If a pharmaceutical company developed a drug that improved immune function, enhanced memory consolidation, regulated metabolic hormones, cleared neurotoxic waste from the brain, and reduced all-cause mortality by 15-20%, it would be the best-selling medication in history. That drug is sleep. The problem is that it cannot be patented, so it receives a fraction of the attention it deserves.
I say this not as hyperbole but as a reflection of the evidence. Sleep is the single most undervalued longevity intervention, and in my clinical experience, it is the one most frequently compromised by patients who are otherwise meticulous about their health.
Understanding Sleep Architecture
Sleep is not a uniform state. It consists of distinct stages, each with specific physiological functions:

Stage N1 (Light sleep): The transition from wakefulness. Brief, typically 5-10% of total sleep time. Minimal restorative value.
Stage N2 (Intermediate sleep): Comprises 45-55% of total sleep. Important for motor skill consolidation and memory processing. Characterized by sleep spindles and K-complexes on EEG.
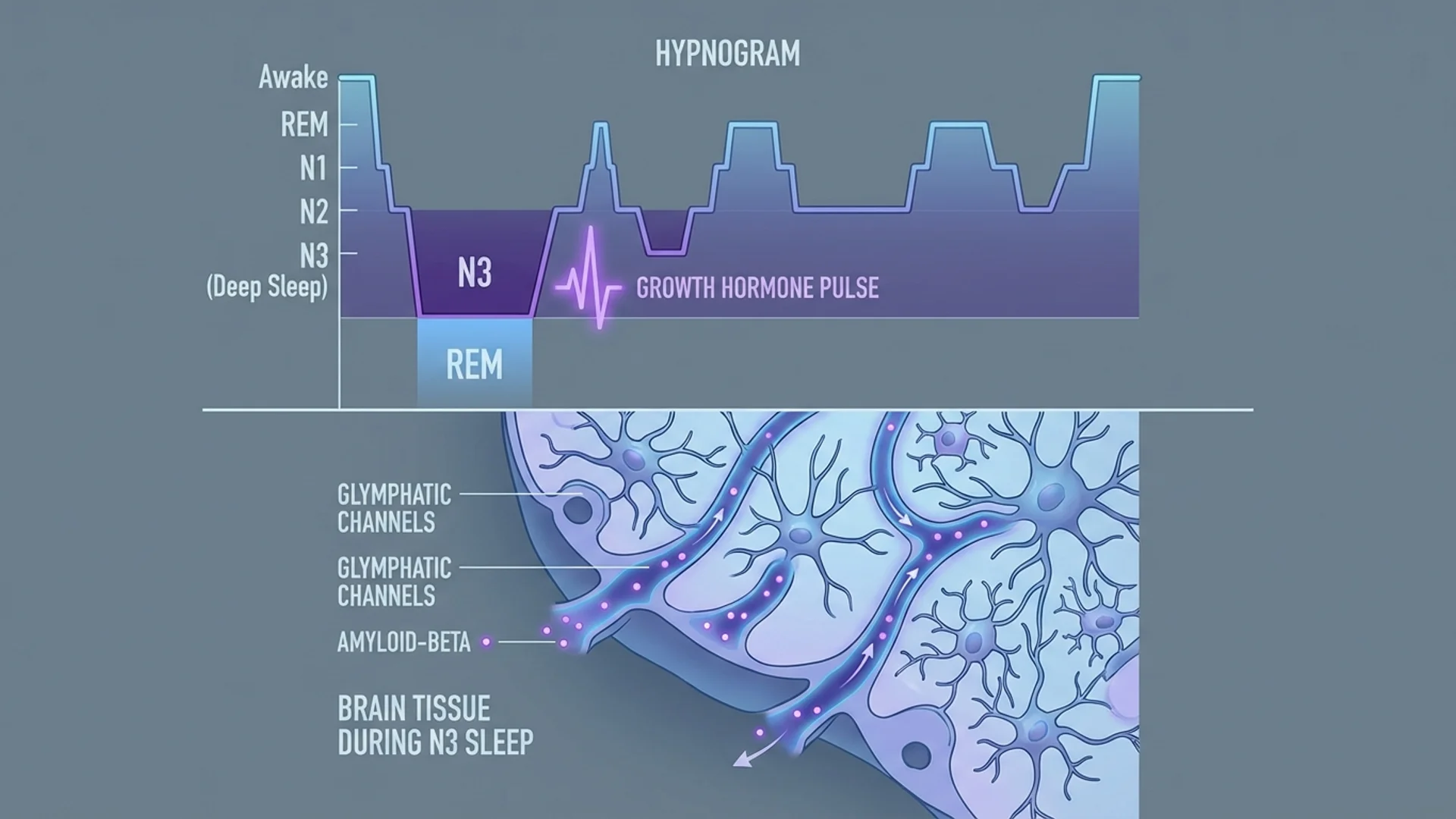
Stage N3 (Deep/slow-wave sleep): The most restorative stage. Constitutes 15-25% of sleep in young adults but declines significantly with age — sometimes to 5% or less by the sixties. During deep sleep:
- Growth hormone is secreted (80% of daily GH release occurs during N3)
- The glymphatic system clears metabolic waste, including amyloid-beta, from the brain [1]
- Immune function is enhanced
- Tissue repair occurs
- Mitochondrial restoration takes place
REM sleep: Comprises 20-25% of total sleep. Essential for emotional processing, memory consolidation, and cognitive function. Dreams occur primarily during REM. REM sleep increases in the latter half of the night, which is one reason that cutting sleep short disproportionately reduces REM time.
The Age-Related Decline
Deep sleep declines with age in a pattern that parallels many other hallmarks of aging. By age 50, a person may have lost 60-70% of the deep sleep they had at age 25 [2]. This is not benign. Reduced deep sleep correlates with:
- Decreased growth hormone secretion
- Impaired glymphatic clearance (potentially contributing to neurodegeneration)
- Reduced immune competence
- Metabolic dysregulation
Whether this decline is a cause of aging, a consequence, or both remains an active area of investigation. What is clear is that interventions that improve deep sleep tend to improve the markers we associate with biological age.
Optimization Strategies
Environment
- Temperature: Core body temperature must drop 1-2 degrees Fahrenheit to initiate sleep. A cool bedroom (65-68 degrees F / 18-20 degrees C) facilitates this. Warming the hands and feet (paradoxically) helps by promoting peripheral vasodilation and core cooling.
- Light: Complete darkness. Even dim light during sleep suppresses melatonin and disrupts circadian signaling. Blackout curtains or a quality sleep mask are not luxuries — they are tools.
- Sound: Consistent low-frequency background sound (white or pink noise) can mask disruptive noises. Silence is preferable if achievable.
Timing
- Consistency is more important than duration. Going to sleep and waking at the same times — including weekends — synchronizes circadian rhythms and improves sleep efficiency.
- Light exposure: Morning bright light (ideally sunlight within 30 minutes of waking) anchors the circadian clock. Evening blue light restriction supports melatonin onset.
Supplements (Evidence-Based)
Magnesium (glycinate or threonate, 200-400 mg before bed): Supports GABA receptor function and has demonstrated modest improvements in sleep quality in controlled trials. Magnesium threonate may have particular relevance for cognitive function due to its ability to cross the blood-brain barrier.
Glycine (3 g before bed): Has shown improvements in subjective sleep quality and next-day alertness in small controlled trials. Likely works by lowering core body temperature.
Melatonin (0.3-1 mg, 30-60 minutes before desired sleep onset): Useful for circadian rhythm adjustment and in older adults with documented melatonin deficiency. Most over-the-counter melatonin products are dosed far too high (3-10 mg), which can cause morning grogginess and potential receptor desensitization. Lower doses are more physiological and often more effective.
Micronized progesterone (for women, by prescription): As noted in my women’s hormone article, oral micronized progesterone has sleep-promoting effects via GABA modulation.
Apigenin (50 mg before bed): A flavonoid found in chamomile with mild anxiolytic and sleep-promoting properties. The evidence is preliminary but the safety profile is favorable.
What to Avoid
- Alcohol: Despite its sedative effect, alcohol fragments sleep architecture, suppresses REM and deep sleep, and is one of the most common causes of poor sleep quality that patients do not recognize.
- Late caffeine: Caffeine has a half-life of 5-6 hours. Afternoon caffeine, even if it does not prevent sleep onset, can reduce deep sleep duration.
- Late heavy meals: Eating large meals within three hours of bedtime can impair sleep quality through thermal and digestive effects.
- Chronic sleep aids: Benzodiazepines and Z-drugs (zolpidem, zopiclone) produce sedation, not restorative sleep. They suppress deep sleep and REM. Long-term use is associated with cognitive decline and falls. I actively taper patients off these medications when possible.
When to Investigate Further
Not all sleep problems are lifestyle problems. I refer for formal sleep evaluation when patients present with:
- Persistent daytime somnolence despite adequate sleep duration
- Witnessed apneas or heavy snoring
- Restless leg symptoms
- Morning headaches or dry mouth (suggesting mouth breathing or apnea)
- Treatment-resistant insomnia
Sleep apnea in particular is dramatically underdiagnosed and has profound implications for cardiovascular health, metabolic function, and longevity.
The Bottom Line
Sleep is not optional. It is not a productivity inefficiency. It is the biological process during which your body repairs, restores, and consolidates the gains from every other health intervention you pursue. No supplement, therapy, or protocol can compensate for chronically inadequate sleep.
In my practice, I address sleep before adding any other longevity intervention. The foundation must be solid before you build on it.

References
- Xie L, et al. Sleep Drives Metabolite Clearance from the Adult Brain. Science. 2013;342(6156):373-377.
- Mander BA, Winer JR, Walker MP. Sleep and Human Aging. Neuron. 2017;94(1):19-36.
This content is educational and does not constitute medical advice. Persistent sleep disorders should be evaluated by a qualified physician.