The supplement industry generates over $50 billion annually in the United States alone, and longevity supplements represent one of its fastest-growing segments. The marketing is sophisticated, the claims are often impressive, and the evidence behind individual products varies from robust to nonexistent.
What I tell my patients is this: supplements are tools, not solutions. They supplement — literally — a foundation of sleep, exercise, nutrition, and stress management. No supplement compensates for a poor foundation. But for patients who have the foundation in place, targeted supplementation can provide meaningful additional benefit.
The key is knowing which supplements have evidence, which are reasonable bets, and which are marketing without substance.
Tier 1: Strong Evidence, Broad Applicability
These supplements have consistent data from randomized controlled trials in humans, address common deficiencies, and have favorable safety profiles.

Vitamin D3
Why: Vitamin D deficiency affects an estimated 40-60% of adults globally. It influences immune function, bone health, mood, cancer risk, and cardiovascular health. Multiple meta-analyses support supplementation in deficient individuals.
Dose: 2,000-5,000 IU daily, adjusted based on blood levels (target: 40-60 ng/mL). Always take with fat for absorption.
Evidence level: Strong (multiple RCTs, meta-analyses).
Omega-3 Fatty Acids (EPA/DHA)
Why: Anti-inflammatory, cardioprotective, neuroprotective. The REDUCE-IT trial showed significant cardiovascular benefit with high-dose EPA (icosapent ethyl) in high-risk patients [1]. General population studies are more mixed but consistently show benefits for triglyceride reduction and inflammation.
Dose: 2-4 g combined EPA+DHA daily. Prioritize EPA-dominant formulations for cardiovascular and anti-inflammatory effects.
Evidence level: Strong for cardiovascular risk reduction and inflammation; moderate for cognitive protection.
Magnesium
Why: Involved in over 300 enzymatic reactions. Deficiency is common (estimated 50% of the Western population is below optimal intake) and contributes to muscle cramps, poor sleep, insulin resistance, and cardiovascular risk.
Dose: 200-400 mg elemental magnesium daily. Forms matter: glycinate and threonate are well-absorbed; oxide is poorly absorbed.
Evidence level: Strong for deficiency correction; moderate for sleep and cardiovascular benefit.
Creatine Monohydrate
Why: Not just for athletes. Creatine supports ATP regeneration in all tissues, including the brain. Evidence supports benefits for cognitive function (particularly in sleep-deprived individuals and vegetarians), muscle mass preservation in aging, and possibly neuroprotection [2].
Dose: 3-5 g daily. No need for loading protocols.
Evidence level: Strong for muscle performance; moderate-to-strong for cognitive benefit.
Vitamin K2 (MK-7)
Why: Directs calcium to bones and away from arteries. Works synergistically with vitamin D3. Deficiency is common, particularly in populations not consuming fermented foods.
Dose: 100-200 mcg daily (MK-7 form).
Evidence level: Moderate-to-strong for bone health; moderate for cardiovascular protection.
Tier 2: Good Evidence, Targeted Applicability
These have meaningful evidence but are most useful in specific contexts or populations.
Coenzyme Q10 (Ubiquinol)
Why: Essential for mitochondrial electron transport. Levels decline with age and are further depleted by statin medications. See my mitochondrial medicine article.
Dose: 100-300 mg daily (ubiquinol form). Essential for statin users.
Evidence level: Strong for statin-associated myopathy; moderate for general mitochondrial support.
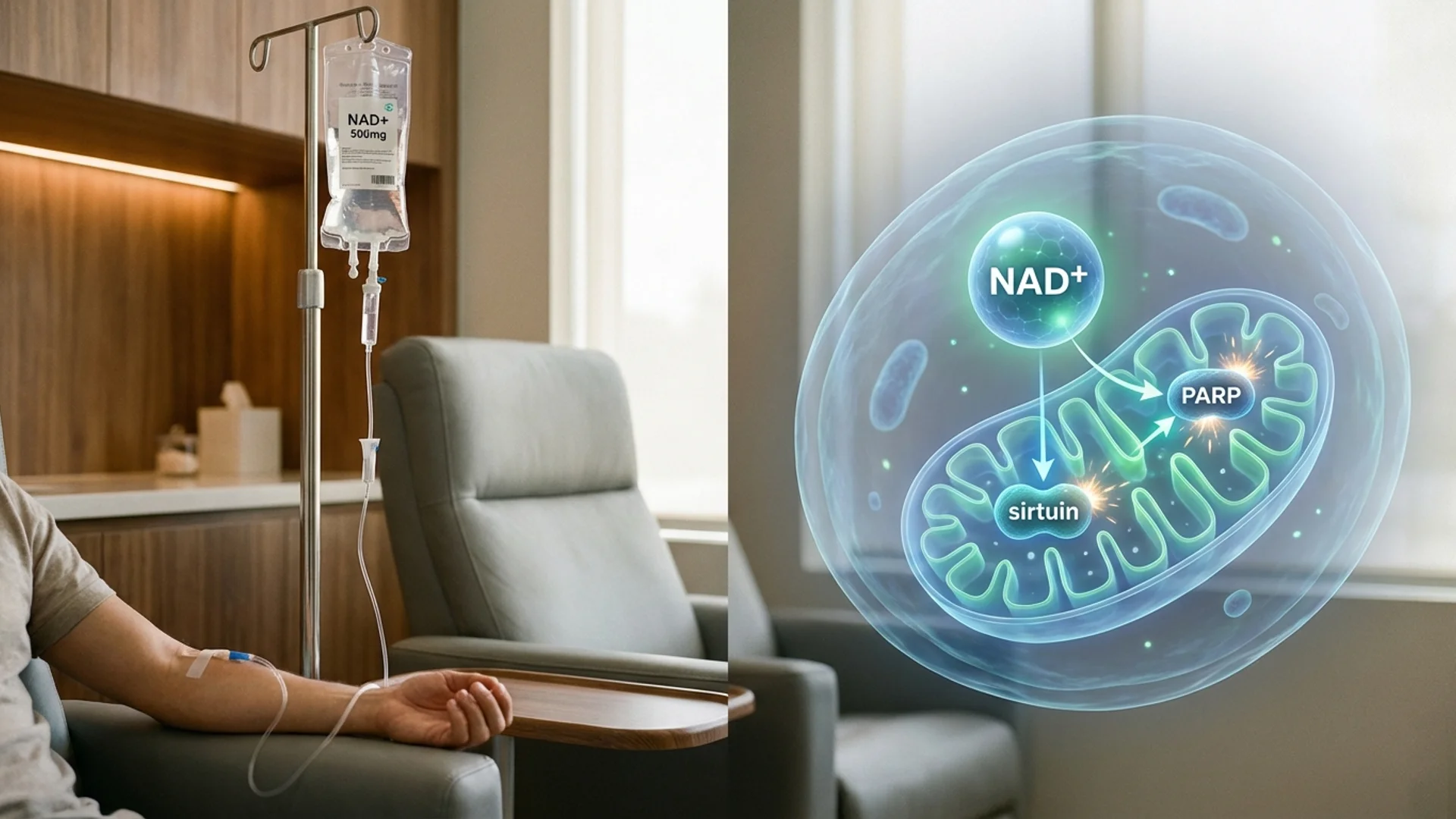
NAD+ Precursors (NMN or NR)
Why: Support NAD+ levels, which decline with age. See my NAD+ article for detailed discussion.
Dose: NMN 500-1,000 mg daily or NR 300-600 mg daily.
Evidence level: Moderate (growing human trial data; strong mechanistic rationale).
Curcumin (Bioavailable Forms)
Why: Anti-inflammatory, potentially disease-modifying for multiple conditions. Standard curcumin has poor bioavailability — formulations with piperine, phytosomes, or liposomal delivery are necessary.
Dose: 500-1,000 mg daily of a bioavailable formulation.
Evidence level: Moderate (multiple human trials for inflammation and joint health; highly variable study quality).
Alpha-Lipoic Acid
Why: Mitochondrial antioxidant, supports glutathione recycling, has evidence for diabetic neuropathy and general antioxidant support.
Dose: 300-600 mg daily, preferably R-alpha-lipoic acid.
Evidence level: Moderate (well-established for neuropathy; less data for general longevity).
Tier 3: Promising but Preliminary
These have interesting mechanistic data and/or early human studies but lack robust, large-scale RCTs.
Spermidine
A polyamine with autophagy-inducing properties. Observational studies associate higher dietary spermidine intake with reduced cardiovascular mortality [3]. Supplemental studies in humans are small but intriguing.
Dose: 1-6 mg daily.
Fisetin
Potential senolytic and anti-inflammatory flavonoid. See my senolytics article.
Dose: As a daily supplement: 100-500 mg. As intermittent senolytic: higher doses per my senolytics discussion.
Glycine
An amino acid that supports glutathione synthesis, collagen production, and sleep quality. Combined with N-acetylcysteine (GlyNAC), it has shown preliminary benefit for oxidative stress reduction in aging adults.
Dose: 3-5 g daily.
PQQ (Pyrroloquinoline Quinone)
Stimulates mitochondrial biogenesis. Human data is limited but mechanistically interesting.
Dose: 10-20 mg daily.
What I Generally Do Not Recommend
- High-dose antioxidant cocktails: The era of megadose vitamin C, vitamin E, and beta-carotene for longevity is over. Multiple large trials showed no benefit and, in some cases, harm. Targeted antioxidant support (CoQ10, ALA, vitamin C at moderate doses) is different from indiscriminate antioxidant loading.
- Proprietary longevity blends with undisclosed doses: If a product does not tell you how much of each ingredient is included, it is impossible to assess whether the doses are therapeutic or merely decorative.
- Supplements for which the primary evidence is animal studies, marketed as if the evidence is human: The evidence hierarchy matters here. Promising mouse data is interesting. It is not a treatment recommendation.
How to Build Your Personal Stack
- Test first. Blind supplementation is inefficient. Blood work (see my longevity panel article) identifies actual deficiencies and guides prioritization.
- Start with Tier 1. Address deficiencies and add broadly applicable, well-evidenced supplements first.
- Add Tier 2 based on individual needs. Statin users need CoQ10. Patients with mitochondrial concerns benefit from NAD+ precursors. Not everyone needs everything.
- Consider Tier 3 as optional. These are reasonable additions for patients who want to be at the frontier, with the understanding that the evidence is less definitive.
- Quality matters. Third-party testing (NSF, USP, ConsumerLab) provides some assurance of purity and potency. The supplement industry is poorly regulated, and what is on the label is not always what is in the bottle.
- Reassess regularly. Supplement needs change with age, health status, and the addition of other interventions. Annual review is appropriate.
The Bottom Line
A thoughtful, evidence-tiered supplement program can meaningfully complement the foundations of longevity. The key is honest assessment of the evidence level for each intervention, individualization based on testing, and realistic expectations about what supplements can and cannot achieve.
References
- Bhatt DL, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. New England Journal of Medicine. 2019;380(1):11-22.
- Avgerinos KI, et al. Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials. Experimental Gerontology. 2018;108:166-173.
- Eisenberg T, et al. Cardioprotection and lifespan extension by the natural polyamine spermidine. Nature Medicine. 2016;22(12):1428-1438.
This content is educational and does not constitute medical advice. Supplement decisions should be guided by laboratory testing and discussed with a qualified physician, particularly if you take prescription medications.