Post-COVID syndrome — also called Long COVID or post-acute sequelae of SARS-CoV-2 (PASC) — affects an estimated 10-30% of people who contract COVID-19. At the time of writing, this represents tens of millions of people worldwide who developed a new chronic illness following a viral infection. Many of them remain without effective treatment.
The condition is real. It is measurable. And for many patients, it is debilitating.
What I find striking about post-COVID — and what differentiates my perspective from many physicians addressing this condition — is how much it resembles the post-infectious syndromes I have been treating for decades. The fatigue, the cognitive dysfunction, the autonomic dysregulation, the reactivation of latent viruses — this is the clinical picture I have seen in chronic Lyme patients, post-EBV patients, and patients with other chronic infectious conditions for years. COVID-19 is a new trigger for a pattern that is not new.
The Mechanisms
Post-COVID is not a single disease. It is a syndrome with multiple contributing mechanisms that vary in their relative importance from patient to patient:

1. Viral Persistence
SARS-CoV-2 RNA and spike protein have been detected in tissues months after acute infection — in the gut, brain, vascular endothelium, and other sites [1]. Whether this represents viable virus or residual antigen is debated, but the clinical implication is the same: persistent viral components drive ongoing immune activation.
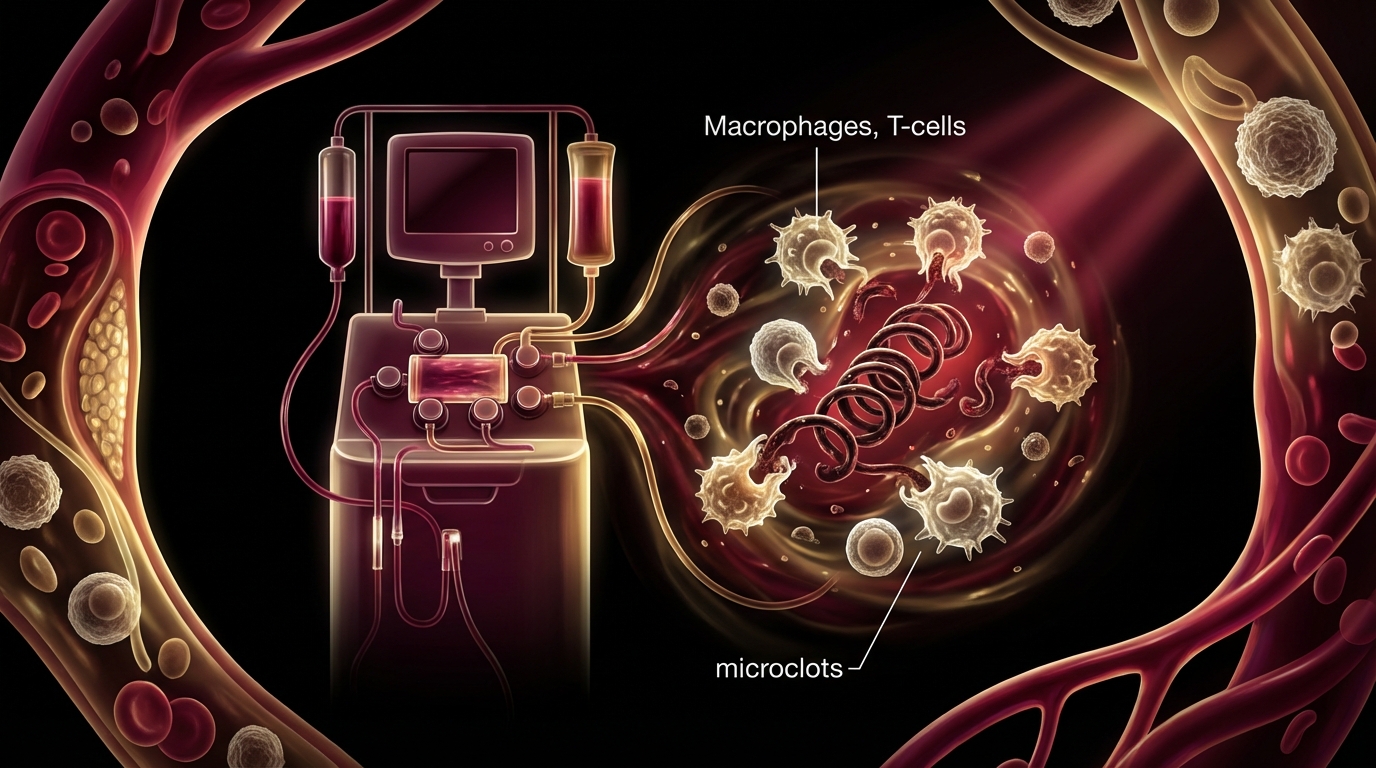
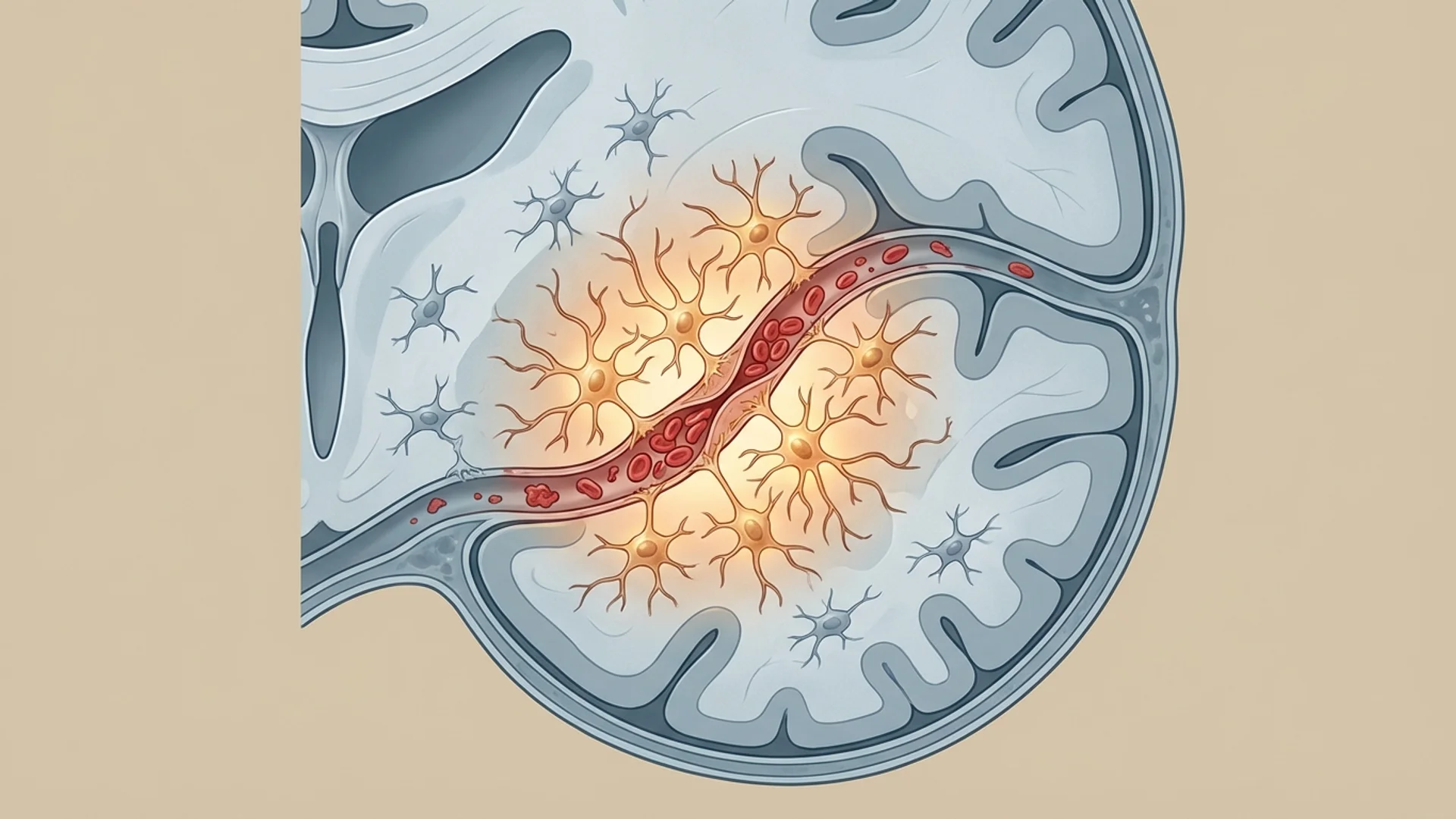
2. Microclots and Endothelial Dysfunction
Dr. Beate Jaeger, who collaborates with our facility, has contributed important research on the role of microclots in post-COVID. Fibrin amyloid microclots — resistant to normal fibrinolysis — trap inflammatory molecules and impair microcirculation. This mechanism explains many post-COVID symptoms, particularly fatigue and cognitive dysfunction. I discuss this in detail in a dedicated article.
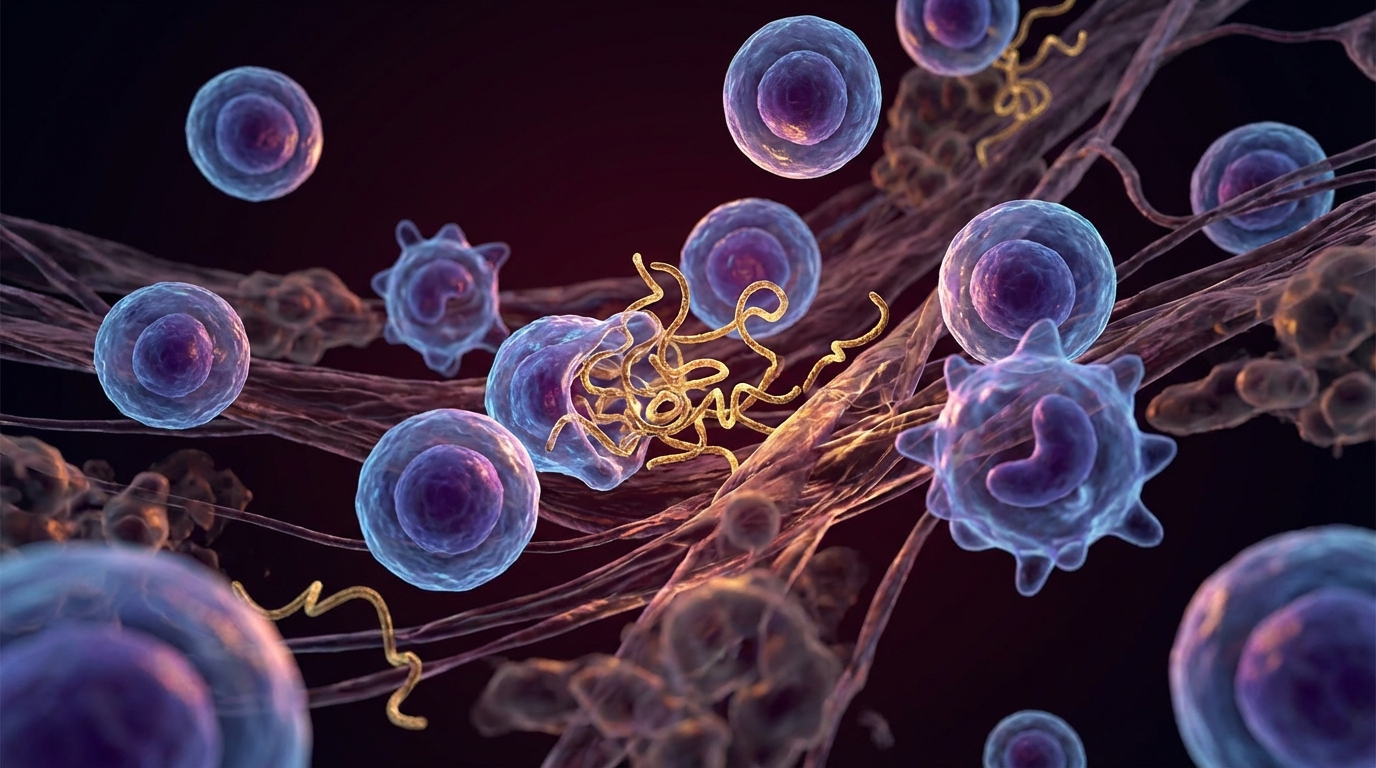
3. Immune Dysregulation
COVID-19 can produce lasting changes in immune function:
- Persistent T cell activation and exhaustion
- Reduced regulatory T cell function
- Elevated inflammatory cytokines (IL-6, TNF-alpha, IFN-gamma) months after infection
- Autoantibody formation (antibodies against the patient’s own tissues)
4. Viral Reactivation
SARS-CoV-2 infection can reactivate latent viruses — particularly EBV, CMV, and HHV-6 — that had been held in check by a competent immune system. In some patients, these reactivated viruses become the primary drivers of ongoing symptoms. See my reactivated viruses article.
5. Autonomic Dysfunction
Dysautonomia — particularly postural orthostatic tachycardia syndrome (POTS) and other forms of autonomic nervous system dysregulation — is common in post-COVID. Patients experience heart rate variability, blood pressure instability, exercise intolerance, and temperature regulation problems.
6. Mitochondrial Dysfunction
The metabolic cost of acute COVID and the ongoing immune activation deplete mitochondrial function. Many post-COVID patients present with the same mitochondrial dysfunction profile I see in chronic fatigue syndrome and chronic infection patients.
Our Diagnostic Approach
When a post-COVID patient presents at our facility, the evaluation is comprehensive:
- Inflammatory markers: hsCRP, IL-6, TNF-alpha, ferritin, D-dimer
- Coagulation assessment: fibrinogen, von Willebrand factor, microclot assessment where available
- Immune function: lymphocyte subsets (T cells, B cells, NK cells), immunoglobulin levels, autoantibody screening
- Viral persistence markers: SARS-CoV-2 spike protein assay, nucleocapsid antibodies
- Reactivated virus panel: EBV (VCA IgG/IgM, EBNA, EA-D), CMV, HHV-6
- Mitochondrial function: organic acid testing, lactate/pyruvate ratios
- Autonomic assessment: tilt-table testing or active standing test, heart rate variability
- Hormonal panel: COVID frequently disrupts thyroid and adrenal function
- Micronutrient status: deficiencies are common after severe illness
Our Treatment Program
Post-COVID treatment at our facility is a multimodal inpatient program, typically spanning two to three weeks. The program is individualized based on the diagnostic findings, but common components include:
Addressing Microclots and Endothelial Dysfunction
- Anticoagulation therapy (carefully titrated based on coagulation assessment)
- Apheresis — therapeutic blood filtration to remove microclots, inflammatory mediators, and autoantibodies. See my apheresis article.
- Endothelial support — targeted nutrients and medications that support vascular healing
Immune Modulation
- IV immunoglobulin therapy in selected cases with demonstrated immune dysfunction
- Low-dose immunotherapy approaches
- Treatment of reactivated viruses when identified
Mitochondrial Rehabilitation
- IV NAD+ therapy
- IHHT (Intermittent Hypoxia-Hyperoxia Training) for mitochondrial biogenesis
- Targeted mitochondrial supplementation (CoQ10, alpha-lipoic acid, B vitamins, magnesium)
- IV nutrient therapy (high-dose vitamin C, glutathione)
Autonomic Support
- Graduated exercise protocols designed for dysautonomic patients
- Hydration and electrolyte optimization
- Pharmacological support where indicated (low-dose beta-blockers, fludrocortisone, or midodrine for POTS)
Detoxification and Anti-Inflammatory Support
- Ozone therapy (as immune modulator and antimicrobial)
- Hepatic support
- Anti-inflammatory supplementation
What I Have Observed
Over the past several years, I have treated hundreds of post-COVID patients. The outcomes vary, but the patterns are consistent:
- Patients whose primary mechanism is microclots and endothelial dysfunction tend to respond well to apheresis and anticoagulation
- Patients with significant viral reactivation improve when the reactivated viruses are addressed
- Patients with predominantly mitochondrial dysfunction respond to NAD+ and IHHT protocols
- Patients with autoimmune features often require longer treatment and may benefit from immunomodulatory therapy
The majority of patients experience meaningful improvement. Complete resolution is possible but not universal. Some patients require ongoing management. The best outcomes occur in patients who are treated comprehensively rather than piecemeal, and who address the specific mechanisms driving their individual presentation.
The Bottom Line
Post-COVID is a post-infectious syndrome with identifiable, measurable mechanisms. It is not psychosomatic. It is not “just anxiety.” It is a condition that responds to targeted treatment when the underlying mechanisms are identified and addressed.
The field is evolving rapidly, and our protocols continue to be refined as new evidence emerges. What I can say with confidence is that a comprehensive, mechanism-based approach produces significantly better outcomes than waiting for spontaneous recovery — which, for many patients, does not come.

References
- Swank Z, et al. Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated With Post-acute Coronavirus Disease 2019 Sequelae. Clinical Infectious Diseases. 2023;76(3):e487-e490.
This content is educational and does not constitute medical advice. Post-COVID syndrome requires individualized medical evaluation and treatment.