Every cell in the human body — with the exception of mature red blood cells — contains mitochondria. A single cell can house hundreds to thousands of them. They produce approximately 90% of the ATP that powers cellular function. When they work well, you feel it. When they do not, you feel that too.
Mitochondrial dysfunction is one of the 12 hallmarks of aging, but in my clinical experience, it is also one of the most practical targets for intervention. Patients with impaired mitochondrial function present with fatigue, cognitive decline, exercise intolerance, and metabolic disturbance — symptoms that are common, debilitating, and frequently dismissed as “normal aging.”
They are common. They should not be dismissed.
How Mitochondria Decline
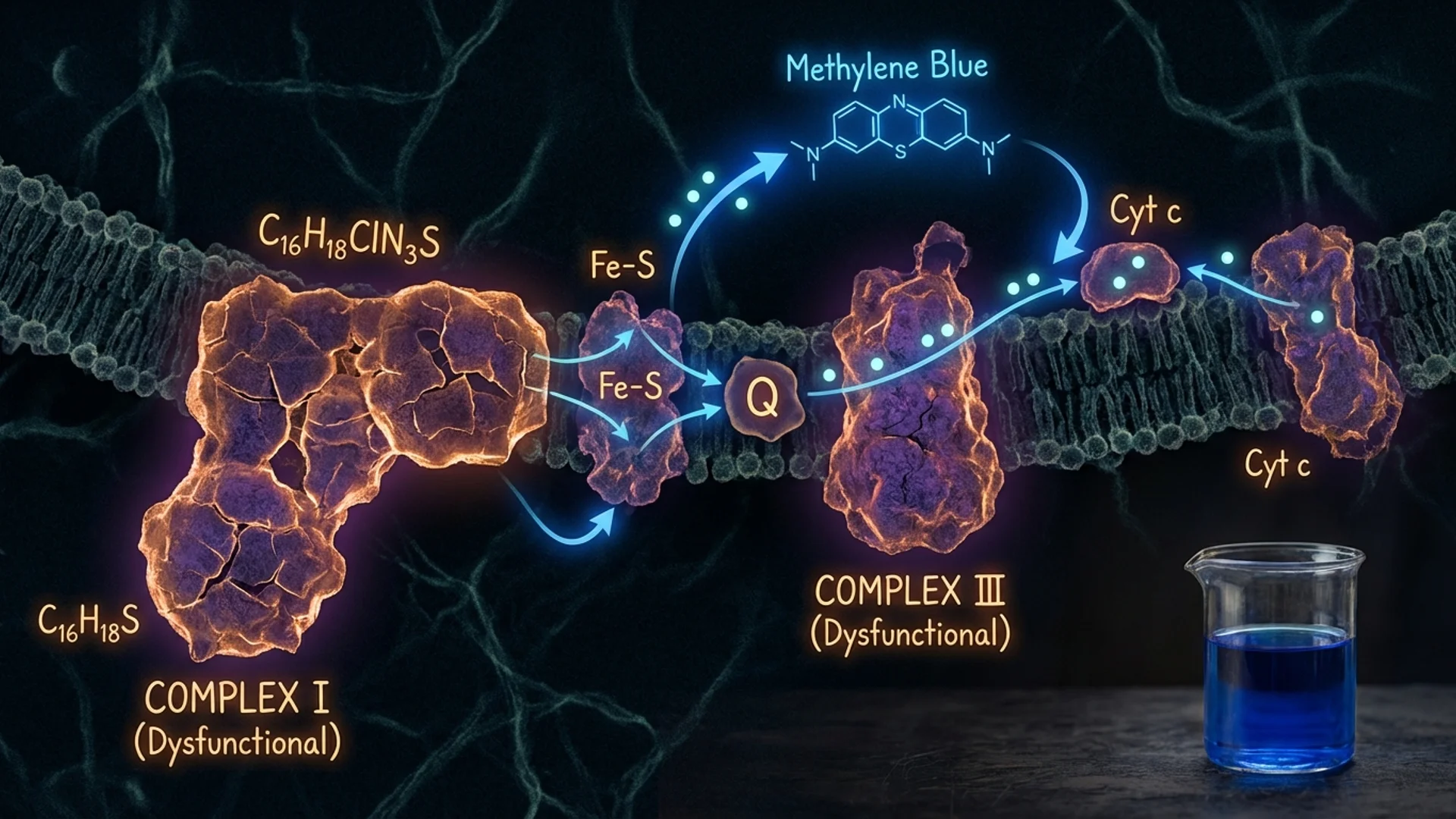
Mitochondria have their own DNA (mtDNA), inherited maternally, which encodes 13 essential components of the electron transport chain. This DNA is particularly vulnerable to damage because it lacks the robust repair mechanisms that protect nuclear DNA and sits in close proximity to the reactive oxygen species (ROS) that mitochondria produce as a byproduct of energy generation.
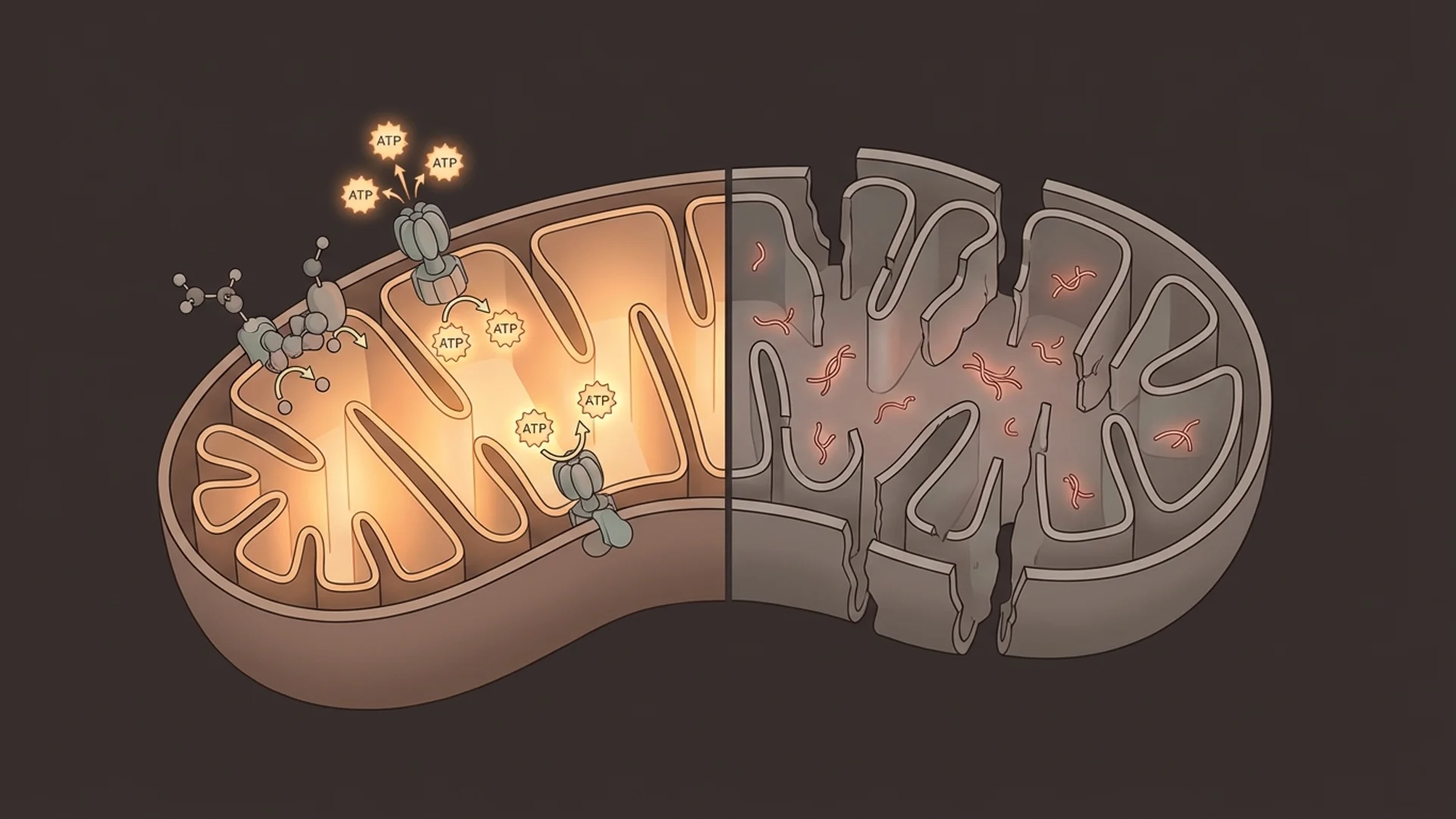
Over a lifetime, mtDNA mutations accumulate. The electron transport chain becomes less efficient. More ROS are produced. A vicious cycle establishes itself: damaged mitochondria produce more oxidative stress, which damages more mitochondria [1].
Additional drivers of mitochondrial decline include:
- NAD+ depletion — NAD+ is required for multiple steps in mitochondrial energy production. Its age-related decline directly impairs mitochondrial function.
- Reduced mitophagy — The selective autophagy of damaged mitochondria (mitophagy) declines with age, allowing dysfunctional organelles to persist.
- Environmental toxins — Heavy metals, pesticides, certain medications (notably statins and some antibiotics), and mold toxins can directly impair mitochondrial function.
- Chronic infection and inflammation — Persistent infections divert cellular resources and generate inflammatory mediators that impair mitochondrial efficiency.
Testing Mitochondrial Function
One of the challenges in mitochondrial medicine is that standard laboratory tests do not assess mitochondrial function directly. In my practice, I use a combination of approaches:
Organic acid testing provides indirect markers of mitochondrial function. Elevated citric acid cycle intermediates, abnormal ratios of specific organic acids, and markers of fatty acid oxidation can suggest mitochondrial impairment.
Lactate and pyruvate ratios offer a crude but clinically useful indicator. Elevated resting lactate or an abnormal lactate-to-pyruvate ratio can suggest impaired oxidative phosphorylation.
CoQ10 levels — Coenzyme Q10 is an essential electron carrier in the mitochondrial transport chain. Low levels correlate with impaired mitochondrial function and are common in patients on statin therapy.
MitoSwab and similar direct assessments — newer tests that assess mitochondrial complex function from buccal swabs are emerging, though validation data is still developing.
Functional assessment — sometimes the most informative approach is clinical. Exercise tolerance testing, perceived energy levels, and response to mitochondrial support therapies provide practical information that laboratory tests may miss.
Treatment: What Improves Mitochondrial Function
Foundational Interventions
Exercise is the most potent stimulus for mitochondrial biogenesis that we know of. Both aerobic exercise and resistance training trigger PGC-1alpha activation and the production of new, healthy mitochondria. High-intensity interval training appears particularly effective [2]. For patients too fatigued to exercise, IHHT offers an alternative pathway to mitochondrial biogenesis without physical exertion.
Sleep is when much of the cellular repair and mitophagy occurs. Chronic sleep deprivation measurably impairs mitochondrial function.
Caloric restriction and time-restricted eating activate AMPK and sirtuins, both of which support mitochondrial quality control.
Targeted Supplementation
Coenzyme Q10 (CoQ10) — Ubiquinol, the reduced form, is essential for electron transport. Doses of 100-300 mg daily have shown benefit in controlled trials for heart failure, statin-associated myopathy, and general fatigue [3]. In patients over 40, particularly those on statins, I consider CoQ10 assessment and supplementation routine.
NAD+ precursors or IV NAD+ — discussed in detail in my NAD+ article.
Alpha-lipoic acid (ALA) — A mitochondrial antioxidant that also supports glutathione recycling. Clinical trial data supports its use in diabetic neuropathy and general antioxidant support. Typical dose: 300-600 mg daily.
Acetyl-L-carnitine — Facilitates fatty acid transport into mitochondria for beta-oxidation. Particularly relevant for patients with fatigue and cognitive complaints. Doses of 500-2,000 mg daily are commonly used.
PQQ (pyrroloquinoline quinone) — Stimulates mitochondrial biogenesis through PGC-1alpha activation. The human data is limited but mechanistically interesting. Typical dose: 10-20 mg daily.
B vitamins — Multiple B vitamins serve as cofactors in mitochondrial energy production. B1 (thiamine), B2 (riboflavin), B3 (niacin/niacinamide), and B5 (pantothenic acid) are all directly involved in the electron transport chain or citric acid cycle.
Magnesium — Required for ATP stabilization (ATP exists in cells as Mg-ATP). Deficiency is common and directly impairs energy production.
Clinical Interventions
IHHT — Intermittent Hypoxia-Hyperoxia Training stimulates mitochondrial turnover through controlled hypoxic stress. See my detailed article.
IV nutrient therapy — In patients with significant mitochondrial dysfunction, IV administration of key nutrients (NAD+, glutathione, B vitamins, magnesium, ALA) can bypass absorption limitations and achieve tissue levels not possible through oral supplementation alone.
Addressing root causes — Identifying and treating underlying contributors to mitochondrial dysfunction — chronic infections, heavy metal exposure, mold toxicity, medication effects — is essential. Supplementing mitochondria while the underlying insult continues is like bailing water without patching the hull.
Clinical Observations
In my practice, mitochondrial support is one of the most consistently rewarding areas of intervention. Patients with documented mitochondrial dysfunction who receive comprehensive treatment — combining lifestyle modification, targeted supplementation, and clinical therapies — frequently report meaningful improvements in energy, cognitive function, and exercise tolerance.
The improvements are not always dramatic or immediate. Mitochondrial repair takes time. I tell patients to expect gradual improvement over weeks to months, not overnight transformation.
What I have also observed is that mitochondrial dysfunction rarely exists in isolation. It typically coexists with hormonal imbalances, nutrient deficiencies, sleep disorders, or chronic infections. Addressing mitochondrial function as part of a comprehensive assessment produces better outcomes than treating it in isolation.
The Bottom Line
Mitochondrial dysfunction is measurable, common, and treatable. It is not simply “getting older.” While we cannot fully reverse age-related mitochondrial decline, we can meaningfully support mitochondrial function through a combination of lifestyle interventions, targeted supplementation, and clinical therapies. For patients experiencing unexplained fatigue, cognitive decline, or exercise intolerance, mitochondrial assessment should be part of the evaluation.
References
- Sun N, Youle RJ, Bhargava P. The Mitochondrial Basis of Aging. Molecular Cell. 2016;61(5):654-666.
- Robinson MM, et al. Enhanced Protein Translation Underlies Improved Metabolic and Physical Adaptations to Different Exercise Training Modes in Young and Old Humans. Cell Metabolism. 2017;25(3):581-592.
- Mortensen SA, et al. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO. JACC Heart Failure. 2014;2(6):641-649.
This content is educational and does not constitute medical advice. Mitochondrial assessment and treatment should be supervised by a qualified physician.