The gastrointestinal tract is not merely a digestive organ. It is the largest immune organ in the body, the primary interface between your internal environment and the outside world, and the seat of a microbial ecosystem that influences everything from mood to metabolic health. When gut function is compromised, the effects ripple outward into virtually every system.
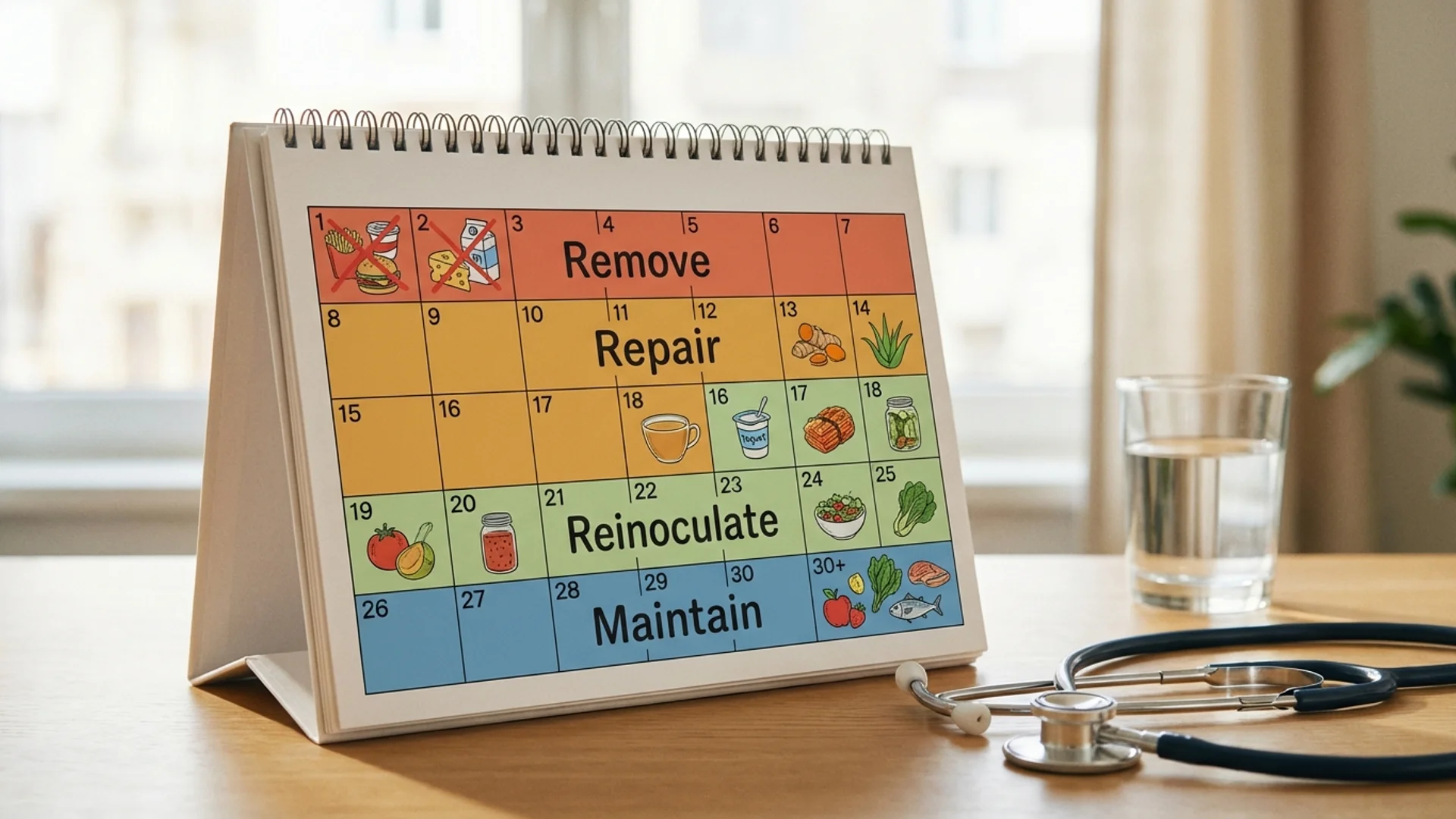
This protocol represents a structured approach to gut restoration that I have refined over years of clinical practice. It is organized into four sequential phases, each building on the one before. The underlying logic is straightforward: before you can rebuild, you must first address what is causing damage; before you can reinoculate, you must first repair the terrain.
A word of clinical honesty before we begin: gut restoration is not a 30-day project. Thirty days is enough to initiate meaningful change, to reduce acute inflammation, to begin restoring barrier function. But complete restoration of a damaged gut ecosystem — particularly after years of antibiotics, processed food, chronic stress, or infection — often requires months of sustained effort. This protocol is a beginning, not a finish line.
Phase 1: Remove (Days 1-7)
The first phase focuses on removing the factors that are actively damaging the gut lining and disrupting the microbiome.
Dietary Eliminations
Remove the following for the full 30 days (not just this phase):
- Refined sugar and artificial sweeteners. Refined sugar feeds pathogenic organisms and disrupts microbial balance. Artificial sweeteners (sucralose, aspartame, saccharin) have been shown in human studies to alter gut microbiome composition and impair glucose tolerance. Evidence level: controlled human studies (Suez et al., Nature 2014).
- Gluten-containing grains. Gluten increases intestinal permeability via zonulin release in susceptible individuals. This is not limited to celiac disease — zonulin upregulation has been documented in non-celiac populations. Evidence level: controlled human studies (Fasano, Physiol Rev 2011). Even if you do not have celiac disease, a 30-day elimination allows you to assess whether gluten is contributing to your symptoms.
- Conventional dairy. Casein A1 (the predominant casein in conventional cow’s milk) generates beta-casomorphin-7 during digestion, which appears to promote intestinal inflammation in some individuals. Evidence level: controlled human studies with individual variation. Clarified butter (ghee) is typically tolerated and may be continued.
- Processed seed oils. Soybean oil, canola oil, sunflower oil, and corn oil are high in omega-6 fatty acids and oxidized lipid products that promote intestinal inflammation. Replace with olive oil, avocado oil, and coconut oil.
- Alcohol. Alcohol directly damages the intestinal epithelium and disrupts tight junction integrity. Even moderate consumption impairs gut barrier function. Evidence level: robust human data.
Address Active Infections or Overgrowth
If there is clinical suspicion or laboratory evidence of:
- Small intestinal bacterial overgrowth (SIBO): This should be addressed with targeted antimicrobials (herbal or pharmaceutical, depending on clinical context) before proceeding to later phases. Reinoculating a gut that has active bacterial overgrowth is counterproductive.
- Fungal overgrowth (Candida or other): Similarly, address with appropriate antifungals. Biofilm-disrupting agents may be necessary for persistent cases.
- Parasitic infection: Stool testing with PCR-based methods (GI-MAP or equivalent) can identify parasitic infections that conventional stool testing misses.
This is where the protocol becomes individual rather than generic. The appropriate treatment for gut infections depends on what is found, and treatment should be guided by a physician with experience in functional gastroenterology. What I tell my patients: the “remove” phase is the most important phase to get right, and it is the phase most likely to benefit from professional guidance.
Supportive Supplements (Phase 1)
Supplement Dose Evidence Level Purpose
Berberine 500 mg twice daily with meals Strong (RCTs) Antimicrobial, blood sugar regulation
Oregano oil (emulsified) 200 mg twice daily Emerging (preclinical + clinical observation) Broad-spectrum antimicrobial
Activated charcoal 500 mg at bedtime (away from other supplements) Moderate (mechanistic data) Toxin binding during die-off
Phase 2: Repair (Days 8-17)
With active irritants and infections being addressed, the second phase focuses on repairing the intestinal lining itself.
Gut Lining Repair Supplements
Supplement Dose Evidence Level Purpose
Zinc carnosine 75 mg twice daily Strong (RCTs, notably Mahmood et al.) Enhances mucosal repair, reduces NSAID-induced permeability
DGL (deglycyrrhizinated licorice) 400 mg before meals Moderate (controlled studies) Stimulates mucus production, protects epithelium
Collagen peptides 10-15 g daily Moderate (controlled studies + mechanistic) Provides amino acid substrates for intestinal connective tissue
Butyrate (as tributyrin) 300-600 mg twice daily Strong (RCTs) Primary fuel for colonocytes; strengthens barrier function
On L-Glutamine
L-glutamine deserves particular discussion. It is the most abundant amino acid in the bloodstream and the preferred fuel source for intestinal epithelial cells (enterocytes). During periods of physiological stress — infection, inflammation, intense exercise — glutamine demand exceeds supply, and the gut lining suffers.
Multiple randomized controlled trials have demonstrated that glutamine supplementation reduces intestinal permeability and supports mucosal repair. A notable study by Zhou et al. showed that glutamine supplementation significantly reduced intestinal permeability in critically ill patients. The evidence for glutamine in gut repair is among the strongest in the functional medicine supplement arsenal. This is not a speculative recommendation — it is supported by Level 1 evidence.
On Butyrate
Butyrate is a short-chain fatty acid produced by beneficial gut bacteria through the fermentation of dietary fiber. It is the primary energy source for colonocytes (the cells lining the colon) and plays a critical role in maintaining barrier function, modulating inflammation, and regulating gene expression in the gut epithelium.
In a healthy gut, sufficient butyrate is produced endogenously by bacteria such as Faecalibacterium prausnitzii and Roseburia. In a compromised gut — where these beneficial species may be depleted — supplemental butyrate can bridge the gap while the microbiome is being restored. Tributyrin is the preferred supplemental form because it survives gastric acid and delivers butyrate to the small and large intestine.
Dietary Additions (Phase 2)
- Bone broth (homemade or from a trusted source): rich in glycine, proline, and gelatin, which provide substrates for intestinal connective tissue repair
- Cooked vegetables (emphasize low-FODMAP initially if SIBO is a concern): beets, carrots, zucchini, sweet potato
- Omega-3 fatty acids (wild-caught fatty fish, or supplemental EPA/DHA at 2-3 g daily): anti-inflammatory effects on intestinal mucosa are supported by controlled human studies
Phase 3: Reinoculate (Days 18-25)
With active infections addressed and the gut lining under repair, the third phase introduces beneficial organisms and the substrates they need to establish themselves.
Probiotic Strategy
The evidence for probiotic supplementation is strain-specific. Not all probiotics are equivalent, and the marketing around probiotics frequently overstates what the research supports. Here is what the evidence shows for specific strains and conditions:
Strain/Product Evidence Level Best Supported For
Saccharomyces boulardii Strong (RCTs) C. difficile prevention, traveler’s diarrhea, IBD adjunct
VSL#3 / Visbiome Strong (RCTs) Ulcerative colitis maintenance, pouchitis
Bifidobacterium infantis 35624 (Align) Strong (RCTs) IBS symptom reduction
Lactobacillus plantarum 299v Strong (RCTs) IBS symptom reduction, iron absorption
My recommendation: Use a multi-strain probiotic that includes at least Lactobacillus and Bifidobacterium species, at a dose of 50-100 billion CFU daily. Take on an empty stomach (first thing in the morning or at bedtime). Continue for at least 90 days.
In addition to supplemental probiotics, incorporate fermented foods daily:
- Sauerkraut (unpasteurized, from the refrigerated section)
- Kimchi
- Kefir (goat or coconut if avoiding dairy)
- Kombucha (low-sugar varieties)
Start slowly with fermented foods. If you experience significant bloating or gas when introducing them, this may indicate residual SIBO or dysbiosis that needs further attention.
Prebiotic Strategy
Prebiotics are the substrates that feed beneficial gut bacteria. The goal is to provide the specific types of fiber that your beneficial organisms need to thrive.
Prebiotic Dose Feeds Evidence Level
Acacia fiber 5-10 g daily Bifidobacteria, Lactobacillus Moderate (controlled studies)
GOS (galactooligosaccharides) 5 g daily Bifidobacteria Strong (RCTs)
Resistant starch (cooked and cooled potato, green banana flour) 10-20 g daily from food Butyrate producers Strong (RCTs)
Important: Introduce prebiotics gradually. Starting with full doses can cause significant bloating and gas as your microbiome adjusts. Begin with half doses and increase over 7-10 days.
Phase 4: Maintain (Days 26-30 and Beyond)
The final phase is about transitioning from an acute intervention protocol to a sustainable long-term approach.
Dietary Reintroduction
Beginning on day 26, you may systematically reintroduce eliminated foods one at a time, with 72 hours between each reintroduction. This spacing allows you to identify delayed sensitivity reactions that would be missed with faster reintroduction.
Reintroduction order (one new food every 3 days):
- Clarified butter/ghee (if not already included)
- Organic, grass-fed butter
- Fermented dairy (yogurt, kefir)
- Eggs
- Non-gluten grains (rice, oats, quinoa)
- Gluten-containing grains (save for last)
For each reintroduction: eat a normal serving of the food on day 1, then observe for 72 hours. Track energy, digestion, bowel habits, joint symptoms, skin, and mood. If symptoms appear, remove that food and wait until symptoms resolve before proceeding with the next reintroduction.
What I tell my patients: the reintroduction phase is diagnostic. It tells you which foods your body tolerates well and which it does not. Some patients discover that gluten or dairy are significant symptom triggers. Others find they tolerate everything without issue. Either outcome is valuable information.
Long-Term Maintenance
- Continue probiotics for at least 90 days total, then reassess. Some patients benefit from ongoing low-dose probiotic supplementation; others maintain microbial diversity through diet alone.
- Maintain prebiotic fiber intake through a diverse, whole-food diet. Aim for 30+ different plant foods per week (the “30-plant challenge” is supported by data from the American Gut Project showing that microbial diversity correlates with plant food diversity).
- Continue glutamine at 5 g daily if you have a history of gut issues, high stress, or intense exercise.
- Periodic butyrate supplementation during periods of stress, travel, or dietary disruption.
Lifestyle Factors
Gut health is not purely a supplement and diet issue. The following factors have documented effects on gut barrier function and microbiome composition:
- Sleep: Sleep deprivation increases intestinal permeability within 48 hours (human data). Prioritize 7-9 hours of quality sleep.
- Stress management: Chronic psychological stress activates the HPA axis, increases cortisol, and directly impairs gut barrier function. The mechanism is well-characterized and the evidence is Level 1. Find a stress management practice that you will actually do consistently.
- Exercise: Moderate exercise improves microbial diversity (human data from Clark et al., Gut 2014). Excessive exercise without adequate recovery can temporarily impair barrier function.
- Meal timing: Allow 12-14 hours overnight without food. This fasting window supports the migrating motor complex (MMC), which is the gut’s self-cleaning mechanism and is impaired by constant snacking.
When to Seek Medical Help
This protocol is designed as a general framework. Certain situations require professional medical evaluation rather than self-guided protocols:
- Blood in stool — always requires evaluation to rule out inflammatory bowel disease, colorectal pathology, or infection
- Unintentional weight loss accompanying GI symptoms
- Symptoms that worsen during the protocol rather than improving
- History of inflammatory bowel disease (Crohn’s disease, ulcerative colitis) — these conditions require medical management, and supplement protocols should complement, not replace, conventional treatment
- Suspected SIBO or fungal overgrowth — accurate diagnosis requires testing, and treatment should be guided by results
- Persistent symptoms after completing the protocol — this suggests an underlying issue that the protocol has not addressed, and further investigation is warranted
Clinical Perspective
I designed this protocol based on years of treating patients with complex gut dysfunction, many of whom come to Klinik St. Georg after conventional gastroenterology has not resolved their symptoms. Here is what that experience has taught me:
The most important intervention is usually the simplest. Removing processed food, refined sugar, and alcohol from the diet for 30 days produces more consistent improvement than any single supplement. I include supplements in this protocol because they can accelerate the process, but the dietary changes are the foundation.
Testing before treating produces better outcomes. A comprehensive stool analysis (GI-MAP or equivalent) performed before starting the protocol helps identify specific infections, imbalances, or markers of inflammation that can be targeted. Treating blindly works sometimes. Treating with data works more often.
Patience matters more than perfection. Gut restoration is not linear. There will be days during this protocol when you feel worse than when you started — particularly during the “remove” phase if significant die-off reactions occur. This is expected and temporary. The patients who succeed are the ones who stay the course, not the ones who execute the protocol perfectly.
The gut is connected to everything. Many of my patients come seeking treatment for fatigue, brain fog, joint pain, or skin conditions — and their symptoms resolve or significantly improve when we address their gut function. This is not surprising given the gut’s role in immune regulation, nutrient absorption, and systemic inflammation. But it means that a gut protocol can have benefits that extend well beyond digestive comfort.
Disclaimer: This protocol is provided for educational purposes and reflects one physician’s clinical approach. It is not a substitute for individualized medical care. Consult a qualified physician before beginning any new supplement protocol, particularly if you have existing medical conditions or are taking medications. Some supplements may interact with pharmaceutical medications.