The concept most patients bring to their first appointment is binary: they want to “boost” their immune system. After 20 minutes of conversation, they usually understand why that framing is inadequate.
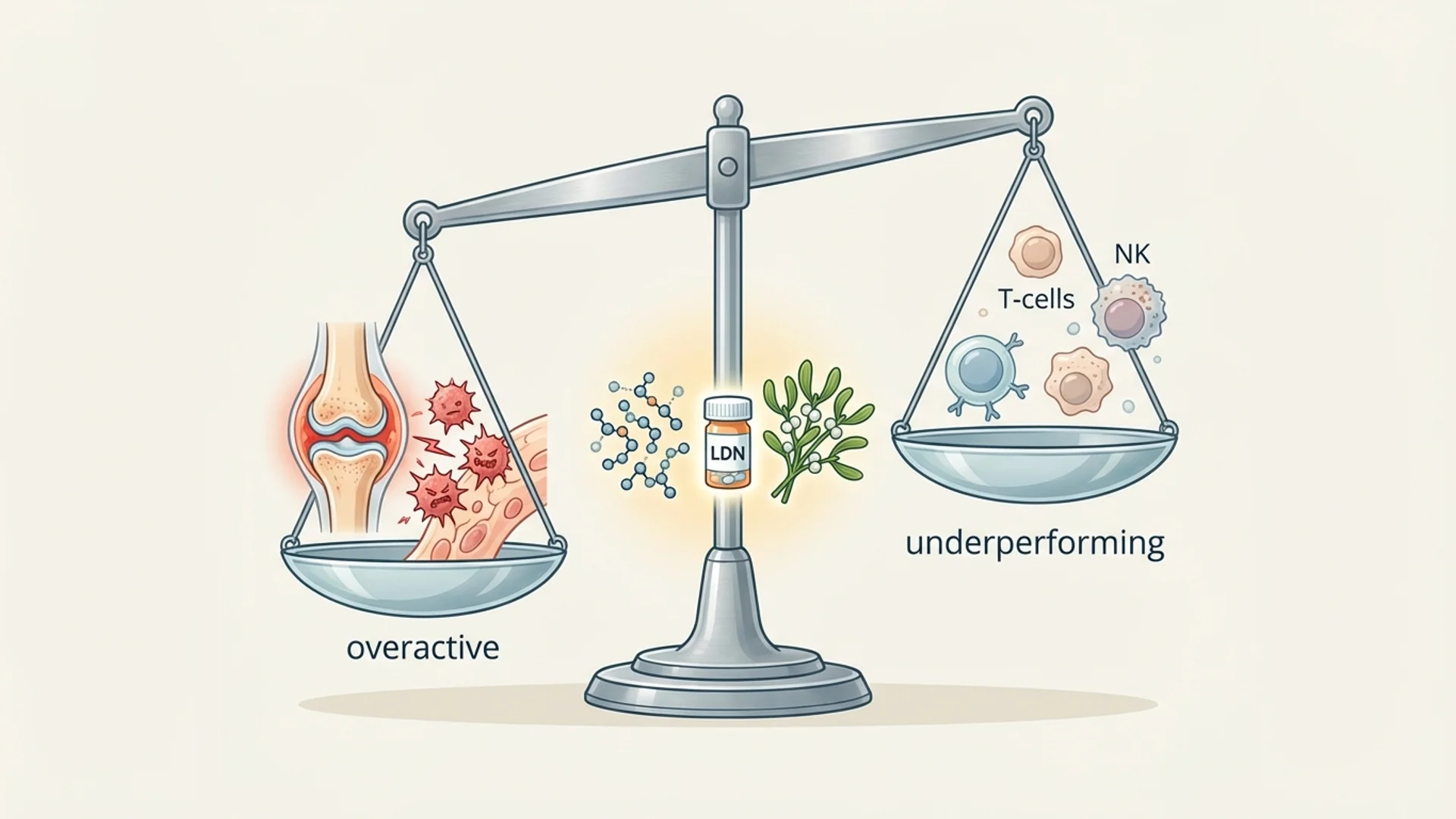
The immune system is not a volume dial that needs turning up. It is a balance. A patient with chronic Lyme disease may have an immune system that is simultaneously over-activated in some pathways (Th1 inflammation, elevated cytokines) and under-performing in others (reduced NK cell activity, exhausted T cells). “Boosting” everything would make some aspects worse.
Immune modulation — the ability to enhance what is underperforming while calming what is overactive — is the clinical goal. It is also considerably more difficult than simple immunostimulation or immunosuppression.
The Difference Between Modulation and Suppression
Conventional immunology has two main levers: stimulate (vaccines, checkpoint inhibitors) and suppress (corticosteroids, biologics, DMARDs). These are powerful tools, and they save lives.
Immune modulation occupies a different conceptual space. Rather than pushing the immune system in one direction, modulators help restore regulatory balance. A true immune modulator can enhance immune function in an immunodeficient patient and calm immune function in an autoimmune patient.
This sounds paradoxical, but it reflects biological reality. Many immune regulatory mechanisms are bidirectional. Regulatory T cells, for example, do not simply suppress — they calibrate. When they function properly, they allow appropriate immune responses while preventing excessive ones.
Evidence-Based Immune Modulators
Low-Dose Naltrexone (LDN)
Naltrexone is an opioid antagonist used at full dose (50 mg) for addiction treatment. At low doses (1.5-4.5 mg, taken at bedtime), it has documented immune-modulating properties through a different mechanism: brief opioid receptor blockade triggers a compensatory upregulation of endorphin production, which in turn modulates immune function through opioid receptors on immune cells.
The evidence base is growing. Randomized controlled trials have been published for Crohn’s disease (Smith et al., showing significant improvement over placebo), multiple sclerosis (Cree et al., demonstrating improved quality of life), and fibromyalgia (Younger et al., showing meaningful symptom reduction). Open-label studies and clinical observation support its use in other autoimmune conditions.
Evidence level: RCTs for specific conditions; clinical observation for broader use. The risk-benefit profile is favorable — side effects are generally limited to vivid dreams and mild sleep disruption during the first one to two weeks.
In my clinical experience, LDN is one of the most consistently useful immune modulators, particularly for patients with autoimmune conditions and chronic pain. Not every patient responds, but those who do often report meaningful improvement within four to eight weeks.
Thymic Peptides
Thymosin alpha-1 (Ta1) is a 28-amino acid peptide that modulates both innate and adaptive immune responses. It enhances dendritic cell maturation, increases NK cell activity, promotes Th1 responses, and supports regulatory T cell function.
Thymosin alpha-1 is approved as a pharmaceutical agent in over 30 countries for hepatitis B and C treatment and as an immune adjuvant. Its use in integrative medicine extends to chronic infections, immune deficiency, and as supportive therapy in oncology.
Evidence level: RCTs for hepatitis B/C and as a vaccine adjuvant; controlled studies for other applications; clinical observation for broader use in integrative practice.
Mistletoe Extract (Viscum album)
Mistletoe therapy is one of the most researched complementary therapies in oncology, with over 150 clinical studies published. It modulates the immune system through multiple mechanisms: enhancing NK cell activity, increasing lymphocyte counts, promoting cytokine release (particularly IL-1, IL-6, and TNF-alpha), and inducing tumor cell apoptosis in vitro.
In Germany, Austria, and Switzerland, mistletoe extract is the most commonly prescribed complementary therapy in oncology. Randomized controlled trials have demonstrated improvements in quality of life, reduction of chemotherapy side effects, and, in some studies, survival benefit — though the survival data remains debated.
Evidence level: RCTs for quality of life and chemotherapy side-effect reduction; moderate evidence for immune modulation; debated evidence for survival benefit.
Intravenous Vitamin C
At pharmacological doses (15-75 g IV), vitamin C acts as a pro-oxidant in the tumor microenvironment while simultaneously supporting immune cell function. It enhances NK cell activity, promotes T cell proliferation, and supports neutrophil function.
Outside oncology, moderate-dose IV vitamin C (7.5-15 g) has anti-inflammatory effects mediated through reduction of NF-kB activation and pro-inflammatory cytokine production. Multiple controlled studies support its use in sepsis (the CITRIS-ALI trial, the Marik protocol), and its application in chronic inflammatory conditions is supported by clinical observation.
Evidence level: RCTs for sepsis and as adjunct in oncology; controlled studies for anti-inflammatory effects; clinical observation for broader use.
Curcumin
Curcumin modulates the immune response through inhibition of NF-kB, COX-2, and multiple pro-inflammatory cytokines (TNF-alpha, IL-1, IL-6). It also enhances Treg function and natural antibody production.
The challenge with curcumin is bioavailability. Standard curcumin supplements have poor oral absorption. Formulations using liposomal delivery, phytosome technology, or piperine co-administration significantly improve absorption.
Evidence level: RCTs for rheumatoid arthritis (comparable to diclofenac in some studies), osteoarthritis, and metabolic syndrome. The evidence base is substantial and growing.
Lifestyle-Based Immune Modulation
Not everything requires a supplement or medication.
Cold exposure — cold water immersion and cold showers have been shown to increase circulating NK cell numbers and activity (Shevchuk, Med Hypotheses 2008; Buijze et al., PLoS ONE 2016 — the latter an RCT showing a 29% reduction in sick days with routine cold showers). The mechanism involves norepinephrine release and subsequent immune cell mobilization.
Heat exposure — sauna use and whole-body hyperthermia activate heat shock proteins that modulate immune responses, increase circulating lymphocytes, and enhance NK cell activity. The Finnish sauna studies (Laukkanen et al.) demonstrate significant all-cause mortality reduction with regular sauna use, with immune modulation as one proposed mechanism.
Exercise — moderate exercise enhances immune surveillance through increased lymphocyte circulation, NK cell activity, and anti-inflammatory cytokine production. The dose matters: moderate exercise is immunomodulatory; excessive exercise without recovery is immunosuppressive.
Sleep — adequate sleep supports regulatory T cell function and maintains the circadian rhythm of cortisol, which is itself a powerful immune modulator. Sleep deprivation shifts the immune system toward pro-inflammatory Th17 responses and away from regulatory Treg function (Besedovsky et al., Pflugers Arch 2012).
The Clinical Decision
Immune modulation is not a protocol; it is a clinical decision that depends on what is wrong. A patient with autoimmune thyroiditis needs a different approach than a patient with chronic Lyme disease, even though both have “immune problems.”
This is why I begin with thorough immune diagnostics — lymphocyte subset panels, NK cell function, cytokine profiles, autoantibody panels — before recommending specific interventions. Treating an immune system without understanding its current state is like adjusting the tuning on an instrument without first listening to what note it is playing.
What I tell my patients: the goal is not to make your immune system stronger or weaker. The goal is to make it smarter — more precisely regulated, more responsive to genuine threats, and less reactive to false ones.
Disclaimer: This article is provided for educational purposes and reflects one physician’s clinical perspective. It is not a substitute for individualized medical care. Immune modulation therapies should be supervised by a qualified physician.