At a Glance
| Property | Value |
|---|---|
| Evidence Level | Strong (polysomnographic studies, longitudinal cohorts linking sleep architecture to mortality) |
| Primary Use | Understanding and optimizing sleep quality beyond total duration |
| Key Mechanism | Cyclic alternation of NREM/REM stages driven by circadian and homeostatic processes |
Sleep Stages and Longevity: Why Total Hours Is Not Enough
You sleep 7.5 hours per night. Your tracker says you got 35 minutes of deep sleep and 55 minutes of REM. Is that enough? Should you be worried?
These are questions I get constantly, and the answer requires more nuance than most sleep content provides. Total sleep duration matters — but sleep architecture matters at least as much, and possibly more, for long-term health outcomes.
Here is what the evidence shows about how much of each sleep stage you actually need, what happens when you do not get enough, and what you can realistically do about it.
The Four Stages of Sleep
Every night, your brain cycles through four distinct stages in approximately 90-minute cycles, repeating 4-6 times per night:
Stage N1: Light Sleep (2-5% of total sleep)
The transition from wakefulness to sleep. Muscle tone decreases. Brain waves shift from alpha (8-12 Hz) to theta (4-7 Hz). You can be easily awakened. This stage has minimal restorative value but is a necessary gateway.
Stage N2: Intermediate Sleep (45-55% of total sleep)
The dominant sleep stage by time. Characterized by sleep spindles (12-14 Hz bursts) and K-complexes on EEG. Heart rate and body temperature decrease. Sleep spindles are increasingly recognized as important for memory consolidation and synaptic plasticity. This stage is not “filler” — it serves important functions, but it is also the stage that expands to fill the gap when deep sleep and REM are suppressed.
Stage N3: Deep Sleep / Slow-Wave Sleep (13-23% of total sleep)
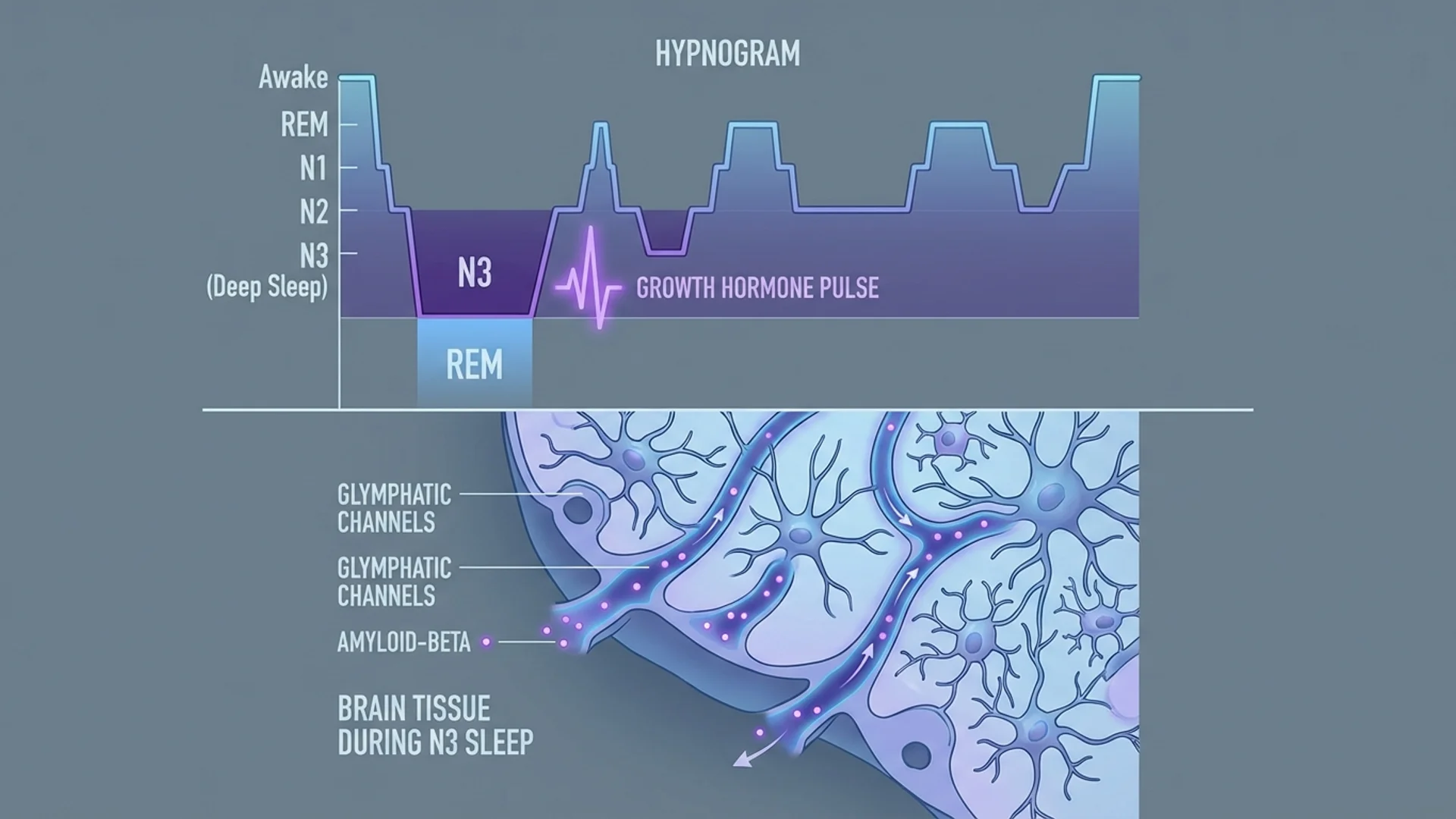
The most physically restorative stage. Defined by high-amplitude delta waves (0.5-2 Hz) dominating the EEG. During N3:
- Growth hormone release peaks. 70-80% of daily GH secretion occurs during deep sleep, primarily in the first N3 episode of the night.
- Glymphatic clearance activates. The brain’s waste disposal system increases activity 10-20 fold during deep sleep, clearing amyloid-beta and tau proteins. This is directly relevant to Alzheimer’s disease risk.
- Immune function consolidates. Cytokine production, T-cell redistribution, and immune memory formation occur preferentially during deep sleep.
- Tissue repair accelerates. Protein synthesis increases, cellular damage is repaired, and energy stores are replenished.
REM Sleep (20-25% of total sleep)
Rapid eye movement sleep is neurologically distinct from all other stages. The brain becomes nearly as active as during wakefulness, while the body is paralyzed (atonia) to prevent acting out dreams. During REM:
- Memory consolidation occurs. Specifically, procedural memory, emotional memory, and creative problem-solving are processed during REM.
- Emotional regulation is maintained. REM sleep processes emotional experiences and reduces the amygdala’s reactivity to negative stimuli. Chronic REM deprivation is strongly linked to anxiety and depression.
- Neural connectivity is pruned and strengthened. Synaptic homeostasis during REM is essential for learning capacity.
How Much Do You Need? Targets by Age
The following targets are derived from polysomnographic normative data and population studies:
Deep Sleep (N3) Targets
| Age Range | Deep Sleep (minutes) | % of Total Sleep | Notes |
|---|---|---|---|
| 18-25 | 80-120 | 18-23% | Peak deep sleep capacity |
| 25-35 | 60-100 | 15-20% | Gradual decline begins |
| 35-50 | 50-80 | 13-18% | Noticeable reduction; optimize aggressively |
| 50-65 | 35-60 | 10-15% | Significant decline; intervention important |
| 65+ | 20-45 | 5-12% | Substantial loss; focus on preservation |
REM Sleep Targets
| Age Range | REM Sleep (minutes) | % of Total Sleep | Notes |
|---|---|---|---|
| 18-25 | 90-120 | 20-25% | Abundant REM |
| 25-35 | 80-110 | 20-25% | Relatively stable |
| 35-50 | 75-100 | 18-22% | Modest decline |
| 50-65 | 60-90 | 15-20% | Gradual reduction |
| 65+ | 50-80 | 13-18% | Meaningful decline |
Important context: These are population averages from polysomnographic studies. Individual variation exists. Some people function well with less than average deep sleep; others need more. The trends, however, are consistent: both deep sleep and REM decline with age, and this decline has health consequences.
The Mortality Connection
The most compelling reason to care about sleep architecture — beyond how you feel — is the mortality data.
Djonlagic et al. analyzed data from the Outcomes of Sleep Disorders in Older Men (MrOS) study and found that reduced N3 sleep was associated with a 29% increase in all-cause mortality in men over 65, independent of total sleep duration (1). Let me emphasize that: total sleep could be adequate (7-8 hours), but if the proportion spent in deep sleep was low, mortality risk increased.
For REM sleep, Leary et al. found that each 5% reduction in REM sleep was associated with a 13% increase in all-cause mortality in community-dwelling older adults (2).
These are observational associations, not proven causal relationships. But the consistency across multiple cohorts, the biological plausibility (immune function, glymphatic clearance, cardiovascular regulation), and the dose-response relationship all point in the same direction: sleep architecture is a biomarker of biological aging and a potential intervention target.
The 90-Minute Cycle: Why Distribution Matters
Sleep stages are not evenly distributed through the night. The architecture follows a predictable pattern:
First half of the night (cycles 1-2): Deep sleep dominates. The longest and most intense N3 episodes occur in the first 3 hours after sleep onset. This is when most growth hormone is released and the bulk of glymphatic clearance occurs.
Second half of the night (cycles 3-5): REM sleep dominates. REM episodes become progressively longer through the night, with the final REM period (typically 5-7 AM) lasting 30-60 minutes.
The practical implication: If you go to bed late but still get 7 hours, you lose proportionally more deep sleep (because you miss the early-night window). If you wake up early, you lose proportionally more REM (because you cut the late-night REM periods). Both truncations have different health consequences.
This is why shift workers, even those who sleep 7-8 hours during the day, often have profound sleep architecture disruption — the circadian system gates deep sleep and REM to specific times, and sleeping at the wrong phase means lower-quality architecture regardless of total duration.
What Your Sleep Tracker Is Actually Measuring
A note of caution about consumer sleep trackers. Devices like Oura Ring, Whoop, Apple Watch, and Garmin estimate sleep stages using accelerometry (movement) and heart rate variability, sometimes supplemented with skin temperature. They are not polysomnography.
What they do well:
- Total sleep time (reasonably accurate, ±30 minutes)
- Sleep-wake detection (good at distinguishing sleep from wakefulness)
- Trend tracking (relative changes over time are more reliable than absolute values)
What they do poorly:
- Deep sleep quantification (accuracy varies widely; Oura tends to overestimate, Whoop tends to underestimate compared to PSG)
- REM vs. light sleep distinction (the most error-prone classification)
- Absolute stage durations (can be off by 30-50%)
My recommendation: Use tracker data for trends, not absolutes. If your deep sleep average drops from 80 minutes to 40 minutes over 3 months, that is meaningful regardless of the absolute accuracy. But do not panic over a single night showing 15 minutes of deep sleep — the device may simply have miscategorized a significant portion.
How to Optimize Each Stage
Increasing Deep Sleep
This is the primary focus for most longevity-oriented patients. The full protocol is in my how to increase deep sleep naturally guide. The highest-impact interventions:
- Cool bedroom (18-19°C)
- Consistent wake time
- Exercise 4-6 hours before bed
- Eliminate alcohol (reduces deep sleep 24-39%)
- Magnesium glycinate 400 mg + glycine 3g before bed
Increasing REM Sleep
REM optimization requires different strategies:
- Protect the late-sleep window. REM dominates hours 5-8 of sleep. If you sleep only 6 hours, you are selectively eliminating REM.
- Manage stress. High cortisol suppresses REM. Evening stress-reduction practices (meditation, breathwork, journaling) protect REM architecture.
- Avoid alcohol. Alcohol suppresses REM even more dramatically than deep sleep — REM rebound (excessive, vivid dreaming) occurs when alcohol wears off in the second half of the night, but net REM time is reduced.
- Avoid THC/cannabis. THC is a potent REM suppressant. Chronic users often report dream cessation — this is REM elimination, not a benefit.
- Manage medications. Many common medications suppress REM: SSRIs, SNRIs, tricyclic antidepressants, beta-blockers, and benzodiazepines. If you take any of these, discuss sleep architecture effects with your physician.
Sleep Architecture as a Longevity Biomarker
In my clinical practice, I increasingly view sleep architecture as a biomarker of biological aging — similar to how we use HRV, VO2 max, or grip strength. A 55-year-old with the deep sleep profile of a 40-year-old is biologically younger in a meaningful sense. The interventions that improve deep sleep — temperature regulation, exercise, stress management, circadian alignment — are the same interventions that improve virtually every other longevity biomarker.
This is not coincidence. Sleep architecture is both a reflection of biological age and a driver of it. Fix the sleep, and the downstream effects cascade into metabolic health, immune function, cognitive performance, and emotional resilience.
The Bottom Line
Healthy sleep requires not just enough hours, but the right architecture: 13-23% deep sleep for physical restoration and 20-25% REM for cognitive and emotional health. Both decline with age, and both predict mortality independently of total sleep time. Track trends, not absolute numbers. Prioritize the behavioral interventions — temperature, consistency, exercise timing, alcohol elimination — before supplements or devices. Sleep architecture is one of the most modifiable longevity biomarkers available to you.
References
-
Djonlagic I, Mariani S, Fitzpatrick AL, et al. Macro and micro sleep architecture and cognitive performance in older adults. Nature Human Behaviour. 2021;5(1):123-145. doi:10.1038/s41562-020-00964-y
-
Leary EB, Watson KT, Ancoli-Israel S, et al. Association of rapid eye movement sleep with mortality in middle-aged and older adults. JAMA Neurology. 2020;77(10):1241-1251. doi:10.1001/jamaneurol.2020.2108
-
Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals. Sleep. 2004;27(7):1255-1273. doi:10.1093/sleep/27.7.1255
-
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377. doi:10.1126/science.1241224