At a Glance
| Property | Value |
|---|---|
| Evidence Level | Clinical observation (30+ years institutional experience, 12,000+ Lyme patients) |
| Treatment Duration | 6-8 hours total (sedation, heating, plateau, controlled cooling) |
| Target Temperature | 41.6-41.8 degrees C for Lyme; ~40 degrees C for moderate WBH |
| Common Side Effects | Fatigue, flu-like symptoms, Herxheimer reaction (3-7 days) |
| Serious Side Effects | Rare (<1%) with proper monitoring; burns, cardiac arrhythmia, dehydration |
| Full Recovery | 1-2 weeks typical; progressive improvement over 4-8 weeks |
You Deserve Honest Answers Before Treatment
Patients come to our hospital from over 90 countries, many of them having spent years searching for effective Lyme disease treatment. When they learn about whole-body hyperthermia, the first question is almost always: “What will it actually feel like? What are the side effects?”
I believe you deserve a completely honest answer. Not reassurance without substance. Not scare tactics. Just the facts — what happens during treatment, what to expect afterward, and how to distinguish normal recovery from something that requires attention.
My father began using whole-body hyperthermia at Klinik St. Georg in the 1990s. I have personally overseen thousands of hyperthermia treatments. This is what I know from three decades of institutional experience with over 12,000 Lyme disease patients.
What Happens During Whole-Body Hyperthermia
Let me walk through the procedure step by step, because understanding what happens helps patients prepare psychologically and physically.
Before Treatment
In the days preceding WBH, we conduct thorough pre-treatment assessment:
- Complete blood panel including inflammatory markers, liver and kidney function, electrolytes, and coagulation parameters
- Cardiac evaluation (ECG, and echocardiography if indicated)
- Assessment of current medication and supplement regimen — some medications must be adjusted or paused
- Hydration optimization — we begin IV fluids the evening before or morning of treatment
- Detailed informed consent discussion covering expected effects, risks, and the treatment plan
Patients are asked to fast for 8-12 hours before the procedure. This is standard preparation for any procedure involving sedation.
The Procedure Itself
Sedation: The patient is placed under deep sedation (not general anesthesia) by our anesthesiology team. This is essential for two reasons: first, it allows the patient to tolerate the sustained high temperature comfortably. Second, it eliminates the stress response that would otherwise accompany extreme hyperthermia, which improves both safety and efficacy. The patient is not conscious during the heating phase and has no memory of it.
Monitoring: Continuous monitoring throughout the procedure includes:
- Core body temperature (via esophageal or rectal probe)
- Heart rate and rhythm (continuous ECG)
- Blood pressure
- Oxygen saturation
- Respiratory rate
- IV fluid balance
An anesthesiologist and nursing team are present throughout the entire procedure.
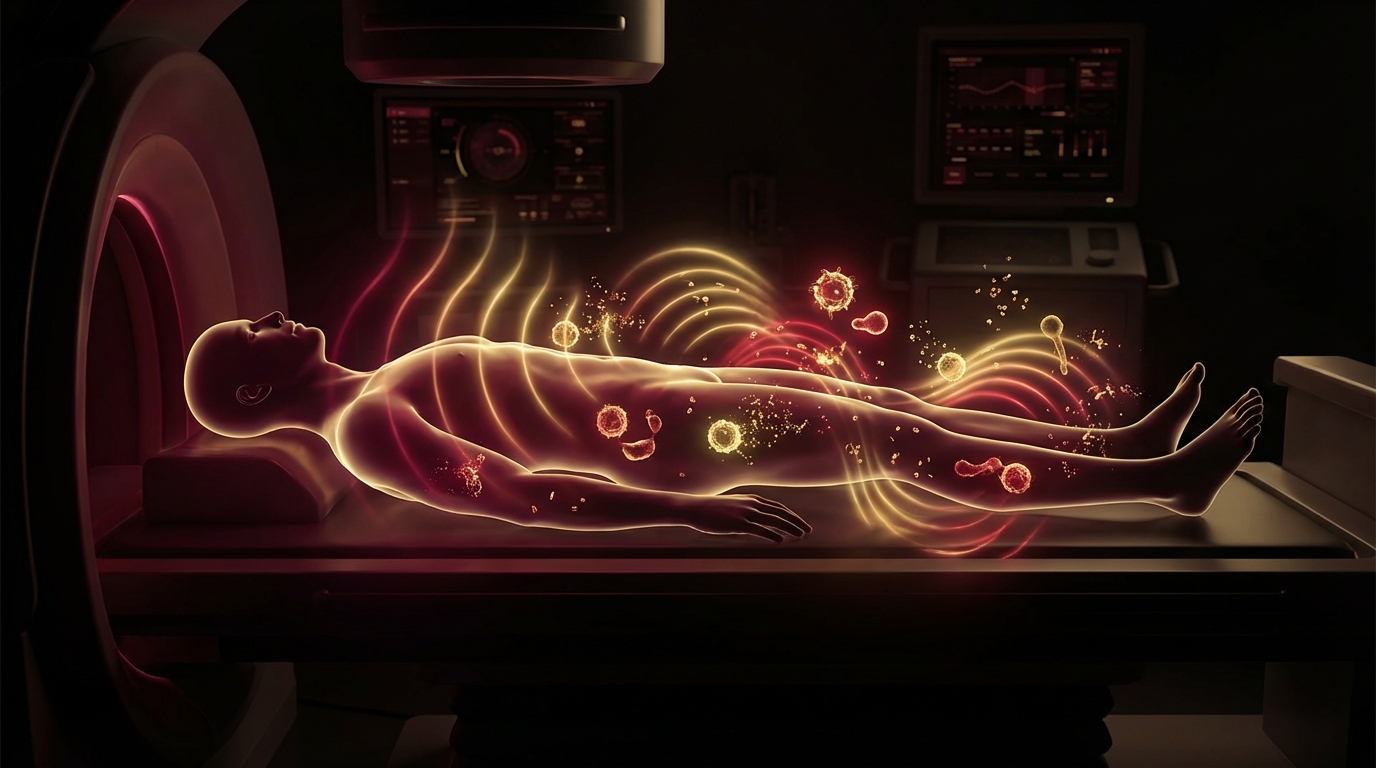
Heating phase: We use the Heckel HT-3000 whole-body hyperthermia device, which uses water-filtered infrared-A radiation to deliver deep, controlled heating. Core temperature rises gradually over approximately 60-90 minutes. The heating rate is carefully controlled — too rapid an increase produces unnecessary cardiovascular stress.
Plateau phase: For extreme WBH targeting Lyme disease, the core temperature is brought to 41.6-41.8 degrees C and maintained at this plateau for approximately 60 minutes. This temperature range is based on the thermolability research of Professor Reisinger at the University of Graz, which demonstrated that Borrelia burgdorferi loses viability at sustained temperatures above 41.5 degrees C [1]. For moderate WBH (used in post-COVID, cancer support, and general immune activation), the target is approximately 40 degrees C for 2-3 hours.
Cooling phase: After the plateau, the body is cooled gradually over 60-90 minutes. Rapid cooling is avoided because it can trigger shivering and cardiovascular stress. The cooling phase is managed with the same precision as the heating phase.
Recovery from sedation: The patient awakens as sedation is tapered. Most patients are awake and oriented within 30-60 minutes of sedation discontinuation, though drowsiness may persist for several hours.
The total time from sedation induction to full awakening is typically 6-8 hours. Patients remain in our hospital for monitoring afterward.
Common Side Effects: What to Expect
I categorize post-WBH effects into three groups: expected normal responses, Herxheimer reactions, and (rarely) complications requiring medical attention.
Expected Normal Responses (Virtually All Patients)
Fatigue: This is the most universal effect. Sustained hyperthermia is a profound physiological stressor — the body has essentially undergone an extreme fever. Expect significant fatigue for 3-5 days following treatment. This is not pathological fatigue. It is the body’s appropriate response to a major immune and metabolic challenge.
What I tell my patients: plan to do nothing for 3-5 days after WBH. No work. No travel. Rest, hydrate, and allow the body to process the treatment. Patients who try to push through recovery invariably feel worse and recover more slowly.
Flu-like symptoms: Muscle aches, headache, mild joint pain, and general malaise are common in the first 24-72 hours. These symptoms mirror what happens during a natural high fever and reflect the inflammatory cascade triggered by hyperthermia. They are self-limiting and respond to standard supportive care (hydration, rest, mild analgesics if needed).
Mild temperature elevation: Low-grade fever (37.5-38.5 degrees C) in the 24-48 hours following WBH is normal. The thermoregulatory system has been challenged, and the immune system is activated. Persistent fever beyond 48 hours should be evaluated.
Appetite changes: Reduced appetite for 1-3 days is common. I encourage patients to eat lightly — broths, soups, easily digestible foods — and prioritize hydration. Appetite typically returns within 3-5 days.
Sleep disturbance: Some patients report disrupted sleep for 2-4 nights following treatment. This may be related to inflammatory mediators, the residual effects of sedation, or the body’s thermal recovery. Sleep quality typically normalizes within a week.
Sweating and thermal dysregulation: Excessive sweating or feeling alternately hot and cold for several days post-treatment is common. The thermoregulatory system needs time to recalibrate after sustained extreme temperatures. Wear light, breathable clothing and maintain a comfortable room temperature.
Skin redness: Mild erythema (skin redness) at areas of direct infrared exposure can occur and typically resolves within 24-48 hours. True thermal burns are rare with modern equipment and experienced operators but must be monitored for.
Herxheimer Reactions: The Die-Off Response
This is the side effect that causes the most anxiety, and it is the one I spend the most time discussing with patients before treatment.
A Herxheimer reaction — named after the early 20th-century dermatologists who first described it — is a temporary worsening of symptoms caused by the release of endotoxins and inflammatory mediators when large numbers of pathogens are killed rapidly [2]. It was first described in syphilis treatment and is well-documented in Lyme disease treatment.
During WBH for Lyme disease, we are intentionally killing Borrelia and co-infection organisms in large numbers by exploiting their thermolability. The resulting release of bacterial debris triggers an inflammatory response that can temporarily intensify symptoms.
What Herxheimer reactions look like after WBH:
- Intensification of existing Lyme symptoms (joint pain, neurological symptoms, fatigue) for 5-14 days
- New symptoms that reflect the body’s inflammatory response to pathogen die-off
- Cognitive fog or temporary worsening of “brain fog”
- Skin reactions (rashes, flushing) in some patients
- Gastrointestinal disturbance (nausea, diarrhea, abdominal discomfort)
- Emotional volatility — some patients experience mood swings or heightened anxiety during the Herxheimer period
The critical message: A Herxheimer reaction is not a complication. It is an expected consequence of effective treatment. I tell my patients: if you have a Herxheimer reaction after WBH, it means the treatment reached the pathogens. The temporary worsening predicts subsequent improvement.
That said, Herxheimer reactions range from mild to severe. Most patients experience moderate symptoms lasting 5-10 days. A subset — perhaps 10-15% in my experience — have more intense reactions lasting up to 2-3 weeks. We monitor all patients through this period and provide supportive care as needed.
Managing Herxheimer reactions:
- Aggressive hydration (3+ liters daily, including electrolyte solutions)
- Rest — the body is processing significant immune activity
- Anti-inflammatory support (we use IV glutathione, IV vitamin C, and oral anti-inflammatory agents)
- Binder therapy (activated charcoal, chlorella, or cholestyramine) to support toxin elimination
- Gentle lymphatic support (dry brushing, light movement when tolerated)
- Close communication with the medical team — we need to distinguish Herxheimer from genuine complications
Rare but Serious Side Effects (<1%)
In our experience with thousands of treatments, serious adverse events are uncommon but must be disclosed:
Cardiac arrhythmia: Sustained hyperthermia increases cardiac workload. Patients with underlying cardiac conditions face elevated risk. This is why we require cardiac assessment before treatment and provide continuous ECG monitoring throughout. Clinically significant arrhythmias are rare in properly screened patients.
Dehydration and electrolyte imbalance: Profuse sweating during WBH can lead to significant fluid and electrolyte losses. This is managed through continuous IV hydration during the procedure and careful post-treatment fluid management. Severe dehydration is preventable with proper protocol adherence.
Thermal injury (burns): First-degree burns at pressure points or areas of direct infrared exposure can occur, particularly in patients with peripheral neuropathy or impaired sensation. Modern equipment and positioning protocols minimize this risk, but it is not zero. We use protective padding and temperature mapping to reduce burn risk.
Prolonged recovery: In a small percentage of patients (approximately 5-10%), recovery takes longer than the typical 1-2 weeks. These patients may experience persistent fatigue or symptom fluctuation for 3-4 weeks. This is more common in patients with high pathogen burden, multiple co-infections, or pre-existing adrenal dysfunction.
Reactivation of dormant infections: WBH activates the immune system broadly. In rare cases, this can lead to reactivation of latent viral infections (herpes simplex, Epstein-Barr virus). This is manageable but needs to be recognized.
The Recovery Timeline
Based on my observation of thousands of patients, here is a realistic recovery trajectory:
Days 1-3: Peak fatigue and flu-like symptoms. This is the lowest point. Most patients rest in our hospital or nearby accommodation during this period.
Days 3-7: Herxheimer reaction typically peaks in this window. Symptoms may intensify before improving. Fatigue remains significant but begins to lift for many patients.
Days 7-14: Progressive improvement. Energy returns gradually. Herxheimer symptoms begin to resolve. Most patients feel well enough to travel home, though I recommend avoiding strenuous activity.
Weeks 2-4: Continued improvement. Many patients report feeling better than they have in months — or years. The immune system has been profoundly stimulated, pathogen burden has been reduced, and the body is rebuilding.
Weeks 4-8: For patients treated for Lyme disease, this is typically when the most meaningful clinical improvements become apparent. Cognitive function, joint pain, fatigue, and neurological symptoms often show their greatest improvement in this window.
Months 2-6: For patients who received the full protocol (typically 2 WBH sessions, combined with antibiotic therapy, apheresis, and immune support), continued gains are common. Serial laboratory assessment helps track objective improvement.
I tell patients: do not judge the success of WBH in the first week. The first week is recovery. The true measure of treatment effect emerges over the following weeks and months.
Contraindications: Who Should Not Receive WBH
Not every patient is a candidate for extreme whole-body hyperthermia. Absolute and relative contraindications include:
Absolute contraindications:
- Severe cardiac insufficiency (NYHA class III-IV heart failure)
- Recent myocardial infarction (within 6 months)
- Unstable angina
- Severe aortic or mitral stenosis
- Acute pulmonary embolism or deep vein thrombosis
- Pregnancy
- Acute cerebrovascular disease
- Uncontrolled seizure disorder
- Severe hepatic or renal failure
Relative contraindications (require case-by-case evaluation):
- Controlled cardiac arrhythmias
- Moderate hepatic or renal impairment
- Poorly controlled diabetes
- Severe peripheral neuropathy (increases burn risk)
- Active autoimmune flare
- Extreme debilitation or very low body weight
- Certain medications that impair thermoregulation
We decline to treat patients who fall outside our safety parameters. No treatment benefit justifies unacceptable risk. In patients with relative contraindications, we may offer moderate WBH (40 degrees C) rather than extreme WBH, as the lower temperature carries a more favorable safety profile.
How Our Approach Differs
I want to address something directly. Not all hyperthermia programs are equal. The safety and efficacy of WBH depends critically on:
The team: Our procedures are performed by experienced physicians with anesthesiology support and trained nursing staff. This is not a spa treatment. It is a medical procedure requiring hospital-level monitoring and emergency preparedness.
The equipment: We use the Heckel HT-3000, a medical-grade whole-body hyperthermia device with precise temperature control. The temperature accuracy and heating homogeneity of the device directly affect both safety and efficacy.
The protocol: Our protocol — 2 sessions at 41.6-41.8 degrees C, based on Reisinger’s thermolability research at the University of Graz — represents three decades of refinement. The target temperature, plateau duration, heating rate, and cooling protocol are all optimized for maximum pathogen kill with acceptable safety margins.
The integration: WBH at our hospital is not a standalone treatment. It is integrated with comprehensive Lyme disease protocols including targeted antimicrobial therapy, apheresis for toxin removal, immune modulation, and nutritional support. The treatment is a component of a program, not a magic bullet.
Patients should ask detailed questions about the qualifications of the treating team, the equipment used, the monitoring protocols, and the institutional experience before undergoing WBH at any facility. In my clinical experience, the difference between a well-run program and a poorly run one is substantial.
The Bottom Line
Whole-body hyperthermia is a medically demanding procedure with predictable, manageable side effects and a favorable safety profile when performed by experienced teams with proper equipment and monitoring. Common effects — fatigue, flu-like symptoms, and Herxheimer reactions — are expected consequences of effective treatment, not complications. Serious adverse events are rare in properly screened and monitored patients.
What I tell my patients before treatment: you will feel worse before you feel better. The first week is recovery, not results. The Herxheimer reaction is a sign the treatment is working. Plan for 1-2 weeks of rest and recovery, be patient with the process, and trust the trajectory. In over 12,000 Lyme patients treated at our hospital, the pattern is consistent: short-term discomfort for long-term improvement.
References
- Reisinger EC, Fritzsche C, Krause R, Krejs GJ. Diarrhea caused by primarily non-gastrointestinal infections. Nat Clin Pract Gastroenterol Hepatol. 2005;2(5):216-222. PMID: 16265183.
- Butler T. The Jarisch-Herxheimer reaction after antibiotic treatment of spirochetal infections: A review of recent cases and our understanding of pathogenesis. Am J Trop Med Hyg. 2017;96(1):46-52. PMID: 28077740.
- Hildebrandt B, Wust P, Ahlers O, et al. The cellular and molecular basis of hyperthermia. Crit Rev Oncol Hematol. 2002;43(1):33-56. PMID: 12098606.
- Issels RD, Lindner LH, Verweij J, et al. Effect of neoadjuvant chemotherapy plus regional hyperthermia on long-term outcomes among patients with localized high-risk soft tissue sarcoma: The EORTC 62961-ESHO 95 randomized clinical trial. JAMA Oncol. 2018;4(4):483-492. PMID: 29450452.
- Wust P, Hildebrandt B, Sreenivasa G, et al. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002;3(8):487-497. PMID: 12147435.