Senescent cell accumulation is one of the most actionable hallmarks of aging. The premise is straightforward: cells that have stopped dividing but resist apoptosis secrete inflammatory factors (the SASP — senescence-associated secretory phenotype) that damage surrounding tissue and accelerate biological aging. Removing these cells improves healthspan in animal models. The question for patients is which senolytic agent to use — and the two flavonoids that dominate this conversation are fisetin and quercetin.
They are both plant-derived polyphenols. They are both available as supplements. And they are frequently discussed as if they are interchangeable. They are not.
At a Glance
| Feature | Fisetin | Quercetin |
|---|---|---|
| Source | Strawberries, apples, persimmons, onions | Onions, apples, capers, berries, tea |
| Senolytic mechanism | PI3K/AKT/mTOR inhibition, Bcl-2 family modulation | Bcl-2/Bcl-xL inhibition (typically combined with dasatinib) |
| Standalone senolytic potency | High (most potent in Kirkland 2018 screen) | Moderate alone; strong with dasatinib |
| Human senolytic trial data | One Phase 2 (AFFIRM-LITE, Mayo Clinic) | Multiple (D+Q: diabetic kidney, IPF, Alzheimer’s) |
| Typical senolytic dose | 20 mg/kg for 2 consecutive days, monthly | 1000 mg quercetin + 100 mg dasatinib for 3 days, monthly |
| Daily supplement use | Common (100-500 mg/day for antioxidant effects) | Common (500-1000 mg/day for antioxidant/anti-histamine) |
| Bioavailability | Low (improved with lipid formulations) | Low (improved with lipid formulations or phytosome) |
| Cost | Moderate ($30-60/month for senolytic cycling) | Low ($15-30/month; dasatinib adds significant cost) |
How Fisetin Works as a Senolytic
Fisetin (3,3’,4’,7-tetrahydroxyflavone) attracted senolytic attention following a landmark 2018 study from the Kirkland laboratory at the Mayo Clinic. In a screen of 10 flavonoids for senolytic activity, fisetin emerged as the most potent at selectively killing senescent cells while sparing normal cells (Yousefzadeh et al., 2018).
Primary senolytic mechanisms:
- PI3K/AKT pathway inhibition: Senescent cells rely on pro-survival signaling through the PI3K/AKT pathway to resist apoptosis. Fisetin inhibits this pathway, removing a key survival signal and allowing senescent cells to undergo programmed cell death.
- mTOR suppression: Fisetin inhibits mTOR signaling, which reduces SASP factor production and impairs the metabolic adaptations that senescent cells use to survive.
- Bcl-2 family modulation: Fisetin shifts the balance of pro-apoptotic (Bax, Bad) versus anti-apoptotic (Bcl-2, Bcl-xL) proteins toward cell death in senescent cells specifically. This selectivity is what makes it a senolytic rather than a general cytotoxic agent.
- SASP suppression: Beyond killing senescent cells, fisetin reduces the inflammatory output of those that remain — it functions as both a senolytic (kills senescent cells) and a senomorphic (modifies senescent cell behavior).
The preclinical evidence:
The Yousefzadeh 2018 study demonstrated that fisetin treatment in aged mice reduced senescent cell markers in multiple tissues, reduced age-related pathology, and extended median and maximum lifespan. Treated mice showed reduced tissue inflammation, improved organ function, and extended healthspan even when treatment began in old age (equivalent to approximately 75 human years).
A subsequent study showed that fisetin reduced senescence-associated markers in human adipose tissue explants, providing an ex vivo bridge between mouse models and human application (Kirkland et al., subsequent publications).
Human trial status:
The AFFIRM-LITE trial at the Mayo Clinic evaluated fisetin in older adults with frailty. Results indicated that intermittent fisetin dosing (20 mg/kg for 2 consecutive days, repeated monthly) was well-tolerated, with preliminary signals of reduced inflammatory markers. The data is early-stage and not yet definitive for clinical efficacy, but the safety profile was favorable.
Additional trials are ongoing for fisetin in osteoarthritis, COVID-19 recovery, and age-related frailty.
How Quercetin Works as a Senolytic
Quercetin (3,3’,4’,5,7-pentahydroxyflavone) is the more familiar flavonoid — it has been studied for decades as an antioxidant, anti-inflammatory, and antihistamine. Its senolytic application came through the pioneering work of James Kirkland and Tamara Tchkonia at the Mayo Clinic, who identified that quercetin combined with dasatinib (a tyrosine kinase inhibitor used in leukemia treatment) produced potent senolytic effects.
Why quercetin alone is insufficient:
Quercetin has moderate senolytic activity on its own — it inhibits Bcl-xL, one of the anti-apoptotic proteins that senescent cells use to resist death. However, senescent cells have multiple redundant survival pathways. Quercetin alone does not adequately suppress all of them, which is why its senolytic effect as a single agent is inconsistent across cell types.
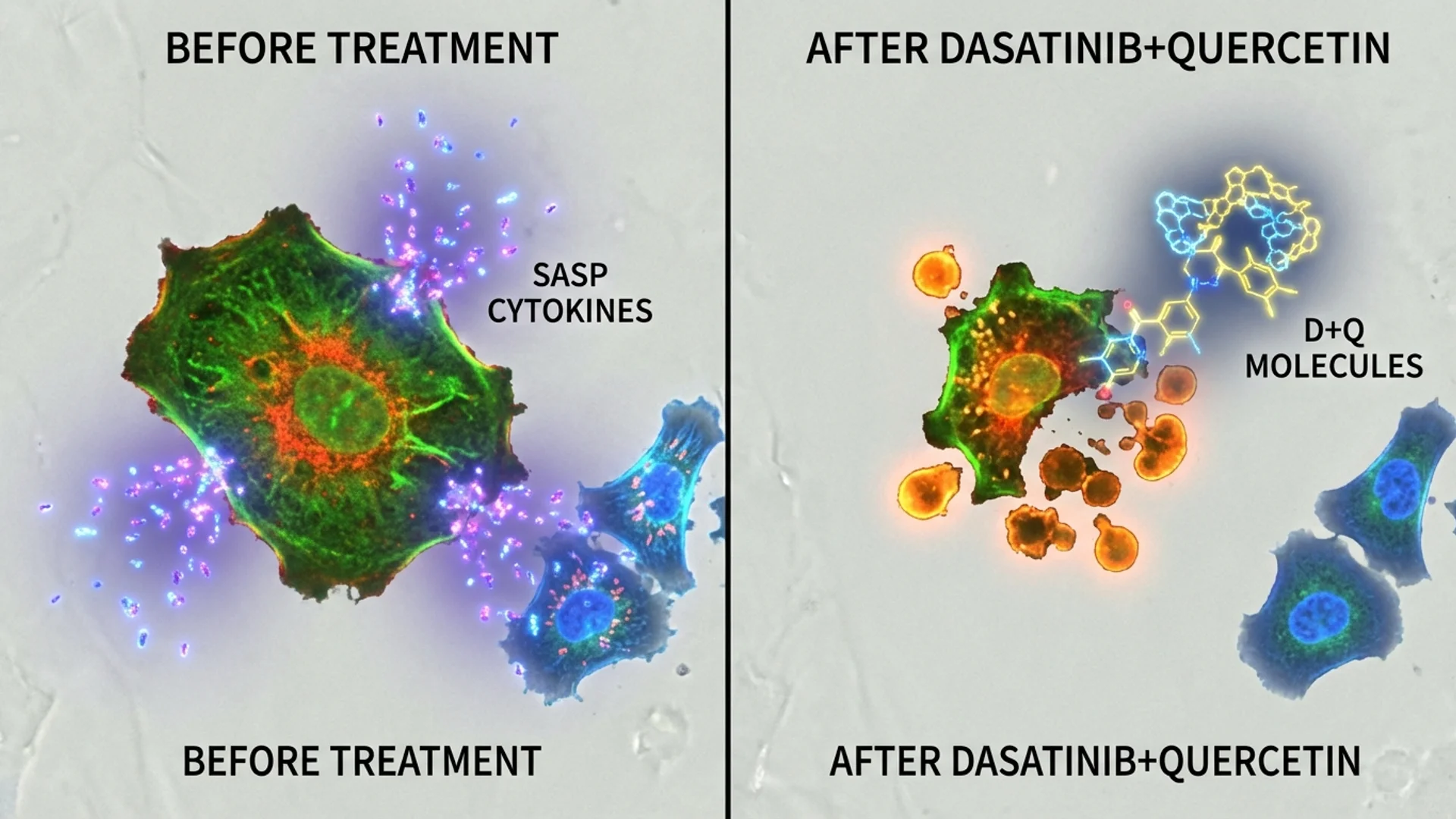
The dasatinib plus quercetin (D+Q) combination:
Dasatinib inhibits a different set of senescent cell survival pathways — primarily SRC family kinases, ephrin receptors, and multiple tyrosine kinases. The combination of dasatinib and quercetin targets complementary survival networks:
- Dasatinib: Blocks SRC kinases, ephrin B receptors, and PAK signaling (more effective against senescent preadipocytes and endothelial cells)
- Quercetin: Blocks Bcl-xL, PI3K, and serpine pathways (more effective against senescent bone marrow stem cells and some epithelial cells)
- Together: The combination achieves broad-spectrum senolytic activity across multiple cell types that neither agent achieves alone (Zhu et al., 2015).
Human trial data (D+Q combination):
The D+Q combination has the most published human senolytic data:
- Diabetic kidney disease (Hickson et al., 2019): First-in-human senolytic trial. Three days of D+Q reduced senescent cell burden in adipose tissue and skin, reduced circulating SASP factors, all within 11 days.
- Idiopathic pulmonary fibrosis (Justice et al., 2019): D+Q improved physical function (6-minute walk distance, chair stands, gait speed) in patients with this senescence-associated lung disease.
- Alzheimer’s disease (pilot data): Ongoing trials at multiple centers examining D+Q for CNS senescent cell clearance.
Quercetin as a daily supplement:
Outside of senolytic protocols, quercetin is widely used at 500-1000 mg/day for its anti-inflammatory, antihistamine, and antioxidant properties. At these daily doses, quercetin functions as a senomorphic agent (reducing SASP) rather than a senolytic (killing senescent cells). The senolytic effect requires intermittent high-dose protocols, not chronic daily supplementation.
Head-to-Head Comparison
| Parameter | Fisetin (standalone) | Quercetin + Dasatinib (D+Q) |
|---|---|---|
| Senolytic potency (preclinical) | Highest single-agent flavonoid | Higher (combination synergy) |
| Spectrum of cell types cleared | Broad (multiple senescent cell types) | Broadest (complementary targeting) |
| Published human senolytic trials | 1 (AFFIRM-LITE, preliminary) | 3+ (DKD, IPF, ongoing) |
| Lifespan extension in mice | Yes (Yousefzadeh 2018) | Yes (multiple studies) |
| Requires prescription component | No (fisetin is OTC) | Yes (dasatinib is Rx only) |
| SASP suppression | Strong (dual senolytic + senomorphic) | Strong |
| Safety profile | Favorable (supplement-grade) | Dasatinib carries hematologic monitoring requirements |
| Accessibility | High (available as supplement) | Lower (requires physician for dasatinib) |
| Typical protocol | 20 mg/kg x 2 days, monthly | D 100mg + Q 1000mg x 3 days, monthly |
| Cost per cycle | $5-15 | $50-300+ (dasatinib cost varies widely) |
| Bioavailability concern | Significant (lipophilic, poor water solubility) | Significant (both agents; formulation matters) |
When I Recommend Fisetin
Fisetin is my preference in the following scenarios:
- Patients seeking an accessible senolytic protocol without prescription medications — fisetin can be purchased as a supplement, making it accessible to patients who want to begin senolytic cycling without requiring a dasatinib prescription.
- Patients who cannot tolerate dasatinib — dasatinib carries potential for cytopenias (low blood counts), pleural effusions, and hepatic effects. For patients with borderline hematologic parameters or liver function, fisetin offers a senolytic option without these risks.
- First-line senolytic trial — for patients new to senolytics, I often start with fisetin because the risk profile is lower. If fisetin cycling produces measurable results (reduced inflammatory markers, improved function), it may be sufficient. If not, escalation to D+Q is the next step.
- Combined senolytic and senomorphic goals — fisetin’s dual activity makes it attractive for patients who want both acute senescent cell clearance (intermittent high-dose) and ongoing SASP suppression (lower daily doses between cycles).
What I tell my patients: fisetin is the most convenient entry point into senolytic therapy. The preclinical data is compelling — it was the most potent single-agent senolytic in the Mayo Clinic screen. The human data is still early, but the safety profile makes it a reasonable option for motivated patients.
When I Recommend Quercetin (as Part of D+Q)
The dasatinib plus quercetin combination is my recommendation when:
- Maximum senolytic effect is the goal — D+Q has the broadest senolytic spectrum and the most published human data. For patients with significant senescent cell burden (advanced biological age, chronic inflammatory conditions, fibrotic diseases), D+Q offers the strongest evidence-based approach.
- Specific conditions with D+Q data — idiopathic pulmonary fibrosis, diabetic kidney disease, and other conditions where human senolytic trial data exists.
- Patients who did not respond adequately to fisetin cycling — if 3-4 months of monthly fisetin cycling has not produced measurable improvement in inflammatory markers or functional outcomes, escalation to D+Q is appropriate.
- Under physician supervision with monitoring — D+Q requires baseline and periodic monitoring of complete blood count, liver function, and chest imaging (dasatinib-specific). This is a physician-supervised protocol, which I consider a feature rather than a limitation.
Here is what the evidence shows: the D+Q combination has more human clinical data supporting its senolytic efficacy than any other approach. The trade-off is the added complexity and risk of dasatinib, which is a chemotherapy-class drug being repurposed at lower doses.
Can You Combine Them?
This question comes up frequently, and the answer requires nuance.
Fisetin + quercetin (without dasatinib): Both are flavonoids that inhibit partially overlapping pathways. Combining them may modestly enhance senolytic coverage, but the incremental benefit over fisetin alone is uncertain. There is no published data on this specific combination as a senolytic protocol. Some practitioners use both, but this is empirical rather than evidence-based.
Fisetin + D+Q: This combination is more interesting theoretically — fisetin’s PI3K/AKT/mTOR inhibition complements D+Q’s targeting of SRC kinases and Bcl-xL. However, adding a third senolytic agent increases the concern about off-target effects on healthy cells. There is no published data on this triple combination, and I do not routinely use it.
My practical approach:
In my clinical experience, the most reasonable protocol is to choose one senolytic approach and execute it well:
- Fisetin protocol: 20 mg/kg body weight (typically 1400-2000 mg for an adult) for 2 consecutive days, once monthly. Use a liposomal or lipid-based formulation for improved bioavailability. Cycle for 3-6 months, then assess.
- D+Q protocol: Dasatinib 100 mg + quercetin 1000 mg for 3 consecutive days, once monthly. Baseline labs before starting, repeat labs at 3 months. Cycle for 3-6 months, then assess.
Between senolytic cycles, daily quercetin (500 mg) or fisetin (100-200 mg) at lower doses can provide senomorphic SASP-suppressing effects without the intermittent senolytic hit.
Clinical Perspective — Julian Douwes M.D.
Senolytics represent one of the most promising intervention points in longevity medicine — the concept of removing dysfunctional cells that poison their neighbors is elegant and well-supported in animal models. The challenge is that we are still in early-stage human translation. Fisetin gives patients an accessible, low-risk entry point with strong preclinical backing. D+Q offers stronger human data but requires physician involvement and monitoring. What I always emphasize to patients is that senolytics are intermittent interventions, not daily supplements. The “hit and run” dosing strategy — high dose for 2-3 days, then stop — is essential because you want to create a brief pro-apoptotic window for senescent cells while minimizing prolonged exposure that might affect healthy cells. Patients who take senolytic doses daily are doing it wrong, and they may be increasing rather than decreasing their risk.
Key Takeaways
- Fisetin was identified as the most potent single-agent senolytic flavonoid in the landmark 2018 Mayo Clinic screening study.
- Quercetin is typically used in combination with dasatinib (D+Q), which has the most published human senolytic trial data.
- Fisetin has dual senolytic and senomorphic activity; quercetin alone has moderate senolytic activity that is dramatically enhanced by dasatinib.
- For accessible, low-risk senolytic cycling, fisetin is the practical choice. For maximum evidence-based senolytic effect, D+Q leads.
- Both flavonoids have significant bioavailability limitations — lipid-based or liposomal formulations are recommended.
- Senolytic protocols are intermittent (2-3 days per month), not daily. Daily dosing at senolytic levels is not appropriate.
- Human evidence for senolytics is still early-stage. Animal data is compelling, but definitive human aging outcomes have not yet been demonstrated in large trials.
References
- Yousefzadeh, M.J., et al. “Fisetin is a senotherapeutic that extends health and lifespan.” EBioMedicine, 36, 2018, pp. 18-28.
- Zhu, Y., et al. “The Achilles’ heel of senescent cells: from transcriptome to senolytic drugs.” Aging Cell, 14(4), 2015, pp. 644-658.
- Hickson, L.J., et al. “Senolytics decrease senescent cells in humans: preliminary report from a clinical trial of dasatinib plus quercetin in individuals with diabetic kidney disease.” EBioMedicine, 47, 2019, pp. 446-456.
- Justice, J.N., et al. “Senolytics in idiopathic pulmonary fibrosis: results from a first-in-human, open-label, pilot study.” EBioMedicine, 40, 2019, pp. 554-563.
- Kirkland, J.L., and Tchkonia, T. “Senolytic drugs: from discovery to translation.” Journal of Internal Medicine, 288(5), 2020, pp. 518-536.