Key Takeaways:
- BPC-157 and TB-500 are the two most commonly used peptides for tissue repair, with complementary mechanisms of action
- The preclinical evidence for these peptides in musculoskeletal healing is extensive and consistent, but human controlled trials are lacking
- Peptide therapy for recovery works best when integrated with rehabilitation, nutrition, and appropriate rest
- This protocol is not about “faster recovery” at the expense of proper healing — it is about supporting the biological processes of repair
- Individual variation in response is significant, and expectations should be calibrated accordingly
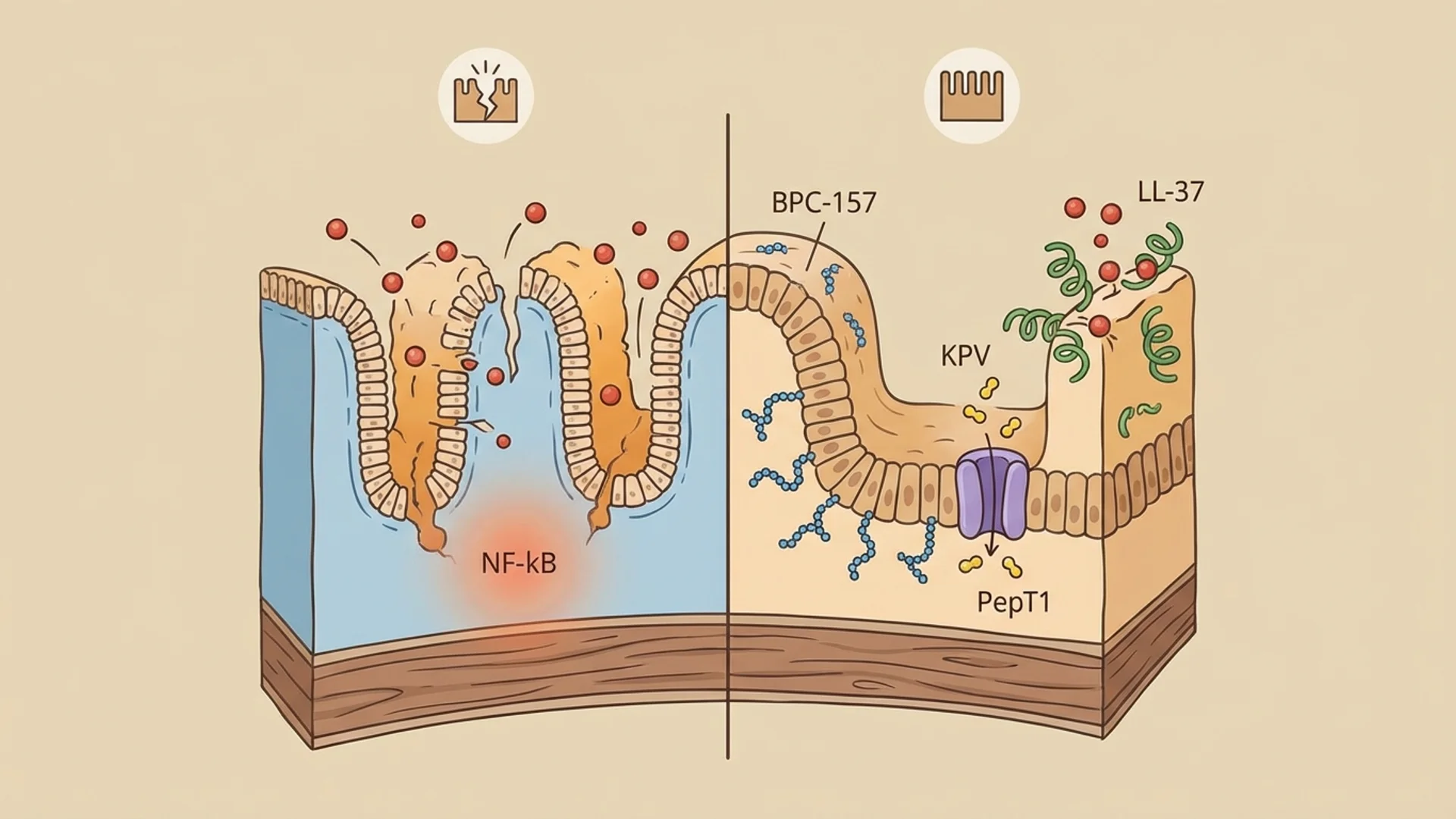
Recovery from injury or surgery is fundamentally a biological process — tissue repair, inflammation resolution, vascular restoration, and functional remodeling. The question that drives interest in peptide therapy for recovery is straightforward: can we support these biological processes with targeted peptide interventions?
The preclinical evidence suggests that the answer is likely yes. BPC-157 and TB-500 have demonstrated consistent, reproducible effects on tissue healing in animal models across dozens of studies and multiple injury types. The clinical question is whether these effects translate to meaningful improvements in human recovery — and the honest answer is that we have encouraging clinical observation but not yet the controlled trial data to be certain.
This protocol reflects my clinical approach to using peptides for recovery from musculoskeletal injury and surgery. It is designed to complement — not replace — appropriate rehabilitation, rest, and surgical management.
Who This Protocol Is For
- Patients recovering from acute musculoskeletal injuries (tendon, ligament, muscle)
- Patients in post-surgical recovery (orthopedic surgery, joint repair, reconstructive procedures)
- Athletes and active individuals with chronic tendinopathies or overuse injuries
- Patients with slow-healing wounds or delayed recovery
- Patients under the supervision of a physician and, where applicable, a physical therapist
Who Should NOT Follow This Protocol Without Medical Supervision
- Patients with active malignancy (angiogenesis promotion concern)
- Patients with active infection at the injury site
- Pregnant or lactating women
- Patients on anticoagulant therapy (consult prescribing physician — vascular effects of these peptides)
- Patients who have not been properly evaluated for the underlying injury (do not treat blindly)
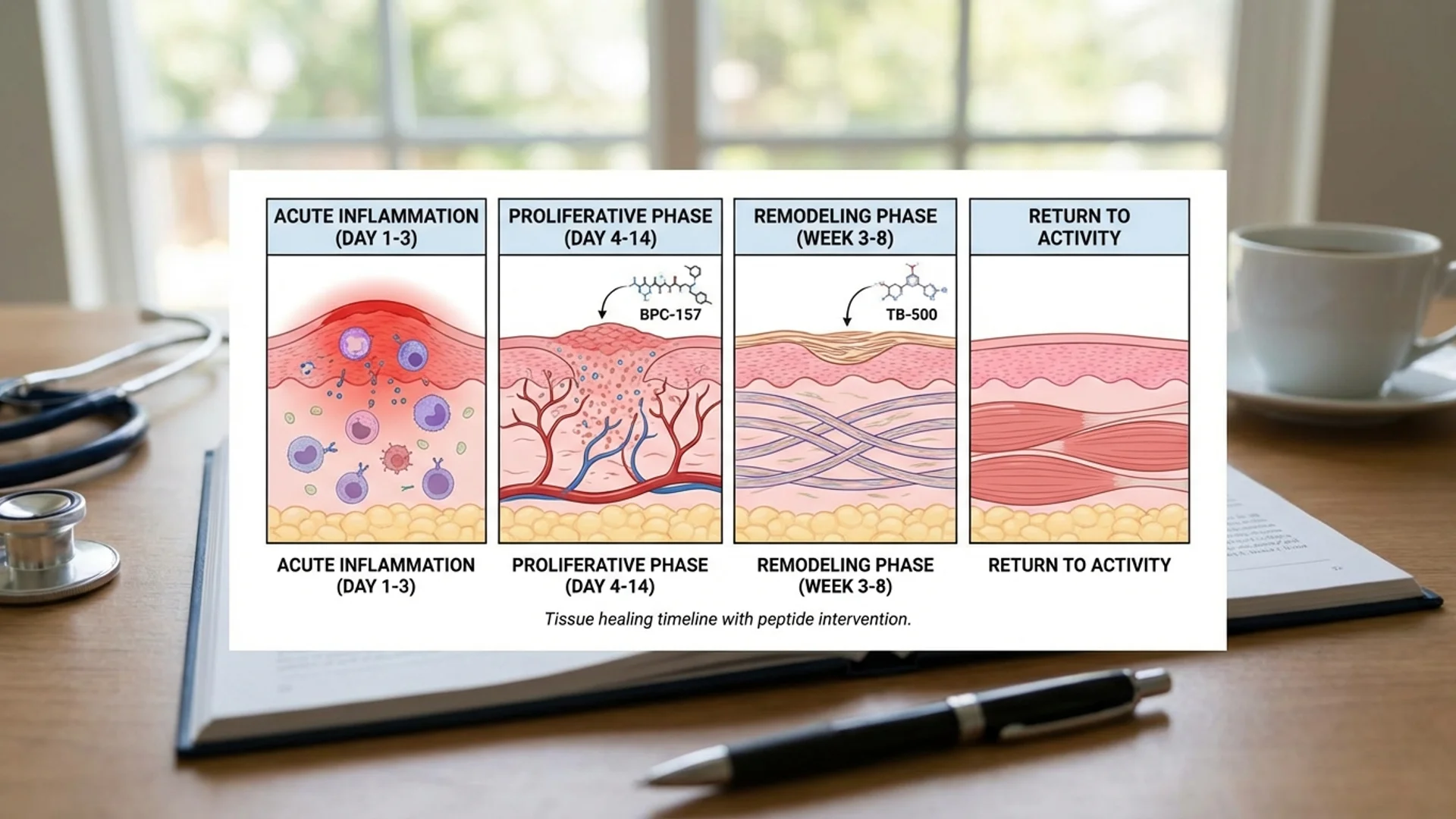
Phase 1: Acute Phase (Days 1-14 Post-Injury or Surgery)
Goal
Support the initial inflammatory response (do not suppress it entirely — controlled inflammation is necessary for healing) while establishing conditions for optimal tissue repair.
Actions
Clinical Assessment:
- Proper diagnosis and imaging of the injury
- Baseline assessment of injury severity and expected recovery timeline
- Surgical consultation if indicated
- Pre-treatment metabolic panel, vitamin D, iron studies
Peptide Protocol (initiate as early as clinically appropriate):
Peptide Dose Route Frequency Duration Evidence Level Purpose
TB-500 2-5 mg SC injection (systemic) Twice weekly Through Phase 1 Animal data, limited human data (parent molecule) Cell migration, anti-inflammatory, anti-fibrotic
Local vs. Systemic Injection: For musculoskeletal injuries, I typically administer BPC-157 locally (subcutaneously near the injury site) when practical, reasoning that higher local concentrations may enhance efficacy at the site of damage. TB-500 is administered systemically because its cell migration effects operate through systemic signaling pathways.
Foundational Support:
Supplement Dose Timing Evidence Level Purpose
Vitamin D3 4,000-5,000 IU/day (adjust to target 50-70 ng/mL) Morning Controlled studies Immune function, tissue repair
Collagen peptides 15-20 g/day 30-60 minutes before rehab Controlled studies (Shaw 2017) Collagen synthesis substrate
Zinc 30 mg/day With meals Controlled studies Wound healing cofactor
Omega-3 (EPA/DHA) 3-4 g/day (acute phase) With meals Controlled studies Anti-inflammatory, resolution
Protein 1.6-2.0 g/kg/day Distributed across meals Controlled studies Tissue repair substrate
Lifestyle:
- RICE/POLICE protocol as appropriate for the injury type
- Sleep optimization (7-9 hours — growth hormone release during sleep is critical for repair)
- Avoid alcohol (impairs healing)
- Avoid NSAIDs if possible in the first 48-72 hours (allow initial inflammatory response to proceed)
What to Expect
The acute phase is about setting the stage for healing. Patients should not expect dramatic improvement in the first 1-2 weeks. Pain should gradually decrease. Swelling follows a normal pattern of peaking in the first 48-72 hours and then gradually resolving. The peptides are supporting biological repair processes that take time.
Phase 2: Proliferative Phase (Weeks 3-8)
Goal
Support active tissue repair — the formation of new blood vessels, collagen deposition, and cell proliferation that rebuild damaged tissue.
Actions
Peptide Protocol (continued):
Peptide Dose Route Frequency Duration Evidence Level Purpose
TB-500 2-5 mg SC injection Once weekly (maintenance) 6 weeks Animal data Continued cell migration, anti-fibrotic
Rehabilitation: This phase is where rehabilitation becomes critical. Peptides support the biological substrate of healing, but appropriate mechanical loading is essential for the proper alignment and strengthening of new tissue.
- Physical therapy per injury-specific protocol
- Gradual, controlled loading (guided by pain response and therapist assessment)
- Collagen peptides taken 30-60 minutes before rehab sessions (per Shaw et al. 2017 protocol)
- Avoid aggressive stretching or loading that exceeds tissue tolerance
Optional Addition (for patients with documented growth hormone insufficiency):
Peptide Dose Route Frequency Duration Evidence Level Purpose
This addition is not appropriate for all patients. I reserve it for patients over 40 with documented low IGF-1 levels who are recovering from significant injuries or surgeries. GH plays a well-documented role in tissue repair, and its decline with age is one factor in slower recovery times among older patients.
Continue:
- All foundational supplements from Phase 1
- Sleep optimization
- Adequate protein intake
What to Expect
This is typically the phase where patients notice the most improvement. Range of motion increases, pain decreases, and functional capacity improves. The rate of improvement varies significantly between patients and between injury types. Tendon injuries, in particular, heal slowly regardless of intervention — patients should expect weeks to months, not days.
Phase 3: Remodeling Phase (Weeks 9-16)
Goal
Support tissue remodeling — the process by which newly formed tissue is reorganized, strengthened, and matured into functional tissue.
Actions
Peptide Protocol (tapering):
Peptide Dose Route Frequency Duration Evidence Level Purpose
TB-500 is discontinued after Phase 2 in most cases. The cell migration and anti-inflammatory effects are most relevant during the acute and proliferative phases.
Rehabilitation (progressive loading):
- Progressive resistance training (guided by therapist)
- Sport-specific or activity-specific movement patterns
- Eccentric loading for tendon injuries (well-supported by evidence)
- Gradual return to full activity
Continue:
- Collagen peptides (maintenance dose: 10 g/day)
- Vitamin D (maintenance)
- Adequate protein
What to Expect
Tissue remodeling continues for months after injury, and the tissue formed during the first 8 weeks continues to mature and strengthen during this phase. Patients often feel “healed” before the tissue has fully remodeled — this is a common point of re-injury. Adherence to progressive loading protocols and avoidance of premature return to full activity is critical.
Phase 4: Return to Activity (Weeks 12-20+)
Goal
Safely return to full activity or sport with mature, resilient tissue.
Actions
Peptides: Discontinued. If recovery has been satisfactory, ongoing peptide therapy is not necessary during this phase.
Rehabilitation:
- Full return-to-activity protocol per therapist guidance
- Gradual increase in intensity, volume, and complexity
- Monitoring for symptom recurrence
- Strength and conditioning to address any deficits identified during recovery
Injury Prevention:
- Address biomechanical factors that contributed to the original injury
- Ongoing strength and mobility work
- Adequate recovery between training sessions
- Nutritional optimization for tissue resilience
What to Expect
Full tissue maturation can take 6-12 months for significant injuries, particularly tendon and ligament injuries. The absence of pain does not mean complete tissue maturation. A conservative approach to return to activity reduces re-injury risk.
When to Seek Medical Help
- Pain that increases rather than decreases during the protocol
- New swelling, redness, or warmth at the injury site (could indicate infection or re-injury)
- Loss of previously regained range of motion
- Signs of allergic reaction to any peptide
- Numbness, tingling, or weakness beyond what is expected for the injury type
- Delayed healing beyond expected timelines (may indicate undiagnosed contributing factors)
Monitoring and Assessment
- Clinical assessment of healing progress at weeks 2, 4, 8, and 12
- Imaging (ultrasound or MRI) at baseline and weeks 8-12 to assess structural healing
- Functional testing per injury type (strength testing, range of motion, sport-specific tests)
- If using GH secretagogues: IGF-1, fasting glucose, and fasting insulin at baseline and week 6
Clinical Perspective
The recovery protocol I have described reflects my attempt to support the body’s healing processes with targeted interventions. I want to be direct about what peptides can and cannot do in this context.
Peptides cannot replace proper rehabilitation. A patient who receives BPC-157 and TB-500 but does not do their physical therapy will not recover as well as a patient who does their physical therapy without peptides. The rehabilitation is the foundation. The peptides are the adjunct.
Peptides cannot override biology. Tendon healing takes time because tendons have poor blood supply and limited regenerative capacity. Peptides may support the healing process, but they do not transform a 12-week recovery into a 4-week recovery. I set this expectation clearly with every patient.
What I have observed in my practice is that patients who receive BPC-157 and TB-500 as part of comprehensive recovery protocols tend to track at the favorable end of expected recovery timelines. They do not heal impossibly fast. They heal well — with good tissue quality, less pain during recovery, and functional outcomes that meet or exceed expectations.
The patients I am most cautious about are athletes who want to use peptides to accelerate return to competition. The risk of returning to full activity before tissue has adequately matured is the same regardless of whether peptides were used. I use the same return-to-activity criteria for peptide-treated patients as for any other patient. The peptides may help achieve those criteria sooner, but the criteria themselves should not change.
The honest answer is that we need controlled human trials comparing recovery outcomes with and without peptide therapy. Until those trials are conducted, I rely on the strong preclinical data, the growing body of clinical observation, and the principle that supporting the biological mechanisms of healing — angiogenesis, cell migration, collagen synthesis, inflammation resolution — is unlikely to cause harm and is likely to help.
References
- Sikiric P, et al. “Pentadecapeptide BPC 157 and its role in accelerating musculoskeletal soft tissue healing.” PM&R. 2020;12(12):1326-1334.
- Krivic A, et al. “Achilles detachment in rat and stable gastric pentadecapeptide BPC 157.” J Orthop Surg Res. 2006;1:23.
- Bock-Marquette I, et al. “Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair.” Nature. 2004;432(7016):466-472.
- Malinda KM, et al. “Thymosin beta 4 accelerates wound healing.” J Invest Dermatol. 1999;113(3):364-368.
- Shaw G, et al. “Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis.” Am J Clin Nutr. 2017;105(1):136-143.
- Seiwerth S, et al. “BPC 157 and Standard Angiogenic Growth Factors.” Curr Pharm Des. 2018;24(18):1972-1989.
- Sosne G, et al. “Thymosin beta 4: a potential novel therapy for neurotrophic keratopathy, dry eye, and ocular surface diseases.” Vitam Horm. 2016;102:277-306.
Disclaimer: This protocol is provided for educational purposes and reflects one physician’s clinical approach to injury recovery. It is not a substitute for individualized medical care, proper diagnosis, or rehabilitation under a qualified therapist. Consult a qualified physician before beginning any peptide or supplement protocol.