Key Takeaways:
- Peptide legality is not a yes-or-no question — it depends on the specific peptide, the jurisdiction, and the intended use
- The FDA’s 2023-2025 Category 2 decisions removed several popular peptides from compounding pharmacy availability in the United States
- In Germany and much of the EU, physician-directed prescribing frameworks provide significantly broader access to therapeutic peptides
- Australia’s TGA has taken a middle path, scheduling some peptides as prescription-only rather than banning them outright
- Purchasing peptides as “research chemicals” is a legal grey zone with genuine safety and legal risks that patients underestimate
At a Glance
| Property | Value |
|---|---|
| Regulatory Complexity | High — varies by peptide, country, and use case |
| US Status (2026) | Multiple peptides restricted from compounding; thymosin alpha-1 and others remain in legal dispute |
| EU/Germany Status | Broader physician prescribing latitude under national frameworks |
| Australia Status | Several peptides moved to prescription-only (Schedule 4) |
| Greatest Risk | Grey market products with no quality assurance or legal protection |
Are Peptides Legal?
This is one of the most common questions I receive from patients, and I understand why. You have read about a peptide that might help your condition, your physician may have mentioned it, and now you want to know whether you can actually obtain it legally. The answer is frustrating in its complexity: it depends on which peptide, where you are, and how you are trying to access it.
Let me be direct. The regulatory landscape for therapeutic peptides is a mess. It is a patchwork of national laws, agency decisions, legal grey zones, and rapidly evolving policy that does not serve patients well. I am not saying this as a libertarian argument against regulation — quality oversight of injectable products is essential. I am saying it as a physician who regularly watches patients with legitimate medical needs navigate a system that was not designed for this category of therapeutics.
Here is what the regulatory picture actually looks like in 2026.
The United States: An Increasingly Restrictive Landscape
The FDA Framework
In the United States, peptides are regulated as drugs when they are used for therapeutic purposes. This means that, legally, a peptide intended to treat, cure, mitigate, or prevent a disease requires FDA approval. Since very few therapeutic peptides have gone through the full FDA approval process — which costs hundreds of millions of dollars and takes years — most therapeutic peptides exist in regulatory categories that were never designed for them.
The primary legal pathway for peptide access in the US has been through compounding pharmacies, which prepare customized medications to individual prescriptions. Under the Federal Food, Drug, and Cosmetic Act (sections 503A and 503B), compounding pharmacies can prepare medications using bulk drug substances that appear on specific FDA lists.
The Category 2 Decisions (2023-2025)
The critical regulatory event was the FDA’s decision to place several commonly used peptides on the Category 2 list — substances that have been evaluated and found not to meet criteria for compounding use. This began in 2023 and expanded through 2025.
Peptides that have been restricted from compounding as of early 2026 include:
- BPC-157 — Restricted based on insufficient safety data for human use and absence of a monograph
- CJC-1295 — Restricted as a growth hormone releasing compound
- Ipamorelin — Restricted alongside CJC-1295
- Selank — Limited availability through compounding
- Semax — Limited availability through compounding
Peptides that remain available through compounding (subject to ongoing review):
- Thymosin alpha-1 — Has been the subject of significant legal and regulatory dispute. As of 2026, access varies by state and by whether the compounding pharmacy operates under 503A or 503B frameworks
- PT-141 (Bremelanotide) — Available as the FDA-approved product Vyleesi, and through some compounding pharmacies
- AOD-9604 — Status varies; some compounders continue to offer it
- GHK-Cu — Primarily topical use; compounding status less restrictive
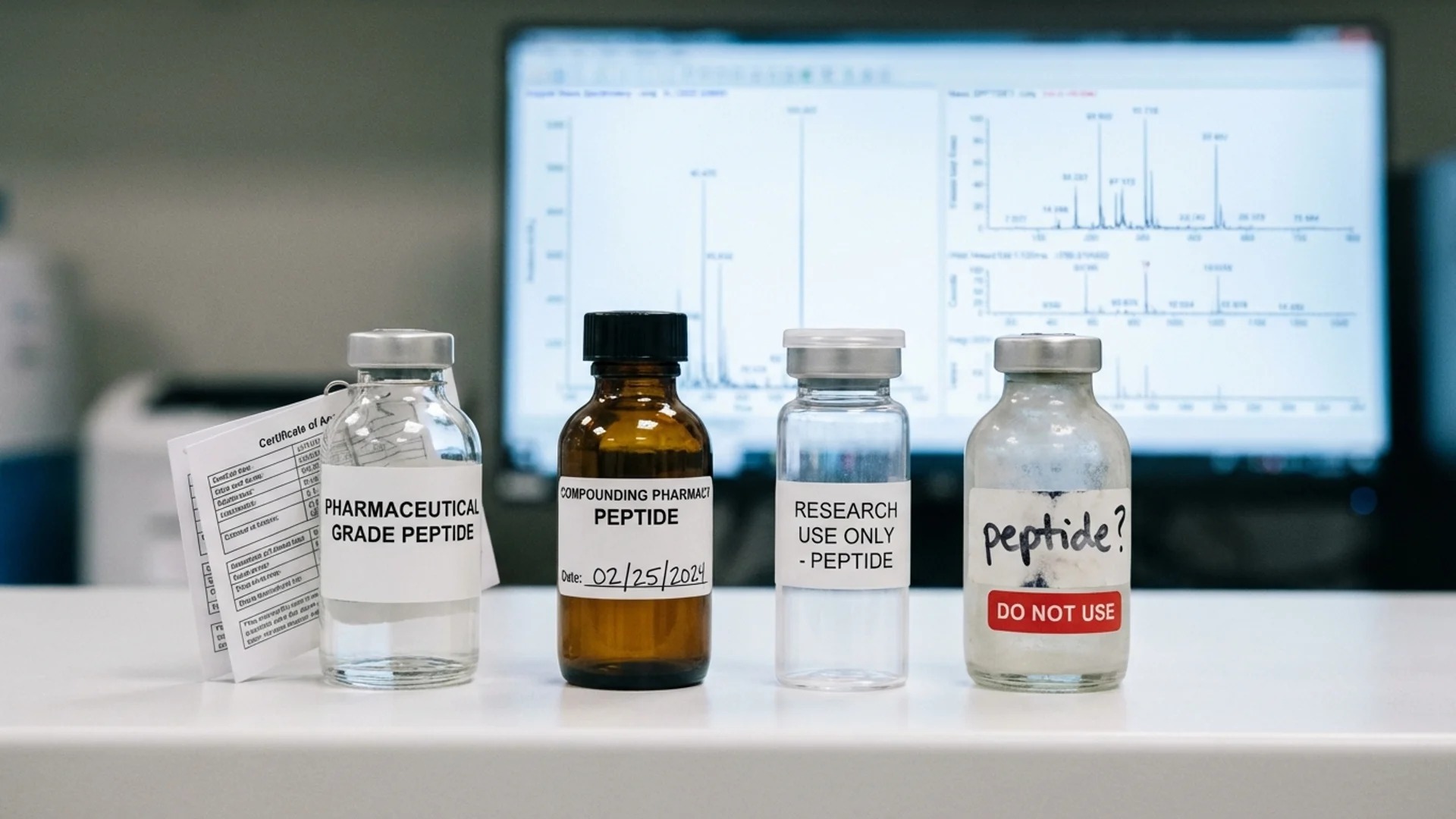
The “Research Chemical” Loophole
This is the legal grey zone that deserves honest discussion. Many peptides that are unavailable through legitimate compounding pharmacies can still be purchased online from companies that label them as “research chemicals” or “for research use only” with a disclaimer that they are “not for human consumption.”
Let me be clear about what this actually means legally and practically.
Legally: Purchasing research chemicals is not explicitly illegal for the buyer in most US states. The legal risk falls primarily on sellers who market products with implicit therapeutic claims. However, this is not a robust legal protection. If a peptide is classified as a drug and you are purchasing it for self-administration, you are operating in a genuinely grey area. You have no legal recourse if the product is contaminated, mislabeled, or causes harm.
Practically: Research chemical peptides have no regulatory quality oversight. There is no requirement for sterility testing, accurate potency verification, endotoxin testing, or identity confirmation. Independent analyses have repeatedly found significant quality problems in research chemical peptides, including incorrect peptides, subtherapeutic concentrations, contamination with synthesis byproducts, and bacterial contamination. Injecting these products carries risks that pharmaceutical or compounding pharmacy products do not.
What I tell my patients: the research chemical route is a gamble with your health. Some products from some suppliers may be perfectly fine. Others may not be. You have no reliable way to know which is which, and the cost savings are not worth the risk when you are injecting something into your body.
State-Level Variation
Some US states have enacted or are considering legislation that provides broader access to peptide therapy. These “right to try” style approaches vary in scope and enforceability. Patients should consult with a healthcare attorney or their prescribing physician about state-specific regulations.

The European Union and Germany
The EU Pharmaceutical Framework
The European regulatory approach to peptides differs structurally from the US model. While the European Medicines Agency (EMA) oversees centralized drug approvals, individual member states retain significant authority over prescribing practices, compounding, and physician-directed therapy.
There is no EU-wide equivalent to the FDA’s Category 2 compounding restrictions. Instead, the legality of peptide therapy is determined at the national level, within the broader EU pharmaceutical directive framework.
Germany: Physician Prescribing Latitude
In Germany, where I practice, the regulatory framework provides physicians with considerably more latitude in prescribing compounded and off-label substances than the US system allows.
Key features of the German framework:
Physician prescribing authority. German physicians operating within the Heilpraktikergesetz and broader medical law framework can prescribe compounded preparations, including peptides, when they determine it is medically appropriate for a specific patient. This is not unlimited freedom — physicians remain bound by professional standards, informed consent requirements, and duty-of-care obligations. But it does not require that every substance be individually approved for the specific indication.
Compounding pharmacy regulations. German Apotheken (pharmacies) with compounding licenses can prepare peptide formulations to physician prescription under the Arzneimittelgesetz (Medicines Act). Quality standards are enforced by state pharmaceutical oversight authorities. The standards are rigorous but the pathway to access is more direct than in the US.
Hospital pharmacy privilege. Hospitals like ours, operating with their own pharmacy or in partnership with licensed compounding pharmacies, can prepare and administer peptide therapies within the hospital setting with appropriate physician oversight and documentation.
What this means for patients: International patients who travel to Germany for treatment at our hospital can receive peptide therapies that may be unavailable in their home countries. This is one of the reasons we see patients from over 90 countries. The therapies are administered under direct physician supervision with pharmaceutical-grade or pharmacy-compounded products.
Other EU Member States
Regulatory approaches vary across Europe:
- Netherlands: Relatively permissive compounding framework. Several Dutch compounding pharmacies supply peptides under physician prescription.
- Switzerland: Not an EU member but relevant for European patients. Swiss pharmaceutical law allows physician-directed compounding with quality oversight.
- United Kingdom (post-Brexit): The MHRA regulates medicines. Peptides for therapeutic use generally require a prescription. The compounding framework is more restrictive than Germany’s but less restrictive than the FDA’s recent approach.
- France, Spain, Italy: Generally more restrictive. Compounding is permitted but the range of available peptides through this route is narrower.
Australia: The Scheduled Approach
Australia’s Therapeutic Goods Administration (TGA) has taken what I consider a more rational middle-ground approach to peptide regulation, though it is not without its own problems.
Schedule 4 Classification
Rather than banning peptides from compounding outright, the TGA has moved several therapeutic peptides to Schedule 4 (prescription-only) classification. This means they are legally available but only through a physician’s prescription, typically compounded by an authorized pharmacy.
Peptides that are Schedule 4 in Australia include BPC-157, thymosin alpha-1, and several growth hormone secretagogues. This approach maintains legal access while requiring physician oversight — a framework I generally support in principle.
Practical Challenges
The Australian system has its own frictions. The number of physicians who are knowledgeable about peptide therapy and willing to prescribe is limited. Compounding pharmacies that specialize in peptide preparation are concentrated in major cities. And costs can be substantial since these preparations are not covered by Medicare or private health insurance.
The TGA has also signaled increasing scrutiny of compounding pharmacies that may be operating more like manufacturers than traditional compounders, which could tighten access further.
The Compounding Pharmacy Question
Across all jurisdictions, compounding pharmacies represent the most common legal pathway for therapeutic peptide access. But patients need to understand that not all compounding pharmacies are equivalent.
US Compounding: 503A vs. 503B
In the US, there are two regulatory categories:
503A pharmacies compound medications to individual patient prescriptions. They are regulated primarily by state pharmacy boards. Quality standards and enforcement vary significantly by state.
503B outsourcing facilities can produce larger batches without individual prescriptions. They are registered with and inspected by the FDA. They must comply with current Good Manufacturing Practice (cGMP) standards. This is a higher quality bar, and 503B products generally offer better quality assurance.
For peptide therapy specifically, I recommend patients use 503B facilities when available. The additional regulatory oversight is meaningful for injectable products.
Quality Markers to Look For
Regardless of jurisdiction, these are the quality indicators patients should expect from a compounding pharmacy preparing injectable peptides:
- Third-party testing with a certificate of analysis (COA) available for each batch
- Sterility testing of all injectable preparations
- Endotoxin testing (bacterial pyrogen testing)
- Potency verification confirming the labeled concentration matches the actual concentration
- Beyond-use dating based on stability testing, not arbitrary assignment
- Proper storage and shipping with temperature monitoring
If a compounding pharmacy cannot provide these, find one that can. In my clinical experience, the quality difference between the best and worst compounding pharmacies is not marginal — it is the difference between a reliable medical product and a gamble.

Prescription Requirements
A question I hear frequently: “Do I need a prescription for peptides?”
The answer, in virtually every jurisdiction with functional pharmaceutical regulation, is yes — for injectable peptides intended for therapeutic use. Oral peptide supplements (collagen peptides, certain bioactive peptides) may be available over the counter as dietary supplements, but injectable therapeutic peptides are prescription products in the US, EU, Australia, and most other regulated markets.
What this means practically:
- You need a physician who is knowledgeable about peptide therapy and willing to prescribe
- The physician should conduct appropriate baseline evaluation (labs, medical history, physical exam)
- The prescription should specify the peptide, dose, concentration, route, and duration
- Follow-up monitoring should be part of the treatment plan
Finding a knowledgeable prescriber is often the greatest practical barrier. Many conventional physicians have limited familiarity with therapeutic peptides. Physicians who specialize in functional medicine, anti-aging medicine, or integrative approaches are more likely to be familiar with peptide protocols, though quality and knowledge vary widely in this space as well.
The Grey Market: What Patients Need to Understand
I want to address the grey market directly because pretending it does not exist serves no one.
A significant number of patients using therapeutic peptides — possibly the majority in the US since the 2023 compounding restrictions — are obtaining them through unregulated sources. These include websites selling “research chemicals,” overseas suppliers, and peer-to-peer networks.
The Risks Are Real
Quality risk. Independent laboratory analyses of grey-market peptides have documented products containing the wrong peptide entirely, products with 30 to 70 percent less active ingredient than labeled, products contaminated with bacterial endotoxins, and products containing synthesis impurities. These are not theoretical concerns. They are documented findings.
Legal risk. While prosecution of individual buyers is rare, it is not impossible. Importing prescription medications without a valid prescription is technically illegal in most jurisdictions. More practically, you have no legal recourse if a grey-market product causes harm.
Medical risk. Without physician oversight, patients may be using peptides at inappropriate doses, for inappropriate indications, with inadequate monitoring, or in combinations that create risks. The peptide itself may be reasonable — the context of unsupervised use is the problem.
Why Patients Turn to the Grey Market
This is where I channel my frustration with the regulatory status quo. Patients do not turn to grey-market peptides because they enjoy risk. They do it because:
- Their physician will not prescribe peptides due to unfamiliarity or liability concerns
- The specific peptide they need has been restricted from compounding (US)
- The cost of legally obtained peptides through compounding pharmacies is prohibitive
- They have a legitimate medical need and have exhausted conventional options
These are rational responses to a system that fails them. That does not make grey-market use safe or advisable — but understanding why it happens is necessary for any honest conversation about peptide regulation.
What I Tell My Patients
The nuance matters here, and I resist the temptation to give a simple answer to a complicated question.
If you are in the United States and want to use peptide therapy legally and safely, your path is: find a knowledgeable physician, get appropriate baseline testing, obtain peptides through a quality compounding pharmacy (ideally 503B), and maintain follow-up monitoring. This path has become narrower since 2023, and I acknowledge that it is frustrating and expensive.
If you are willing to travel, Germany and several other European jurisdictions offer legal access to a broader range of therapeutic peptides under direct physician supervision. This is one of the services we provide at St. George Hospital for international patients, and it is a legitimate reason that medical tourism for peptide therapy exists.
If you are considering grey-market peptides, I would rather you did so with your eyes open than in ignorance. Understand the quality risks, understand the legal ambiguity, and at minimum work with a physician who can monitor your response, even if they did not prescribe the peptide.
What I hope changes: a regulatory framework that distinguishes between novel synthetic drugs requiring full approval and endogenous peptides or close analogs that merit a streamlined pathway for physician-directed therapeutic use. The current system, particularly in the US, forces patients to choose between legal access to a shrinking list of compounds and grey-market access to everything else. Neither extreme serves patient safety.
The Bottom Line
Peptide legality in 2026 is jurisdiction-dependent, peptide-specific, and actively evolving. The safest and most reliable path remains physician-prescribed, pharmacy-compounded therapy within your country’s legal framework. Where that framework is too restrictive for legitimate medical needs, international treatment under proper medical supervision is a viable alternative. The grey market exists and will continue to exist as long as regulatory frameworks fail to provide reasonable legal access — but it carries risks that patients should not minimize. Work with a knowledgeable physician. Demand quality-assured products. And advocate for better regulation rather than accepting the current status quo.
References
- U.S. Food and Drug Administration. Bulk Drug Substances Used in Compounding Under Section 503B of the FD&C Act. FDA.gov. Updated 2025.
- U.S. Food and Drug Administration. Category 2 Bulk Drug Substances: Nominated Substances Not Eligible for Use in Compounding. FDA.gov. Updated 2025.
- Gudeman J, et al. Potential risks of pharmacy compounding. Drugs in R&D. 2013;13(1):1-8. doi:10.1007/s40268-013-0005-9
- European Commission. Directive 2001/83/EC of the European Parliament and of the Council on the Community code relating to medicinal products for human use. Amended through 2024.
- Therapeutic Goods Administration. Scheduling of peptide-based substances: Scheduling delegate’s interim decision. TGA.gov.au. 2024.
- Arzneimittelgesetz (AMG). German Medicines Act. Federal Ministry of Health. Current consolidated version 2025.
- Cohen PA, et al. Quantity of active ingredients in illegally marketed peptide products. JAMA Network Open. 2023;6(4):e239091.
- National Academies of Sciences, Engineering, and Medicine. Compounded Topical Pain Creams: Review of Select Ingredients for Safety, Effectiveness, and Use. Washington, DC: National Academies Press. 2020.