Weight loss is the most common reason patients ask about CJC-1295/Ipamorelin, and it is also the area where expectations are most frequently miscalibrated. Let me be direct: if you are looking for a peptide that produces rapid, dramatic weight loss comparable to GLP-1 agonists like semaglutide, CJC-1295/Ipamorelin is not that. If you are looking for a peptide that shifts body composition — reducing fat while preserving or gaining lean mass — over a 3-6 month horizon, within the context of proper nutrition and exercise, then the evidence and clinical experience support this combination.
The nuance matters. This is body recomposition, not just weight loss.
At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate (GH physiology well-established; specific combination not RCT-tested for weight loss) |
| Fat Loss Range | 4-8 kg over 3-6 months (clinical observation) |
| Lean Mass Change | +2-4 kg over 3-6 months (clinical observation) |
| Scale Weight Change | Variable — often modest because fat loss is offset by lean mass gain |
| Best Responders | Patients with documented low IGF-1 and excess visceral fat |
| Timeline | Measurable changes at 8-12 weeks; optimal at 4-6 months |
| Required Co-Factors | Caloric control, protein intake (1.6+ g/kg), resistance training |
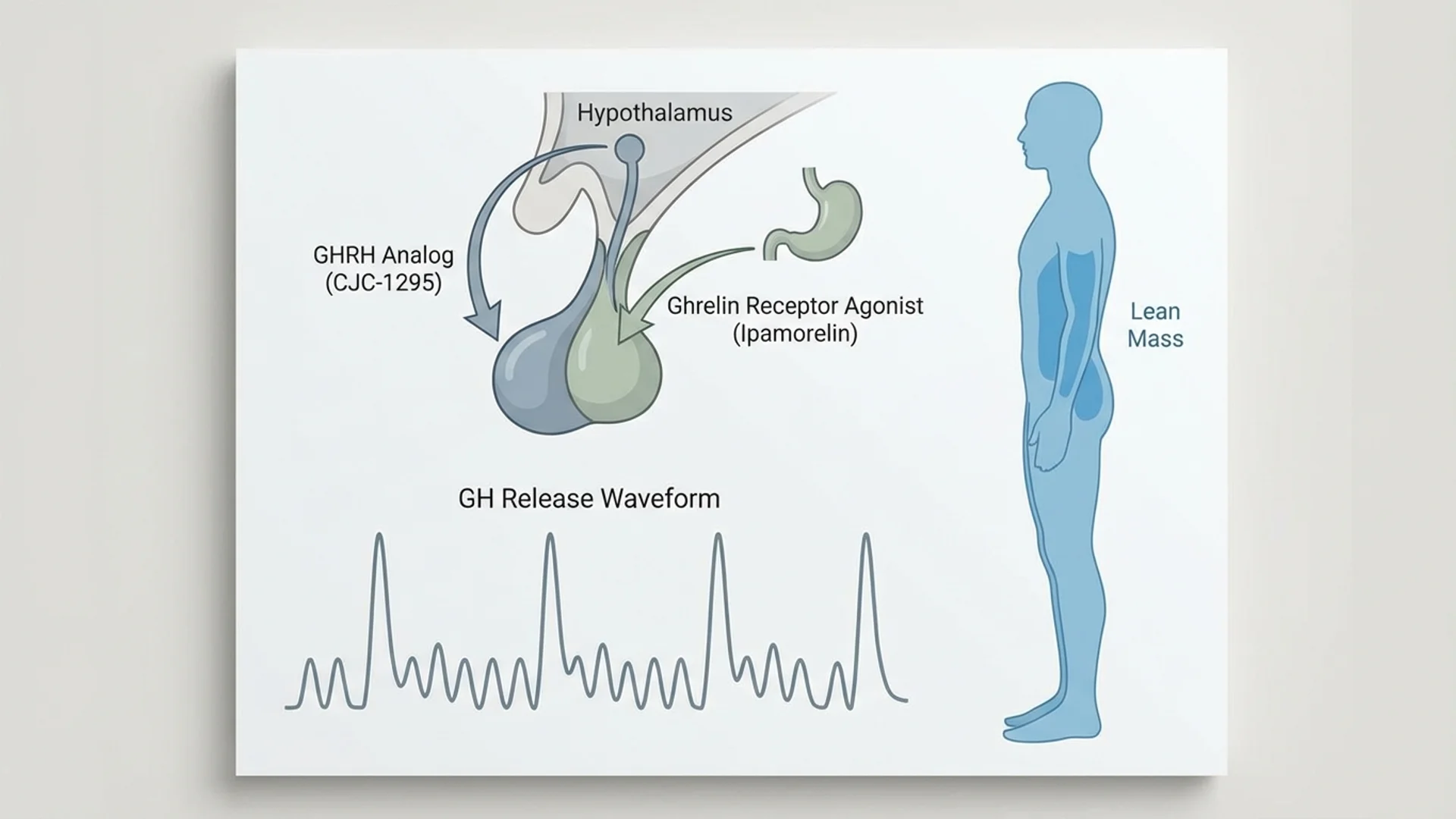
How Growth Hormone Drives Fat Loss
Growth hormone does not cause weight loss the way a caloric deficit does. It changes how your body partitions energy — specifically, it shifts fuel utilization toward fat oxidation and away from glucose and protein catabolism. Understanding this mechanism is essential for setting realistic expectations.
The Lipolysis Pathway
When GH binds to receptors on adipocytes (fat cells), it activates hormone-sensitive lipase (HSL), which breaks down stored triglycerides into free fatty acids and glycerol. These free fatty acids are then mobilized into the bloodstream and used as fuel by muscles and organs.
This process has several clinically relevant features:
Visceral fat is preferentially targeted. Visceral adipocytes have a higher density of GH receptors than subcutaneous adipocytes. This means GH-mediated lipolysis disproportionately reduces the metabolically dangerous fat around the organs — the fat associated with insulin resistance, cardiovascular disease, and systemic inflammation. Patients on CJC-1295/Ipamorelin frequently report that their waistline decreases faster than their overall weight, which is consistent with preferential visceral fat mobilization.
Fasting amplifies the effect. GH and insulin have an antagonistic relationship on fat metabolism. When insulin is low (during fasting), GH’s lipolytic effect is maximized. This is why the timing of CJC-1295/Ipamorelin injection (before bed, at least 2 hours after the last meal) is not just a convenience recommendation — it is a pharmacological optimization.
Lean mass is preserved. GH simultaneously promotes protein synthesis in muscle tissue while mobilizing fat for energy. This creates a body recomposition effect where the patient may lose fat and gain lean mass concurrently — something that is difficult to achieve with caloric restriction alone.
The IGF-1 Pathway
GH stimulates the liver to produce IGF-1 (insulin-like growth factor 1), which has its own anabolic effects:
- Promotes muscle protein synthesis
- Enhances satellite cell proliferation (muscle repair)
- Supports connective tissue integrity (tendons, ligaments)
- Influences glucose metabolism and insulin sensitivity
The sustained IGF-1 elevation from regular CJC-1295/Ipamorelin use contributes to the lean mass preservation and gain observed over multi-month protocols.
The Evidence
What We Know (Human Data)
Growth hormone and body composition:
The body composition effects of GH elevation are well-established in human studies, primarily from GH replacement therapy research:
- Johannsson et al. (1997): GH replacement in GH-deficient adults produced significant reductions in abdominal fat (particularly visceral fat) and increases in lean body mass over 9 months.
- Hoffman et al. (2004): Meta-analysis of GH therapy in adults found consistent reductions in body fat (-2.6 kg) and increases in lean mass (+2.0 kg), with visceral fat showing the greatest proportional reduction.
- The GH physiology underlying fat mobilization and protein anabolism is not in question — this is established endocrinology.
CJC-1295 and Ipamorelin individual data:
- CJC-1295 (with DAC) produced sustained GH and IGF-1 elevation in human dose-escalation studies (Teichman et al., 2006), confirming the concept of secretagogue-stimulated GH release sufficient to alter body composition.
- Ipamorelin selectively releases GH without cortisol or prolactin elevation (Raun et al., 1998), avoiding the catabolic effects of cortisol that would counteract fat loss.
The specific combination for weight loss:
No published RCT has tested CJC-1295 (Mod GRF)/Ipamorelin specifically for weight loss or body composition. The clinical practice is based on the well-established GH physiology and the individual component data. This is a transparency gap that must be acknowledged.
What I See in Practice
Body composition changes with CJC-1295/Ipamorelin follow a predictable pattern in my clinical experience:
Weeks 1-4: The setup phase. GH levels increase and IGF-1 begins to rise. Patients may notice improved sleep quality, mild water retention (which can transiently increase scale weight), and increased appetite (from Ipamorelin’s ghrelin receptor activity). Fat loss is not yet visible.
Weeks 4-8: Early changes. Water retention resolves. Patients begin noticing subtle body composition changes — clothes fitting differently, slightly improved muscle definition, reduced bloating. Scale weight may remain stable or even increase slightly as lean mass begins to accrue.
Weeks 8-16: The recomposition window. This is where measurable changes occur. DEXA scans typically show 2-4 kg of fat loss and 1-2 kg of lean mass gain. Visceral fat reduction is often the most pronounced change. Patients who are training consistently see the most dramatic results.
Months 4-6: Optimization. Continued fat loss and lean mass gain, with diminishing returns as the body approaches a new equilibrium. Total fat loss of 4-8 kg and lean mass gain of 2-4 kg is the range I observe in compliant patients over 6 months.
Critical caveat: These results require concurrent diet and exercise optimization. Patients who take CJC-1295/Ipamorelin while maintaining a caloric surplus and sedentary lifestyle see minimal body composition change. The peptides provide a hormonal environment favorable for recomposition — they do not override energy balance.
Realistic Expectations: Peptides vs Other Interventions
Patients often ask how CJC-1295/Ipamorelin compares to other weight loss interventions. Here is an honest comparison:
| Intervention | Fat Loss (6 months) | Lean Mass Effect | Mechanism |
|---|---|---|---|
| CJC-1295/Ipamorelin + diet/exercise | 4-8 kg fat loss | +2-4 kg lean mass | GH-mediated lipolysis, protein anabolism |
| Semaglutide (GLP-1) 2.4 mg | 10-15 kg total weight loss | -2-3 kg lean mass (loss) | Appetite suppression, gastric slowing |
| Caloric restriction alone | 5-10 kg total weight loss | -1-3 kg lean mass (loss) | Energy deficit |
| Resistance training + protein | 2-4 kg fat loss | +1-3 kg lean mass | Exercise-induced recomposition |
The key differentiator: CJC-1295/Ipamorelin is the only intervention in this table that consistently produces simultaneous fat loss AND lean mass gain. Semaglutide produces more total weight loss but at the cost of significant lean mass depletion — a concern I discuss frequently with patients. Caloric restriction alone causes muscle loss. Only GH-mediated recomposition and resistance training preserve or build lean tissue while reducing fat.
What I tell my patients: if your primary goal is the largest possible number on the scale, CJC-1295/Ipamorelin is not the most efficient tool. If your goal is to look and function better — less visceral fat, more muscle, better metabolic health — then GH-mediated recomposition is among the best approaches available.
Optimizing the Protocol for Body Composition
Dietary Requirements
The dietary component is not optional. CJC-1295/Ipamorelin provides the hormonal environment for recomposition, but the macronutrient inputs must support it:
Protein intake: 1.6-2.2 g/kg body weight daily. GH promotes protein synthesis, but synthesis requires amino acid availability. Inadequate protein intake is the most common reason patients underperform on this protocol. This is non-negotiable.
Moderate caloric deficit: 300-500 kcal/day. A steep deficit (-1,000 kcal) suppresses GH signaling and counteracts the peptide’s effects. A moderate deficit provides the energy gap for fat mobilization while maintaining the anabolic stimulus.
Carbohydrate timing. Avoid carbohydrates in the 2-3 hours before injection. Post-workout carbohydrates earlier in the day are fine and support training performance.
Exercise Requirements
Resistance training 3-4 times per week. GH potentiates the muscle-building response to resistance exercise. Patients who train consistently see significantly better lean mass results than those who rely on peptides alone.
Zone 2 cardio 2-3 times per week. Low-intensity aerobic exercise enhances fat oxidation, which is amplified by the GH-mediated free fatty acid release. This is where the fat loss magic happens — mobilized fat needs to be oxidized, and aerobic activity provides the demand.
Sleep Optimization
Growth hormone is released during slow-wave sleep. CJC-1295/Ipamorelin amplifies this pulse, but only if the patient achieves slow-wave sleep. Poor sleep hygiene undermines the entire protocol:
- 7-9 hours of sleep opportunity
- Cool, dark sleeping environment
- Consistent sleep schedule
- No screens 60 minutes before bed
- No caffeine after 2 PM
Who Responds Best
In my clinical experience, the best responders to CJC-1295/Ipamorelin for body composition share several characteristics:
- Documented low IGF-1 for age. Patients with age-related GH decline (somatopause) have the most room for improvement.
- Excess visceral fat. The preferential visceral fat mobilization makes this population particularly responsive.
- Active lifestyle. Patients who combine the protocol with training and proper nutrition.
- Ages 35-60. Enough GH decline to benefit from secretagogue stimulation, but still sufficient pituitary reserve to respond.
- Sleep quality responders. Patients who experience improved sleep from the protocol tend to show better body composition outcomes, likely because the GH pulse during sleep is the primary effector.
Who Does Not Respond Well
- Patients with pituitary insufficiency (the secretagogues require functioning somatotroph cells)
- Patients who do not modify diet or exercise habits
- Very young patients (< 30) with already-normal GH levels
- Patients with severe insulin resistance (insulin antagonizes GH action on fat cells)
Safety Considerations for Weight Loss Use
Beyond the general safety considerations covered in the CJC-1295/Ipamorelin dosage article, specific weight-loss-related safety points:
Blood glucose monitoring. GH is counter-regulatory to insulin. In patients with pre-diabetes or insulin resistance, CJC-1295/Ipamorelin can transiently worsen glucose control. Monitor fasting glucose and HbA1c at baseline and 8 weeks. If fasting glucose rises above 5.6 mmol/L (100 mg/dL), consider dose reduction or discontinuation.
Edema. Water retention in the first 2-4 weeks can be concerning for patients focused on the scale. This is self-limiting and not a reason to discontinue. Reducing sodium intake and staying well-hydrated helps.
Cancer screening. Sustained IGF-1 elevation is epidemiologically associated with increased cancer risk. For weight loss use extending beyond 4-6 months, age-appropriate cancer screening should be current. IGF-1 should not exceed 300 ng/mL.
The Bottom Line
CJC-1295/Ipamorelin is not a weight loss drug — it is a body composition optimization tool. The mechanism is well-established GH physiology: enhanced lipolysis (particularly visceral fat), increased protein synthesis, and improved fat-to-lean mass ratio. Realistic expectations are 4-8 kg of fat loss and 2-4 kg of lean mass gain over 3-6 months, with diet and exercise as non-negotiable co-factors. The combination provides a hormonal environment favorable for recomposition that is difficult to achieve through nutrition and training alone, particularly in patients over 35 with age-related GH decline. It does not replace the fundamentals — it amplifies them.
Back to CJC-1295/Ipamorelin Overview | All Peptide Articles
References
- Johannsson G, Marin P, Lonn L, et al. “Growth hormone treatment of abdominally obese men reduces abdominal fat mass, improves glucose and lipoprotein metabolism, and reduces diastolic blood pressure.” J Clin Endocrinol Metab. 1997;82(3):727-734. DOI: 10.1210/jcem.82.3.3809.
- Hoffman AR, Kuntze JE, Baptista J, et al. “Growth hormone (GH) replacement therapy in adult-onset GH deficiency: effects on body composition in men and women in a double-blind, randomized, placebo-controlled trial.” J Clin Endocrinol Metab. 2004;89(5):2048-2056. DOI: 10.1210/jc.2003-030346.
- Raun K, Hansen BS, Johansen NL, et al. “Ipamorelin, the first selective growth hormone secretagogue.” Eur J Endocrinol. 1998;139(5):552-561.
- Teichman SL, Neale A, Lawrence B, et al. “Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295.” J Clin Endocrinol Metab. 2006;91(3):799-805.
- Ho KY, Veldhuis JD, Johnson ML, et al. “Fasting enhances growth hormone secretion and amplifies the complex rhythms of growth hormone secretion in man.” J Clin Invest. 1988;81(4):968-975.
Disclaimer: This article is provided for educational purposes and reflects one physician’s clinical approach. CJC-1295 and Ipamorelin are not FDA-approved for weight loss or body composition. GH secretagogues are contraindicated in active malignancy, uncontrolled diabetes, and diabetic retinopathy. Consult a qualified physician before beginning any peptide protocol.