When a cell is damaged beyond repair but does not die, it enters a state called senescence. It stops dividing, but it remains metabolically active — secreting inflammatory cytokines, growth factors, and proteases that damage surrounding tissue. These cells have been called “zombie cells,” and while the term is informal, it captures something important: they are neither fully alive nor appropriately dead, and they cause real harm.
Senescent cells accumulate with age. By the time a person reaches their seventies, they may represent a meaningful fraction of cells in certain tissues. The senescence-associated secretory phenotype — SASP — drives chronic inflammation, impairs tissue repair, and appears to accelerate other hallmarks of aging [1].
The senolytic hypothesis is straightforward: if we can selectively eliminate senescent cells, we might slow or partially reverse aspects of aging. The animal data supporting this hypothesis is among the most striking in all of longevity medicine.
What the Animal Data Shows
In 2015, researchers at Mayo Clinic demonstrated that eliminating senescent cells in genetically modified mice extended median lifespan by approximately 25% [2]. The treated mice showed improved cardiac function, reduced cancer incidence, and delayed onset of age-related pathology.
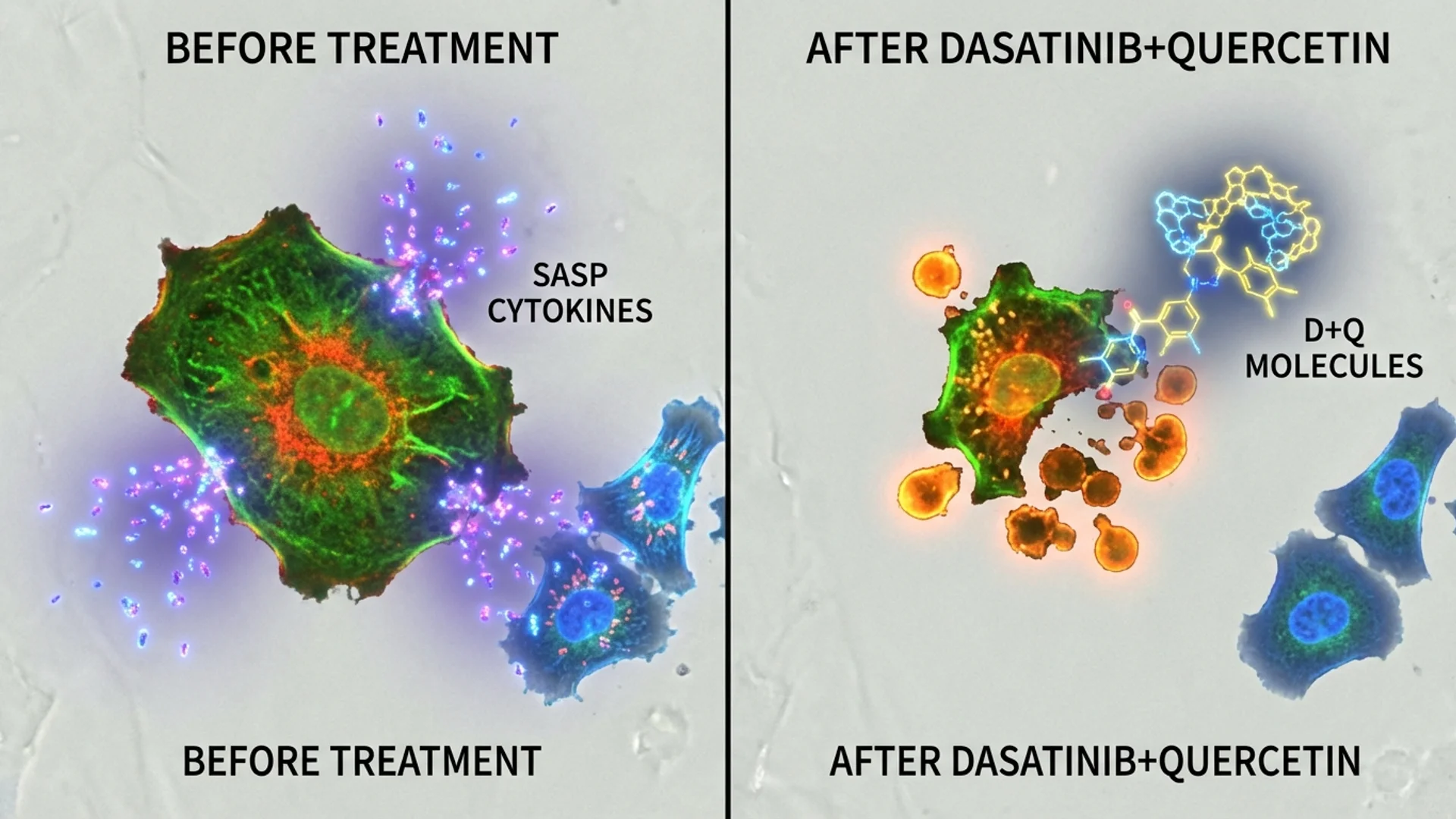
Subsequent studies using pharmacological senolytics — rather than genetic engineering — confirmed and extended these findings. Dasatinib plus quercetin (D+Q), administered intermittently to aged mice, improved physical function, reduced age-related pathology, and extended lifespan [3]. Fisetin, a naturally occurring flavonoid, showed similar senolytic activity in mouse models [4].
I want to be clear about the evidence hierarchy here. These are animal studies. They are well-designed, reproducible, and mechanistically coherent. But the history of medicine is full of interventions that worked beautifully in mice and failed in humans. This deserves continued research, and it deserves honest framing.
The Key Senolytic Compounds
Dasatinib + Quercetin (D+Q)
Dasatinib is an FDA-approved tyrosine kinase inhibitor used in leukemia treatment. Quercetin is a plant flavonoid found in onions, apples, and supplements. Together, they target different pro-survival pathways that senescent cells use to resist apoptosis.
The combination was identified through a hypothesis-driven screen by Kirkland and colleagues [3]. It has been the most extensively studied senolytic combination in both animal and human research.
Human data: A small, open-label study in patients with idiopathic pulmonary fibrosis (a disease associated with high senescent cell burden) showed that intermittent D+Q improved physical function measures after three weeks of treatment [5]. Larger trials are underway.
Important caveat: Dasatinib is a prescription chemotherapy agent with real side effects, including pleural effusions, cytopenias, and gastrointestinal disturbance. It should not be used casually. In my practice, I prescribe D+Q only after careful patient selection, thorough baseline assessment, and with appropriate monitoring.
Fisetin
Fisetin is a flavonoid with demonstrated senolytic activity in preclinical models. It is available as a supplement, which has made it popular in the longevity community. The AFFIRM-LITE trial at Mayo Clinic evaluated fisetin in older adults, and results have been mixed — some benefit signals but not the dramatic effects some had hoped for.
The advantage of fisetin is its favorable safety profile. The disadvantage is uncertainty about its senolytic potency in humans at achievable doses. The bioavailability of standard fisetin supplements is poor, and whether currently available formulations achieve senolytic concentrations in target tissues has not been established.
Other Compounds Under Investigation
- Navitoclax (ABT-263): A potent senolytic targeting BCL-2 family proteins. Effective in preclinical models but carries significant hematological toxicity (thrombocytopenia), limiting its clinical utility.
- FOXO4-DRI: A peptide that disrupts the p53-FOXO4 interaction in senescent cells. Promising preclinical data, but peptide delivery and cost remain challenges.
- UBX0101: A small molecule targeting MDM2/p53 interaction. Failed in a Phase II trial for osteoarthritis, raising questions about whether the approach was too narrowly targeted.
How I Use Senolytics in Practice
I want to be transparent about my approach. Senolytics are not a standard-of-care treatment for aging. They are an investigational strategy with compelling preclinical rationale and limited but growing human data.
When I prescribe senolytic protocols, I do so:
- In patients with clear evidence of accelerated biological aging or high inflammatory burden
- After comprehensive baseline assessment, including inflammatory markers, biological age testing, and organ function evaluation
- Using intermittent dosing — typically two to three consecutive days per month, consistent with the published protocols
- With appropriate monitoring before, during, and after treatment
- With informed consent that includes honest discussion of the evidence limitations
My typical D+Q protocol follows the published Mayo Clinic approach: dasatinib 100 mg plus quercetin 1,000 mg daily for three consecutive days, repeated monthly for three to six months, then reassessed based on biomarkers.
For patients who prefer a supplement-only approach, I discuss fisetin at higher doses (approximately 20 mg/kg on two consecutive days monthly), with the caveat that the human senolytic efficacy at these doses is not established.
What I Have Observed
In my clinical experience with senolytic protocols, I have observed:
- Modest improvements in inflammatory markers (hsCRP, IL-6) in some patients
- Subjective improvements in energy and joint comfort in approximately half of treated patients
- In a subset of patients undergoing serial biological age testing, stabilization or modest improvement in epigenetic age scores
I have also observed patients who showed no measurable response. Individual variation plays a significant role, and we do not yet have reliable predictors of who will respond.
The Honest Limitations
Several important questions remain unanswered:
- Optimal dosing in humans. The D+Q doses used in trials were adapted from cancer treatment protocols, not derived from human dose-finding studies specifically for senolytic effects.
- Long-term safety. Intermittent senolytic therapy appears well-tolerated in short-term studies, but we do not have five- or ten-year safety data.
- Which senescent cells to target. Not all senescent cells are harmful. Some play beneficial roles in wound healing and tumor suppression. A blunt senolytic approach may have unintended consequences.
- Measurement challenges. We lack validated, accessible biomarkers for senescent cell burden in living humans. This makes it difficult to confirm that senolytics are actually clearing their targets.
The Bottom Line
Senolytics represent one of the most scientifically grounded approaches in longevity medicine. The mechanistic rationale is clear, the animal data is strong, and the early human data is cautiously encouraging.
But this is an area where the evidence hierarchy matters. We are still early. I use senolytics selectively, monitor carefully, and maintain honest expectations with my patients. The field is advancing rapidly, and I expect the next five years to bring substantially more clarity.
References
- Childs BG, et al. Senescent cells: an emerging target for diseases of ageing. Nature Reviews Drug Discovery. 2017;16(10):718-735.
- Baker DJ, et al. Clearance of p16Ink4a-positive senescent cells delays ageing-associated disorders. Nature. 2011;479(7372):232-236.
- Zhu Y, et al. The Achilles’ heel of senescent cells: from transcriptome to senolytic drugs. Aging Cell. 2015;14(4):644-658.
- Yousefzadeh MJ, et al. Fisetin is a senotherapeutic that extends health and lifespan. EBioMedicine. 2018;36:18-28.
- Justice JN, et al. Senolytics in idiopathic pulmonary fibrosis: Results from a first-in-human, open-label, pilot study. EBioMedicine. 2019;40:554-563.
This content is educational and does not constitute medical advice. Senolytic therapy is investigational and should only be undertaken under medical supervision. Dasatinib is a prescription medication with significant potential side effects.