The word “detox” carries significant baggage, and I use it with reservations. In consumer wellness, “detox” often implies that the body is full of unnamed toxins that can be flushed away with a juice cleanse. This is not what I mean.
What I mean is this: the human body has sophisticated detoxification systems — primarily the liver, kidneys, gut, skin, and lungs — that continuously process and eliminate metabolic waste products, environmental chemicals, heavy metals, and microbial byproducts. These systems work well under normal conditions. Under conditions of increased toxic burden, nutrient deficiency, or organ dysfunction, they can become overwhelmed.
Supporting detoxification means ensuring these systems have the substrates, cofactors, and conditions they need to function optimally. It does not mean overriding them with aggressive interventions.
Phase 1: Reduce Incoming Burden (Ongoing)
Before supporting elimination, reduce what is coming in.
Dietary
- Organic produce where feasible, prioritizing the EWG “Dirty Dozen” (highest pesticide residue). Glyphosate exposure from conventional produce is associated with gut microbiome disruption and potentially with hepatic enzyme interference.
- Filtered water — a quality carbon or reverse osmosis filter removes chlorine, fluoride, heavy metals, and pharmaceutical residues. Municipal water treatment does not remove all contaminants.
- Minimize processed food — food additives, preservatives, and packaging chemicals (BPA, phthalates) add to the liver’s processing burden.
- Clean protein sources — grass-fed, wild-caught, organic where possible. Concentrated animal feeding operations (CAFOs) concentrate pesticides, hormones, and antibiotic residues in animal products.
Environmental
- Air quality — HEPA air purifiers in sleeping areas. Indoor air is typically 2-5 times more polluted than outdoor air (EPA data).
- Personal care products — the average person applies over 100 chemicals to their skin daily through conventional products. Switch to EWG-verified or minimal-ingredient alternatives.
- Household cleaning — conventional cleaners contain volatile organic compounds, endocrine disruptors, and respiratory irritants. Vinegar, baking soda, and castile soap handle most cleaning needs.
Phase 2: Liver Support (4-6 Weeks)
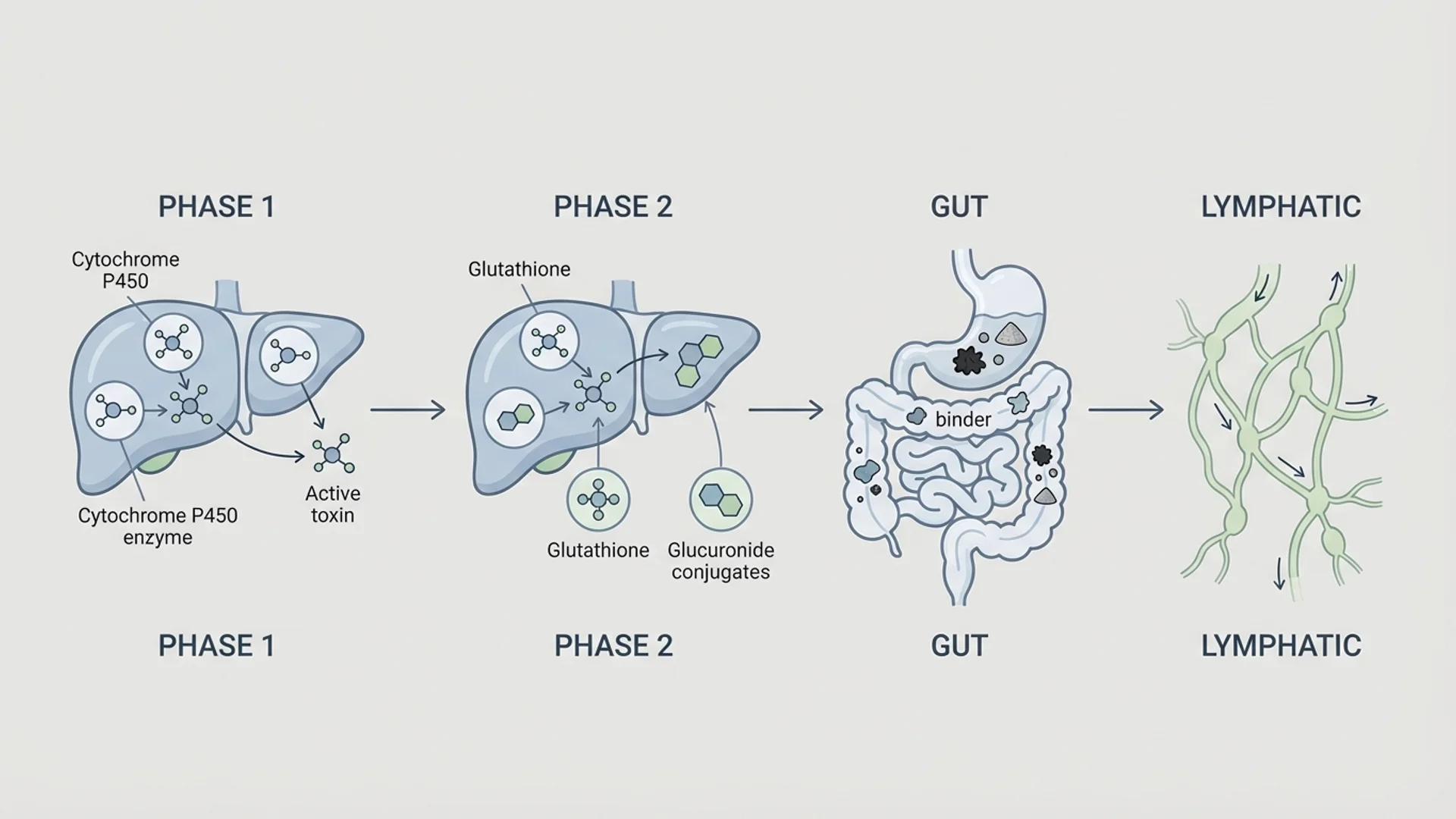
The liver processes toxins in two phases:
Phase 1 (functionalization): Cytochrome P450 enzymes modify toxins, often making them more reactive (and temporarily more toxic). This phase requires B vitamins, vitamin C, and glutathione.
Phase 2 (conjugation): The reactive intermediates from Phase 1 are conjugated (attached to carrier molecules) for excretion. Major Phase 2 pathways include glucuronidation, sulfation, glutathione conjugation, methylation, acetylation, and amino acid conjugation. Each pathway requires specific nutrients.
The critical principle: Phase 1 and Phase 2 must be balanced. Upregulating Phase 1 without adequate Phase 2 capacity produces an accumulation of reactive intermediates that can be more harmful than the original toxins. This is why aggressive “detox” protocols can make people feel worse.
Liver Support Supplements
Supplement Dose Evidence Level Purpose
Milk thistle (silymarin) 200-400 mg standardized extract Moderate (controlled studies) Hepatoprotection, glutathione support, anti-inflammatory
Calcium-D-glucarate 500 mg twice daily Moderate (controlled studies) Supports glucuronidation; inhibits beta-glucuronidase
B complex (methylated) 1 capsule daily Strong (individual B vitamins have RCT evidence) Phase 1 and Phase 2 cofactors
Alpha-lipoic acid 300-600 mg daily Moderate (controlled studies) Antioxidant, heavy metal chelation support
Sulforaphane (from broccoli sprout extract) 30-60 mg daily Moderate (controlled studies) Nrf2 activation, Phase 2 enzyme induction
Glycine 3-5 g daily Moderate (controlled studies) Amino acid conjugation, glutathione synthesis
Dietary Liver Support
- Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, kale) — contain sulforaphane and indole-3-carbinol, which induce Phase 2 enzymes. Evidence level: strong (controlled human studies).
- Sulfur-rich foods (garlic, onions, eggs) — provide sulfur for sulfation pathways.
- Bitter greens (arugula, dandelion greens, endive) — stimulate bile production and flow.
- Adequate protein — Phase 2 amino acid conjugation requires amino acid substrates. Protein-deficient diets impair detoxification capacity.
Phase 3: Binder Support (As Needed)
Binders are substances that bind toxins in the gastrointestinal tract, preventing reabsorption through enterohepatic circulation. This is particularly relevant during antimicrobial therapy (Herxheimer reactions), mold exposure, and active chelation.
Binder Dose Best For Evidence Level
Bentonite clay 1 teaspoon in water daily Mycotoxins, heavy metals Moderate (controlled studies for aflatoxin binding)
Chlorella 3-5 g daily Heavy metals (mercury) Moderate (controlled studies)
Modified citrus pectin 5-15 g daily Heavy metals (lead, mercury) Moderate (controlled studies, notably Eliaz et al.)
Cholestyramine Rx required, per physician dosing Mold toxins, bile acid sequestration Strong (established pharmaceutical)
Critical timing rule: All binders must be taken at least one hour away from medications and supplements. Binders are non-specific — they will bind medications, nutrients, and supplements along with toxins.
Phase 4: Lymphatic and Elimination Support
The lymphatic system transports waste products and immune cells but has no pump — it relies on muscle contraction, breathing, and gravity.
Lymphatic Support
- Movement — daily walking, rebounding (mini-trampoline), or yoga. The lymphatic system requires physical movement to function.
- Dry brushing — brushing the skin with a natural-bristle brush toward the heart before showering. The evidence is traditional rather than clinical, but the practice supports skin circulation and is low-risk.
- Adequate hydration — 30-35 mL per kg body weight daily. Lymphatic fluid is largely water-based.
- Deep breathing — diaphragmatic breathing creates negative intrathoracic pressure that assists lymphatic drainage from the lower body.
Bowel Regularity
Toxins conjugated in the liver are excreted through bile into the intestine. If transit time is slow (constipation), these toxins can be deconjugated by bacterial beta-glucuronidase and reabsorbed. Daily bowel movements are essential for effective detoxification.
If constipation is present: increase fiber (ground flaxseed, 2 tablespoons daily), increase magnesium (citrate form, 400-600 mg), ensure adequate hydration, and increase movement.
Sweating
Sweat is a legitimate elimination pathway for heavy metals and certain organic pollutants. Infrared sauna (20-30 minutes, 3-4 times per week) is the most practical way to induce therapeutic sweating. Evidence for heavy metal excretion through sweat: controlled studies (Genuis et al., multiple publications in Archives of Environmental Contamination and Toxicology).
When to Seek Medical Help
- Symptoms that worsen during the protocol (may indicate mobilization without adequate elimination)
- Known heavy metal exposure requiring chelation therapy
- Mold illness requiring medical management
- Liver enzyme elevations (AST, ALT, GGT) above reference ranges
- Jaundice, dark urine, or pale stool
Disclaimer: This protocol is provided for educational purposes and reflects one physician’s clinical approach. It is not a substitute for individualized medical care. Patients with known toxic exposures or liver disease should work with a physician experienced in environmental medicine.