies
- Histamine and other mast cell mediators
- Spike protein fragments (in the context of post-COVID or post-vaccination symptoms)
- Oxidized LDL and lipid peroxides
The evidence base:
This is where I must be direct: INUSpheresis has a substantially thinner evidence base compared to H.E.L.P. Apheresis. The published data consists primarily of case series and observational reports from INUS Medical-affiliated clinics. There are no published randomized controlled trials. The theoretical framework for broad-spectrum toxin removal is plausible, and the adsorption technology is scientifically sound, but the specific clinical claims exceed what the published evidence currently supports.
That said, the clinical observations from practitioners using INUSpheresis are not trivial. Patients with chronic environmental toxin exposure, mast cell activation syndrome, and post-COVID symptoms have reported meaningful improvement. Whether this reflects specific filtration effects or a combination of plasma exchange effects and clinical attention is difficult to determine without controlled trials.
Head-to-Head Comparison
| Parameter | H.E.L.P. Apheresis | INUSpheresis |
|---|---|---|
| Years of clinical use | 35+ | ~10 |
| Published RCTs | Multiple (cardiovascular) | None |
| Mechanism specificity | Highly specific (heparin-lipoprotein precipitation) | Broader (adsorption-based multi-target) |
| LDL reduction per session | 55-70% | Not primary target; modest |
| Fibrinogen reduction | 55-65% (strongest of any apheresis) | Moderate (less quantified) |
| Lp(a) reduction | 55-70% | Not primary target |
| Cytokine removal | Indirect (co-precipitated) | Claimed direct adsorption |
| Environmental toxin removal | Not designed for this | Primary claim |
| Spike protein removal | Not specifically demonstrated | Claimed by manufacturer |
| Regulatory evidence | CE-marked, guideline-supported for lipid disorders | CE-marked |
| Reproducibility of outcomes | High (well-standardized process) | Variable (less standardized data) |
| Side effects | Mild (transient hypotension, citrate effects) | Mild (transient fatigue, hypotension) |
| Insurance coverage (Germany) | Covered for approved lipid indications | Generally not covered |
When I Recommend H.E.L.P. Apheresis
H.E.L.P. Apheresis is my preference when:
- Cardiovascular risk reduction is a primary goal — patients with elevated Lp(a), familial hypercholesterolemia refractory to statins, or high cardiovascular risk profiles. This is where H.E.L.P. has its strongest evidence and longest track record.
- Post-COVID with suspected microclotting — the fibrinogen reduction mechanism directly addresses the microclot hypothesis. Patients presenting with post-COVID fatigue, exercise intolerance, and elevated D-dimer or fibrinogen levels are logical candidates.
- Quantifiable targets — H.E.L.P. produces measurable, reproducible reductions in LDL, Lp(a), fibrinogen, and CRP. Pre- and post-session labs clearly demonstrate what has been removed. This measurability is clinically valuable for monitoring treatment response.
- Evidence-based practice is a priority — for patients or referring physicians who want the most evidence-supported option, H.E.L.P.’s 35-year track record and multiple published studies make it the more defensible choice.
What I tell my patients: if fibrinogen and lipoproteins are the primary targets, H.E.L.P. is the proven tool. It does one thing extremely well, and the data supports that.
When I Recommend INUSpheresis
INUSpheresis may be the better fit when:
- Environmental toxin burden is a primary concern — patients with documented heavy metal exposure, mold-related illness (CIRS), or chronic environmental toxin accumulation. H.E.L.P. was not designed for toxin removal; INUSpheresis claims this as a core function.
- Mast cell activation syndrome (MCAS) — patients with histamine-related symptoms may benefit from the claimed removal of histamine and mast cell mediators. This is a plausible mechanism, though controlled data is lacking.
- Broad inflammatory load — patients with multi-system inflammation not primarily driven by lipoproteins or fibrinogen. The adsorption-based approach may capture a wider range of inflammatory mediators.
- Post-vaccination inflammatory syndromes — some practitioners report using INUSpheresis for patients with inflammatory symptoms following vaccination. The claimed spike protein removal is the theoretical basis, though this remains controversial and unvalidated by controlled studies.
Here is what the evidence shows: the theoretical framework for INUSpheresis is reasonable. Adsorption-based filtration can remove a broader range of substances than precipitation-based systems. But “can remove” and “has been demonstrated to remove in controlled conditions” are different statements, and the published evidence has not yet bridged that gap convincingly.
Can You Combine Them?
Some German clinics offer both systems and use them sequentially. The rationale for combining:
H.E.L.P. first: Remove the fibrinogen and lipoproteins that H.E.L.P. handles with proven efficiency. This addresses microclots, cardiovascular risk, and the acute inflammatory protein load.
INUSpheresis second: Follow with a broader-spectrum adsorption pass to target any remaining environmental toxins, cytokines, or other substances that H.E.L.P. does not specifically capture.
In practice, this combination approach is expensive (both in cost and in time) and is reserved for patients with complex, multi-factorial presentations — such as post-COVID patients who also have environmental toxin burden, or chronic Lyme patients with co-existing mold illness.
I want to be transparent: there are no published studies evaluating the combination approach versus either therapy alone. The rationale is mechanistic, and the clinical decision to combine is based on individual patient assessment rather than protocol-level evidence.
Clinical Perspective — Julian Douwes M.D.
The apheresis landscape for post-COVID and chronic inflammatory conditions is evolving rapidly. H.E.L.P. Apheresis has the evidence base that makes it defensible to any physician or insurance reviewer — 35 years of cardiovascular data, reproducible outcomes, and measurable results. INUSpheresis addresses a different clinical need, targeting the broader toxin and inflammatory load that H.E.L.P. was not designed for. I do not view them as competitors. When a patient presents with elevated Lp(a), high fibrinogen, and post-COVID fatigue, I reach for H.E.L.P. When a patient presents with chronic environmental toxin exposure and multi-system inflammation, INUSpheresis may offer something that H.E.L.P. cannot. The honest position is that both have clinical utility, and the evidence base for one is substantially stronger than the other. Patients deserve to understand that distinction before making a treatment decision.
Key Takeaways
- H.E.L.P. Apheresis uses heparin-mediated precipitation to selectively remove LDL, Lp(a), fibrinogen, and CRP with 35+ years of evidence and multiple published studies.
- INUSpheresis uses adsorption-based filtration to target a broader range of substances including environmental toxins, cytokines, and inflammatory mediators, but has limited published clinical evidence.
- For post-COVID microclotting, H.E.L.P. has the stronger mechanistic and clinical rationale due to its potent fibrinogen reduction.
- For environmental toxin burden and broad detoxification, INUSpheresis addresses targets that H.E.L.P. was not designed for.
- Neither system is a standalone cure — both are components of comprehensive treatment protocols.
- Combining both systems is practiced at some centers but lacks comparative evidence.
- Insurance coverage in Germany is available for H.E.L.P. for approved lipid indications but generally not for INUSpheresis.
References
- Seidel, D., et al. “The HELP-LDL-Apheresis Multicenter Study, an angiographically assessed trial on the role of LDL-apheresis in the secondary prevention of coronary heart disease.” European Journal of Clinical Investigation, 21(4), 1991, pp. 375-383.
- Jaeger, B.R., et al. “Longitudinal cohort study on the effectiveness of lipid apheresis treatment to reduce high lipoprotein(a) levels and prevent major adverse coronary events.” Nature Clinical Practice Cardiovascular Medicine, 6(3), 2009, pp. 229-239.
- Pretorius, E., et al. “Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin.” Cardiovascular Diabetology, 20(1), 2021, 172.
- Bornstein, S.R., et al. “Long-COVID, metabolic and endocrine disease.” Hormone and Metabolic Research, 54(8), 2022, pp. 562-566.
- Klinghardt, D. “INUSpheresis in environmental medicine: clinical observations.” Journal of Environmental Medicine, (observational data cited from INUS Medical clinical reports).