You have tried antidepressants — maybe two, maybe five. Some helped partially. Some caused side effects that were worse than the depression itself. And now someone has suggested TMS, and you are wondering whether it actually works or whether this is just another expensive clinic selling hope.
Let me be direct: TMS for depression is not experimental. It is not alternative medicine. It is an FDA-cleared treatment with two decades of controlled clinical evidence, endorsed by every major psychiatric guideline in the world. The question is not whether it works — the question is whether it will work for you, and what protocol gives you the best chance.
At a Glance
| Property | Detail |
|---|---|
| Evidence Level | Strong (multiple large RCTs, meta-analyses, FDA clearance) |
| Primary Use | Treatment-resistant major depressive disorder |
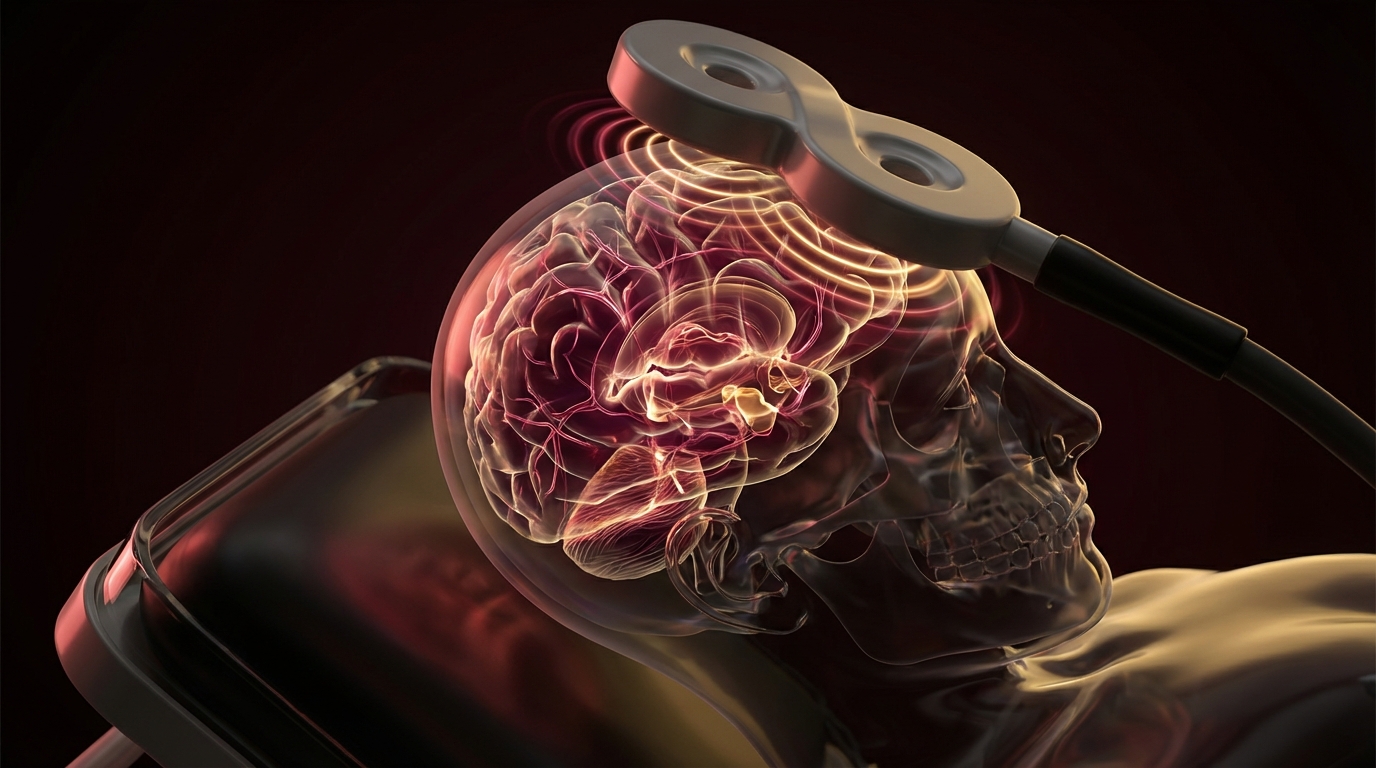
| Key Mechanism | Repetitive electromagnetic stimulation of the left dorsolateral prefrontal cortex (DLPFC) |
| FDA Clearance | rTMS for depression (2008), deep TMS (2013), theta burst (2018) |
| Response Rate | 50-60% (at least 50% symptom reduction) |
| Remission Rate | 30-35% (full symptom resolution) |
TMS Depression Treatment: The 20-Year Track Record
The FDA Clearance Story
In October 2008, the FDA cleared the first repetitive TMS (rTMS) device — the NeuroStar system by Neuronetics — for treatment-resistant major depressive disorder. The pivotal trial was a multisite, randomized, sham-controlled study of 301 patients who had failed at least one adequate antidepressant trial [1].
That initial clearance was based on a specific protocol: high-frequency (10 Hz) stimulation of the left dorsolateral prefrontal cortex (DLPFC), delivered in 37.5-minute sessions, five days per week, for 4-6 weeks. The rationale was straightforward — neuroimaging studies consistently showed that the left DLPFC was hypoactive in depression, and high-frequency rTMS increases cortical excitability.
Since 2008, the evidence base has expanded enormously:
- 2013: FDA clearance for deep TMS (Brainsway H-coil system) for depression
- 2018: FDA clearance for theta burst stimulation (TBS) protocols, reducing session time from 37 minutes to approximately 3 minutes
- 2020: FDA clearance for the SAINT protocol (Stanford Accelerated Intelligent Neuromodulation Therapy), an intensive protocol delivering 10 sessions per day over 5 days
Each clearance was backed by controlled trial data. This is not a treatment that was approved based on anecdote or marketing — it accumulated evidence through the same rigorous process as any pharmaceutical.
Why the STAR*D Trial Matters
To understand why TMS matters, you need to understand the STAR*D trial — the largest study of antidepressant treatment ever conducted [2].
STAR*D enrolled over 4,000 patients with major depressive disorder and systematically stepped them through escalating medication strategies. The results were sobering:
- Step 1 (first antidepressant): ~33% remission rate
- Step 2 (switch or augment): ~25% cumulative additional remission
- Step 3 (third medication strategy): ~12-20% additional remission
- Step 4 (fourth strategy): ~10-15% additional remission
By the time a patient has failed two or more adequate medication trials, the probability of remission with another medication drops to roughly 10-15%. These are the patients for whom TMS was designed — and where it offers response rates three to four times better than another medication switch.
This is the context that matters. TMS is not competing with first-line antidepressants. It is filling a gap that medications cannot.
How TMS Works for Depression
The Mechanism
Depression is not simply a “chemical imbalance” — that model has been oversimplified to the point of being misleading. What neuroimaging and circuit-level research shows is that depression involves dysfunctional connectivity between specific brain networks, particularly:
- Hypoactivity of the left DLPFC: Reduced activity in the left dorsolateral prefrontal cortex, a region involved in executive function, emotional regulation, and cognitive control
- Hyperactivity of the subgenual anterior cingulate cortex (sgACC): Excessive activity in a region associated with rumination, negative self-referential processing, and autonomic stress responses
- Disrupted default mode network (DMN) connectivity: Abnormal patterns in the brain’s “resting state” network, associated with persistent rumination
High-frequency rTMS to the left DLPFC directly addresses the first of these — it increases cortical excitability and metabolic activity in a region that is underperforming. But the effects are not limited to the stimulation site. Through transsynaptic connections, DLPFC stimulation modulates activity in deeper limbic structures including the sgACC [3].
This is why TMS is not just a local treatment — it modulates circuits, not just a single brain region.
Neuroplasticity
A single TMS session produces transient changes in cortical excitability. Repeated sessions — delivered daily over weeks — produce lasting neuroplastic changes. This is analogous to how a single exercise session produces temporary cardiovascular changes, but consistent training produces structural adaptation.
The neuroplastic mechanisms include:
- Long-term potentiation (LTP)-like effects: Strengthening of synaptic connections in stimulated circuits
- Neurotransmitter modulation: Changes in dopamine, serotonin, and GABA signaling in targeted regions
- Structural changes: Imaging studies show changes in cortical thickness and white matter integrity after TMS treatment courses [4]
- Network normalization: Functional connectivity patterns begin to resemble those seen in non-depressed individuals
The Protocols: rTMS, Deep TMS, and Theta Burst
Standard rTMS (10 Hz Protocol)
The original and most extensively studied protocol:
- Target: Left DLPFC
- Frequency: 10 Hz (high frequency = excitatory)
- Pulses per session: 3,000
- Session duration: ~37 minutes
- Treatment course: 5 sessions/week for 4-6 weeks (20-30 sessions total)
- Motor threshold: Adjusted to individual cortical excitability
This protocol has the deepest evidence base. A 2019 meta-analysis of 81 randomized controlled trials involving over 4,200 patients confirmed that active rTMS was significantly more effective than sham for both response and remission [5].
Deep TMS (H-Coil)
Standard figure-8 coils stimulate cortex at a depth of approximately 1.5-2 cm. The H-coil, developed by Brainsway, generates a broader and deeper magnetic field pattern that can stimulate structures at 3-4 cm depth.
For depression, the advantage is more direct engagement of limbic circuits. The DSMB (data safety monitoring board) for the pivotal trial recommended early termination due to clear efficacy — meaning the treatment effect was so strong that it was unethical to continue randomizing patients to sham [6].
In my clinical practice, I view deep TMS as an important advance, but the evidence advantage over standard rTMS is not yet definitive. What I can say is that some patients who did not respond adequately to standard rTMS do respond to deep TMS protocols — likely because of the increased depth of stimulation.
Theta Burst Stimulation (TBS)
This is where the field got interesting. Theta burst stimulation uses a patterned delivery of pulses — three pulses at 50 Hz, repeated every 200 ms (5 Hz theta rhythm) — that mimics endogenous hippocampal firing patterns. This pattern is thought to be particularly effective at inducing neuroplastic changes.
The THREE-D trial (2018) was a landmark non-inferiority study comparing intermittent TBS (iTBS) to standard 10 Hz rTMS in 414 patients with treatment-resistant depression [7]. The results:
- iTBS was non-inferior to standard rTMS on all efficacy measures
- Response rates: iTBS 49% vs. rTMS 47%
- Remission rates: iTBS 32% vs. rTMS 28%
- Session duration: iTBS ~3 minutes vs. rTMS ~37 minutes
Let me be clear about what this means: the same clinical outcome in 3 minutes instead of 37. This transformed the practical delivery of TMS, making it more accessible, less burdensome, and more scalable.
The SAINT Protocol (Stanford Accelerated Protocol)
The most ambitious evolution of TMS for depression is the Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol, developed by Nolan Williams and colleagues [8].
SAINT uses:
- Functional MRI-guided targeting: Instead of anatomical landmarks, the exact stimulation target is personalized based on the individual’s functional connectivity — specifically, the DLPFC subregion most anti-correlated with the sgACC
- Intensive dosing: 10 sessions per day, 50 minutes apart, for 5 consecutive days (50 total sessions in one week)
- Theta burst delivery: iTBS pattern for rapid session completion
The open-label results were remarkable: 90% remission rate in 21 treatment-resistant patients [8]. The subsequent randomized, sham-controlled trial confirmed these results with a 79% remission rate in the active treatment group versus 13% in sham [9].
Here is what the evidence shows: the SAINT protocol represents the most potent TMS approach currently available. The remission rates substantially exceed anything achieved with standard protocols. The limitation is that it requires functional MRI infrastructure and an extremely intensive treatment schedule.
Response Rates: Who Responds Best?
Overall Numbers
Across meta-analyses and large pragmatic studies, the general response rates for standard rTMS in treatment-resistant depression are:
- Response (≥50% improvement on depression scales): 50-60%
- Remission (full symptom resolution): 30-35%
- Durability: Most responders maintain benefits at 6-12 months, some require maintenance sessions
These numbers deserve context. These are patients who have already failed multiple treatments. A 50-60% response rate in this population is substantially better than what another medication trial offers.
Predictors of Response
Clinical research has identified several factors associated with better TMS outcomes:
Favorable predictors:
- Shorter duration of current depressive episode
- Fewer failed medication trials (1-2 rather than 5+)
- Absence of personality disorder comorbidity
- Non-psychotic depression
- Functional MRI-guided targeting (as in SAINT)
- Higher treatment adherence (completing all sessions)
Less favorable predictors:
- Very chronic, treatment-refractory depression (multiple failed medication trials and psychotherapy)
- Comorbid severe anxiety disorders
- Active substance use disorder
- Psychotic features
In my clinical experience, the patients who respond best to TMS are those with moderate-to-severe depression who have failed 1-3 medication trials and are relatively earlier in their treatment journey. This does not mean that patients with more extensive treatment histories cannot respond — many do — but the probability is lower.
Combination with Medication
An important clinical point: TMS is not typically used in isolation. Most patients continue their current antidepressant regimen during TMS treatment. The combination appears to be at least additive, and some data suggests synergistic effects — particularly when TMS is combined with medications that enhance neuroplasticity [10].
What I tell my patients: TMS is not a replacement for medication in most cases. It is an augmentation strategy that addresses different aspects of the neurobiology. Some patients are eventually able to reduce or discontinue medications after successful TMS, but that decision should be made gradually with psychiatric guidance.
What a Treatment Course Looks Like
Initial Evaluation
Before TMS, patients should have a comprehensive psychiatric assessment confirming treatment-resistant major depressive disorder. Screening for contraindications is essential:
- Absolute contraindications: Metallic implants in or near the head (excluding dental fillings), cochlear implants, implanted brain stimulators
- Relative contraindications: Epilepsy or seizure history (TMS carries a small seizure risk, approximately 0.1%), unstable neurological conditions, pregnancy (limited safety data)
The Treatment Session
A typical standard rTMS session:
- Motor threshold determination (first session): The coil is positioned over the motor cortex, and stimulation intensity is gradually increased until a visible thumb twitch is produced. This calibrates the treatment intensity to the individual’s cortical excitability.
- Coil positioning: The coil is moved to the left DLPFC treatment target, typically 5-6 cm anterior to the motor cortex “hot spot.” Advanced protocols use neuronavigation for more precise targeting.
- Stimulation delivery: Pulses are delivered in trains — typically 4 seconds on, 26 seconds off for 10 Hz protocols. Patients feel a tapping or clicking sensation on the scalp. It is not painful, though some patients find the first few sessions uncomfortable.
- Duration: 3 minutes (theta burst) to 37 minutes (standard 10 Hz).
- Frequency: Five days per week for 4-6 weeks.
Patients can drive themselves to and from treatment. There is no anesthesia, no sedation, and no recovery period. Most patients return to normal activities immediately after each session.
What to Expect
Most patients do not notice dramatic improvement during the first week. The neuroplastic changes take time to consolidate. A typical response trajectory:
- Weeks 1-2: Minimal change, some patients report subtle improvements in sleep or energy
- Weeks 2-3: Gradual improvement in mood, motivation, and cognitive clarity
- Weeks 3-6: Continued improvement, with maximum benefit often not reached until after the treatment course is complete
Some patients experience a delayed response — significant improvement occurring 2-4 weeks after completing the treatment course. This is consistent with the neuroplastic mechanism and is a reason not to judge efficacy prematurely.
After Treatment: Durability and Maintenance
How Long Do Results Last?
The durability data is encouraging but imperfect. A naturalistic study following TMS responders found that approximately 60-70% maintained their response at 12 months [11]. Those who relapsed typically did so within the first 6 months.
Factors associated with longer durability include:
- Achieving full remission (vs. partial response)
- Continuing antidepressant medication
- Ongoing psychotherapy
- Lifestyle factors (exercise, sleep, social connection)
Maintenance TMS
For patients who respond well but experience gradual recurrence, maintenance TMS — periodic “booster” sessions — is a practical strategy. There is no universally standardized maintenance protocol, but common approaches include:
- Weekly sessions for 1-2 months after the initial course, then tapering
- Monthly sessions indefinitely for patients with recurrent depression
- “As needed” retreatment at the first sign of symptom return
In my clinical experience, maintenance TMS every 2-4 weeks helps sustain remission in patients with recurrent depression who would otherwise relapse despite medication. This is an active area of research, and formal guidelines for optimal maintenance protocols are still evolving.
Safety
TMS has an excellent safety profile. The most common side effects:
- Scalp discomfort at the treatment site (most common, typically mild, improves over sessions)
- Headache (occurs in approximately 30% of patients, usually mild and responsive to OTC analgesics)
- Lightheadedness (transient, typically the first few sessions)
The most serious potential risk is seizure. The estimated risk is approximately 0.1% per treatment course — comparable to the background seizure risk of many commonly prescribed antidepressants. In practice, seizures during TMS are exceedingly rare when safety parameters are followed appropriately.
There is no evidence of cognitive impairment, personality change, or memory loss from TMS. This is a meaningful distinction from electroconvulsive therapy (ECT), which — while highly effective — carries cognitive side effects that concern many patients.
TMS vs. Other Treatments for Resistant Depression
TMS vs. ECT
ECT remains the most effective acute treatment for severe, treatment-resistant depression, with remission rates of 50-70%. However, it requires general anesthesia, causes temporary cognitive side effects (particularly autobiographical memory impairment), and carries significant stigma.
TMS offers lower remission rates but a far more favorable side effect profile, no anesthesia requirement, and no cognitive impairment. For many patients, TMS is the appropriate first step before considering ECT.
TMS vs. Ketamine/Esketamine
Ketamine and esketamine (Spravato) offer rapid antidepressant effects — sometimes within hours. TMS effects develop over weeks. However, TMS produces more durable changes without the dissociative side effects, abuse potential, and requirement for in-clinic monitoring that ketamine involves.
These are not competing treatments — they serve different clinical needs and can be combined.
TMS vs. Psychotherapy
TMS and psychotherapy address depression through fundamentally different mechanisms. TMS modulates brain circuits directly. Psychotherapy changes cognitive and behavioral patterns. The combination is logical and, in my clinical observation, often more effective than either alone.
The Bottom Line
Twenty years of evidence have established TMS as a legitimate, effective treatment for depression that has not responded to medication. The response rates are strong, the safety profile is excellent, and the technology continues to evolve — theta burst and the SAINT protocol represent meaningful advances in both efficacy and convenience.
What I tell my patients who are considering TMS: this is not a last resort, and it is not a gamble. It is a well-studied treatment that works for roughly half of the people who try it when medications have failed. Those odds are substantially better than switching to yet another antidepressant.
The nuance matters, though. Not every TMS protocol is equivalent. Not every patient is an ideal candidate. And finding a provider who uses evidence-based protocols with proper targeting makes a real difference in outcomes. Ask questions, review the protocols, and make an informed decision.
References
- O’Reardon JP, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biological Psychiatry. 2007;62(11):1208-1216. PMID: 17573044.
- Rush AJ, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. American Journal of Psychiatry. 2006;163(11):1905-1917. PMID: 17074942.
- Fox MD, et al. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biological Psychiatry. 2012;72(7):595-603. PMID: 22658708.
- Lan MJ, et al. Transcranial magnetic stimulation of left dorsolateral prefrontal cortex induces brain morphological changes in regions associated with a treatment-resistant major depressive episode. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2016;65:109-114. PMID: 26407269.
- Brunoni AR, et al. Repetitive transcranial magnetic stimulation for the acute treatment of major depressive episodes: a systematic review with network meta-analysis. JAMA Psychiatry. 2017;74(2):143-152. PMID: 27898482.
- Levkovitz Y, et al. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. 2015;14(1):64-73. PMID: 25655160.
- Blumberger DM, et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. The Lancet. 2018;391(10131):1683-1692. PMID: 29726344.
- Cole EJ, et al. Stanford Accelerated Intelligent Neuromodulation Therapy for treatment-resistant depression. American Journal of Psychiatry. 2020;177(8):716-726. PMID: 32252538.
- Cole EJ, et al. Stanford Neuromodulation Therapy (SNT): a double-blind randomized controlled trial. American Journal of Psychiatry. 2022;179(2):132-141. PMID: 34711062.
- Donse L, et al. Simultaneous rTMS and psychotherapy in major depressive disorder: clinical outcomes and predictors from a large naturalistic study. Brain Stimulation. 2018;11(2):337-345. PMID: 29191438.
- Dunner DL, et al. A multisite, naturalistic, observational study of transcranial magnetic stimulation for patients with pharmacoresistant major depressive disorder: durability of benefit over a 1-year follow-up period. Journal of Clinical Psychiatry. 2014;75(12):1394-1401. PMID: 25271871.