
Featured
Magnesium: 7 Forms Compared — Which One Do You Need?
Magnesium glycinate vs threonate vs taurate and 4 more forms compared. Dosing, deficiency signs, and why serum testing is unreliable. A physician's guide.
Condition
Testosterone optimization, hormone health, prostate care, and performance medicine. Evidence-based approaches to men's health beyond marketing.
Why St. George Hospital uses 2 extreme hyperthermia sessions at 41.6-41.8°C for Lyme eradication, not 5-6 moderate sessions. The science behind the protocol.
Honest guide to whole-body hyperthermia side effects. What happens during treatment, common reactions, Herxheimer responses, recovery timeline, and contraindications.
Options beyond atovaquone-azithromycin for relapsing babesiosis. Combination protocols, herbal adjuncts, and when exchange transfusion is considered.
Evidence-based herbal protocols for Bartonella including Cryptolepis, Japanese Knotweed, and Cat's Claw — what the research shows and how clinicians use them.
A direct comparison of American IDSA Lyme guidelines and German integrative Lyme treatment. Why patients travel to Germany, what's different, and what the evidence supports.
Does a Herxheimer reaction mean treatment is working? The science behind die-off, why worse does not always mean better, and the goal of controlled pathogen clearance.
Evidence-based strategies for managing Jarisch-Herxheimer reactions during Lyme treatment — hydration, detox support, dose pacing, and when to call your doctor.
Physician-ranked guide to sleep supplements. Magnesium glycinate, glycine, apigenin, L-theanine, and ashwagandha compared by evidence quality for deep sleep enhancement.
Evidence-based guide to testosterone optimization after 40. Testing, natural decline, the optimization ladder from lifestyle to TRT, risks, benefits, and monitoring — from a physician who treats it daily.

What to expect during brain fog recovery after Lyme treatment — the multi-system recovery approach, realistic timelines, and evidence-based strategies.
Evidence-based CJC-1295/Ipamorelin dosing guide by Dr. Julian Douwes. Nightly subcutaneous protocols, DAC vs no-DAC, cycling, and growth hormone optimization.
How TB-500 supports tendon and ligament healing. Mechanisms, preclinical evidence, clinical observations, and practical protocols for connective tissue.

Evidence-based guide to ashwagandha. Cortisol reduction, thyroid effects, dosing, extract types, safety, and what the clinical data actually shows.
Physician guide to berberine dosing for blood sugar, insulin sensitivity, and metabolic health. Optimal doses, timing, GI management, and comparison to metformin.
Head-to-head comparison of berberine and metformin for glucose control, lipids, and longevity. Both activate AMPK — but how do they really compare?
Evidence-based guide to CoQ10 supplementation. Ubiquinol vs ubiquinone, absorption differences, statin interactions, mitochondrial function, and what I recommend in clinical practice.
Physician guide to CoQ10 dosing by condition. Ubiquinol vs ubiquinone, heart health, male fertility, migraine prevention, energy, and statin users. Evidence-based protocols.
Physician guide to CoQ10 depletion from statins. Why it happens, symptoms of statin-induced CoQ10 deficiency, optimal dosing with ubiquinol, and what the evidence shows.
The bioavailability problem with curcumin explained. Comparing Meriva, Longvida, BCM-95, Theracurmin, liposomal, and piperine forms. Dosing by condition.

Physician comparison of curcumin formulations for absorption. Meriva, BCM-95, Theracurmin, NovaSOL, and piperine ranked by bioavailability data, clinical evidence, and cost.
Evidence-based curcumin dosing for joint pain and arthritis. Meta-analysis results, comparison to NSAIDs, best formulations, timeline to improvement, and physician protocols.

Physician guide to curcumin vs turmeric supplements. Why turmeric spice has poor bioavailability, how curcumin extracts differ, and what to look for in a supplement.
Physician comparison of fish oil, krill oil, and algae oil for omega-3 supplementation. EPA and DHA content, absorption, sustainability, cost, and evidence-based recommendations.

Evidence-based guide to lion's mane mushroom for brain health. NGF stimulation, cognitive benefits, dosing, extract types, and what the clinical data supports.

Physician guide to magnesium deficiency symptoms including muscle cramps, insomnia, anxiety, heart palpitations, and fatigue. Testing, causes, and how to correct it.

Physician comparison of magnesium glycinate vs magnesium L-threonate. Which form for sleep, which for cognition, absorption differences, dosing, and evidence quality.

Physician guide to magnesium supplement timing. When to take glycinate, threonate, citrate, and other forms for maximum absorption and effect. Morning vs night, food interactions.
NAC N-acetyl cysteine benefits reviewed by a physician. Glutathione precursor, psychiatric uses, liver protection, COVID research, and dosing from 600-1800mg.

Evidence-based NAC dosing by condition. Liver support, respiratory health, immune function, mental health, and general antioxidant use. Physician-guided protocols.
Evidence-based guide to NAC for fertility in men and women. PCOS, ovulation, sperm quality, oxidative stress, and dosing protocols from clinical trials.
Physician comparison of NAC vs glutathione supplements. Oral bioavailability, mechanisms, when to use each, liposomal glutathione, and evidence-based recommendations.
Evidence-based guide to nattokinase for fibrinolysis and microclots. Mechanism, dosing, post-COVID relevance, combination with serrapeptase, and safety with blood thinners.
Omega-3 EPA and DHA dosing guide by condition. Therapeutic vs maintenance doses, omega-3 index testing, fish oil vs algal, and quality markers. Evidence graded honestly.
Evidence-based omega-3 dosing for inflammation. How much EPA and DHA for joint pain, cardiovascular inflammation, neuroinflammation, and autoimmune conditions. Physician protocols.
Evidence-based guide to probiotic strain selection. Which strains work for which conditions, when to avoid probiotics, CFU counts, spore-based vs traditional, and what I use in clinical practice.
Physician guide to evidence-based probiotic strain selection. Which specific strains work for IBS, bloating, immunity, mood, and vaginal health, with dosing and evidence grades.

Physician guide to choosing a probiotic supplement. CFU count myths, strain identification, delivery mechanisms, third-party testing, and what the label should tell you.

Physician guide to probiotics, prebiotics, postbiotics, and synbiotics. Definitions, mechanisms, when to use each, and how they work together for gut health.
Physician guide to quercetin senolytic protocols. Quercetin + dasatinib evidence, quercetin + fisetin alternatives, dosing schedules, and the science of clearing senescent cells.

Evidence-based supplement timing guide. Fat-soluble vitamins with meals, magnesium at night, iron on an empty stomach, and how to build morning and evening stacks based on pharmacokinetics.
Vitamin D benefits and dosing from a physician. Optimal levels, cofactors K2 and magnesium, immune modulation, LL-37 upregulation, and why most people are deficient.

Testosterone, DHEA, thyroid, and growth hormone in aging men. Evidence-based approach to male hormonal health and longevity.

Estrogen, progesterone, thyroid, and DHEA in aging women. Evidence-based approach to female hormonal health across perimenopause and beyond.
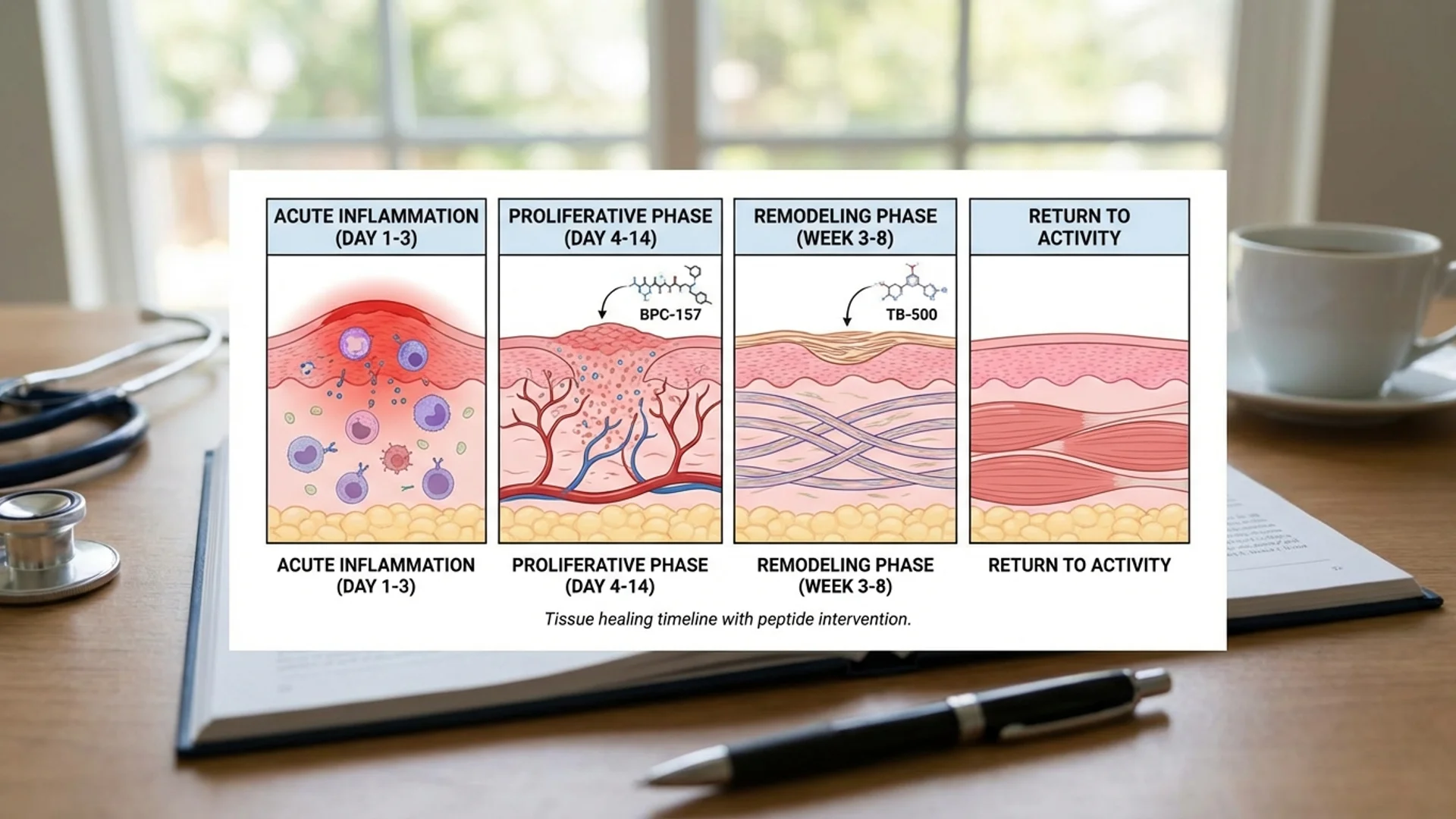
BPC-157 and TB-500 for injury recovery, surgical healing, and athletic performance. Evidence-based protocol from Dr. Julian Douwes.
Evidence-based protocol for mental clarity, focus, and memory from a physician who treats cognitive dysfunction daily.

An evidence-based recovery protocol addressing inflammation, clotting, energy, and immune regulation after COVID-19. By Dr. Julian Douwes.

How to prepare your body before traveling to St. George Hospital for Lyme, Post-COVID, or integrative cancer treatment.
Schedule a consultation to discuss your case with Dr. Julian Douwes and the clinical team at St. George Hospital.
Complete Guide
In-depth reference by Dr. Julian Douwes
Men die, on average, five years earlier than women in virtually every developed country. They are more likely to die from nine of the ten leading causes of death. They are significantly less likely to seek preventive medical care, and when they do present, their conditions are often more advanced.
This is not inevitable biology. Much of this disparity is behavioral and systemic: men are socialized to ignore symptoms, medical education has historically underemphasized male-specific hormonal health, and the healthcare system has not created pathways that encourage men to engage proactively with their health.
At St. George Hospital, we have developed a dedicated men’s health program because we believe that the hormonal, cardiovascular, metabolic, and psychological dimensions of men’s health deserve the same rigorous, evidence-based attention that women’s health has rightly received over the past several decades. This is not “anti-aging” vanity medicine. It is serious preventive and restorative medicine grounded in clinical evidence.
No topic in men’s health generates more confusion than testosterone. There are those who treat it as a fountain of youth and those who consider it dangerous. The truth, as usual, is more nuanced.
For years, the primary concern about testosterone replacement therapy (TRT) was cardiovascular risk. The 2023 TRAVERSE trial — a large, randomized, placebo-controlled cardiovascular safety trial involving over 5,000 men — put this concern to rest for appropriately selected patients. The trial demonstrated no increased risk of major adverse cardiovascular events in men with hypogonadism receiving testosterone therapy compared to placebo.
This does not mean testosterone is risk-free. It means that in men with documented testosterone deficiency and symptoms consistent with hypogonadism, the cardiovascular fear that prevented many physicians from prescribing TRT was not supported by rigorous evidence. The TRAVERSE trial changed the risk-benefit conversation fundamentally.
Testosterone replacement is indicated when a man has both documented low testosterone levels (typically total testosterone below 300 ng/dL on multiple morning measurements, confirmed with free testosterone and SHBG) and symptoms consistent with deficiency: persistent fatigue, reduced libido, erectile dysfunction, loss of muscle mass, increased body fat, depressed mood, cognitive decline, or reduced bone density.
Both criteria must be met. A low number alone, without symptoms, does not necessarily require treatment. And symptoms alone, without laboratory confirmation, may have other causes that deserve investigation first.
At St. George Hospital, we use bioidentical testosterone — molecularly identical to the testosterone produced by the human body. This is administered via transdermal gel, intramuscular injection, or subcutaneous injection, depending on patient preference and pharmacokinetic goals.
We do not use synthetic androgens or anabolic steroids. The goal is physiologic replacement — restoring levels to the healthy range, not pushing them to supraphysiologic concentrations. The distinction matters for both efficacy and safety.
Responsible testosterone therapy requires consistent monitoring. We check the following at regular intervals:
This monitoring is non-negotiable. Any physician who prescribes testosterone without regular blood work is not practicing responsible medicine.
Testosterone, while important, is only one component of male hormonal health. A comprehensive evaluation addresses several additional axes.
Dehydroepiandrosterone (DHEA) is the most abundant steroid hormone in the body and serves as a precursor to both testosterone and estrogen. DHEA levels decline steadily from age 25 onward, and low levels are associated with reduced immune function, fatigue, decreased sense of well-being, and loss of bone density. We measure DHEA-S (the sulfated, stable form) and supplement cautiously when levels are suboptimal.
Thyroid dysfunction in men is underdiagnosed because it is considered “a women’s disease.” In reality, subclinical hypothyroidism in men contributes to fatigue, weight gain, cognitive sluggishness, depression, and elevated cholesterol. We assess the complete thyroid panel — not just TSH, but free T3, free T4, reverse T3, and thyroid antibodies — because a normal TSH can mask meaningful functional thyroid insufficiency.
Growth hormone (GH) declines progressively with age, contributing to reduced muscle mass, increased visceral fat, thinning skin, decreased exercise capacity, and impaired recovery. We assess GH status through IGF-1 levels and, where indicated, provocative stimulation testing. When deficiency is documented, we discuss the evidence, risks, and benefits of GH therapy with full transparency. Growth hormone therapy is a regulated treatment in Germany and is prescribed only for documented deficiency, not as a lifestyle enhancement.
Chronic stress disrupts the diurnal cortisol pattern, and many men presenting with fatigue, abdominal weight gain, insomnia, and reduced stress tolerance have measurable HPA axis dysregulation. We assess this through four-point salivary cortisol testing, which maps the cortisol curve throughout the day. Treatment addresses root causes — stress management, sleep optimization, adaptogenic support — rather than simply suppressing cortisol.
Prostate-specific antigen (PSA) testing remains controversial, and I think the controversy has done men a disservice. The US Preventive Services Task Force initially recommended against routine PSA screening, then revised its position to recommend shared decision-making. The problem was never the test itself, but how results were acted upon — leading to overdiagnosis and overtreatment of indolent cancers.
My position is that informed PSA testing, interpreted in context (PSA velocity, free-to-total PSA ratio, age-specific reference ranges, and prostate health index where available), remains a valuable tool for early detection when combined with clinical judgment. The key is nuanced interpretation, not abandonment of screening.
BPH affects the majority of men over 50 and significantly impacts quality of life through urinary frequency, urgency, nocturia, and incomplete emptying. We address BPH through a combination of targeted botanicals with evidence (saw palmetto extract standardized to 85-95% fatty acids, beta-sitosterol), lifestyle modifications (reduced evening fluid intake, pelvic floor exercises), and conventional medications (5-alpha reductase inhibitors, alpha-blockers) when indicated.
Prostate cancer prevention draws on epidemiological evidence: maintaining a healthy body weight, regular physical activity, adequate selenium and vitamin D status, consumption of lycopene-rich foods, and management of chronic inflammation all appear to confer protective benefit. We integrate these strategies into our comprehensive men’s health programs.
Sexual dysfunction is one of the most common reasons men seek medical attention, yet it remains surrounded by stigma that prevents honest clinical discussion. I approach this topic the same way I approach cardiovascular disease or metabolic syndrome: as a medical issue that deserves proper diagnosis and treatment.
Erectile dysfunction (ED) in men over 40 is frequently a vascular problem — the penile arteries are among the smallest in the body, and endothelial dysfunction manifests there before it manifests in the coronary arteries. ED has been demonstrated to precede cardiovascular events by an average of 3-5 years, making it an important early warning sign.
Our evaluation of ED includes vascular assessment (carotid intima-media thickness, endothelial function), hormonal evaluation (testosterone, thyroid, prolactin), and psychological screening. Treatment addresses root causes — hormone optimization, vascular health improvement, stress management — rather than simply prescribing phosphodiesterase inhibitors, though these medications remain useful tools in the appropriate context.
Libido, ejaculatory function, and overall sexual satisfaction are also addressed within the hormone optimization framework. Low testosterone, elevated prolactin, thyroid dysfunction, and medication side effects are all common and treatable causes of sexual complaints.
Heart disease is the leading killer of men worldwide, and the standard lipid panel — total cholesterol, LDL, HDL, triglycerides — is insufficient for proper risk assessment. Many men who experience cardiac events have “normal” standard lipid values.
We advocate for advanced cardiovascular testing:
Every man over 40 should know his ApoB and Lp(a) levels. If Lp(a) is elevated, aggressive management of other modifiable risk factors becomes essential. If the CAC score is non-zero, the conversation about treatment intensity changes significantly.
Sarcopenia — the age-related loss of muscle mass and strength — begins in the fourth decade and accelerates after age 60. It is associated with increased fracture risk, metabolic dysfunction, insulin resistance, reduced functional independence, and increased mortality.
Prevention and treatment are straightforward in principle:
Resistance training is the single most effective intervention. Progressive overload through compound movements (squat, deadlift, press, row) 2-4 times weekly, with appropriate programming for age and fitness level, is more impactful than any supplement or medication.
Protein intake of 1.6-2.2 grams per kilogram of body weight per day, distributed across meals, provides the amino acid substrate necessary for muscle protein synthesis. Most men over 40 consume inadequate protein.
Creatine monohydrate (3-5 grams daily) is the most well-studied performance supplement in existence, with decades of safety data. It improves strength, power output, and muscle hydration, and emerging evidence suggests neuroprotective benefits.
Testosterone optimization, as discussed above, supports muscle maintenance and growth. GH assessment is relevant in cases of severe sarcopenia with documented deficiency.
Men are roughly four times more likely to die by suicide than women, yet far less likely to seek help for depression, anxiety, or cognitive decline. This is a public health crisis that the medical profession has been slow to address.
At St. George Hospital, we approach men’s mental health from a physiological foundation. Testosterone deficiency is strongly associated with depressive symptoms, irritability, and cognitive decline — and in many cases, hormone optimization produces meaningful improvement in mood and mental clarity without the need for antidepressant medication. This is not to say that all male depression is hormonal. But the hormonal axis should be evaluated before or alongside psychological treatment.
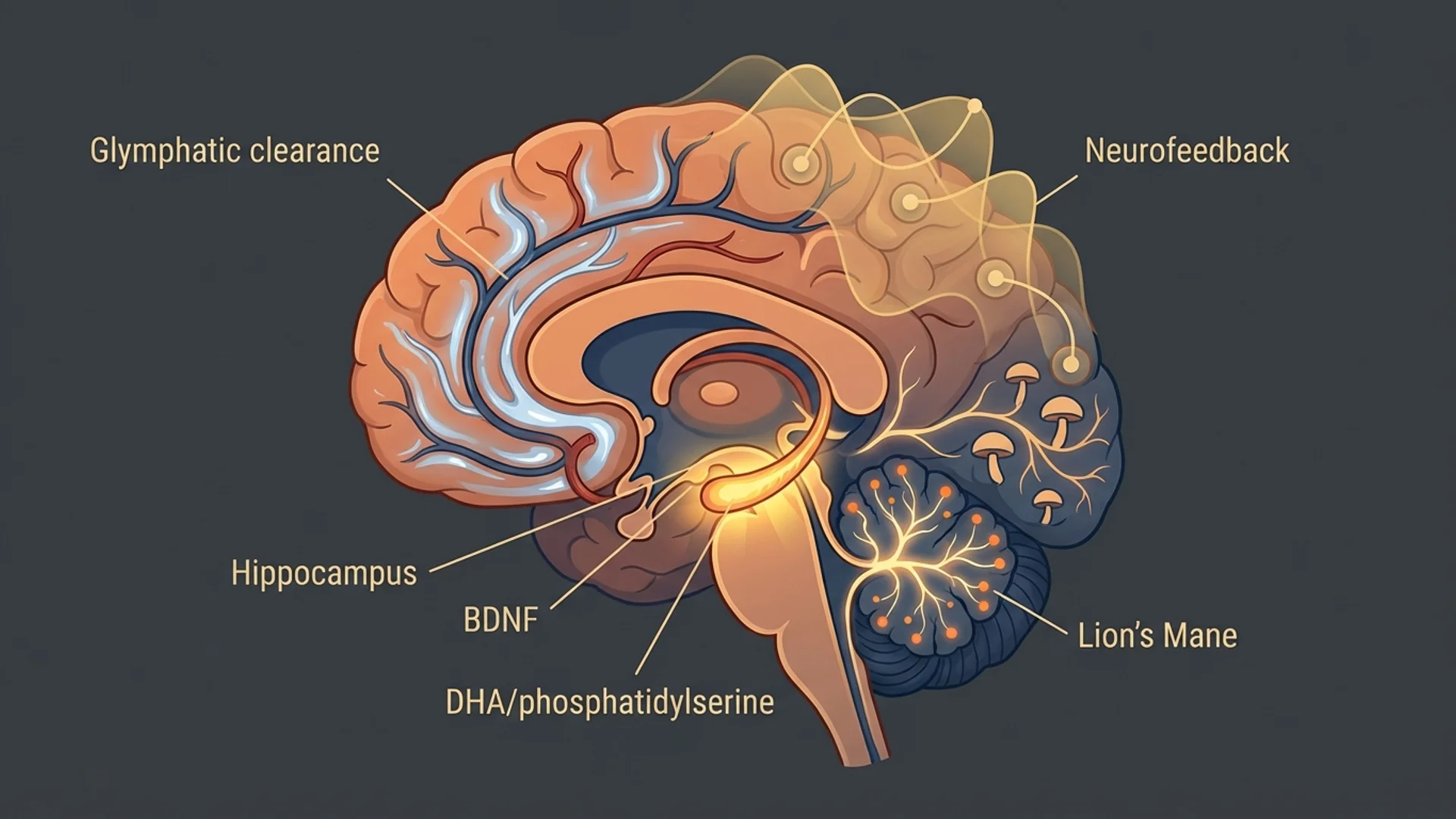
We also offer neurofeedback training, a non-invasive technique that uses real-time EEG feedback to help patients improve brainwave regulation. Neurofeedback has a growing evidence base for attention, executive function, stress resilience, and sleep quality. For men who are reluctant to engage with traditional therapy, neurofeedback offers a technology-based entry point into brain health optimization.
Cognitive performance — memory, processing speed, executive function — is also addressed through cardiovascular optimization (the brain depends on vascular health), sleep improvement, targeted supplementation (omega-3 fatty acids, phosphatidylserine, lion’s mane extract in appropriate cases), and metabolic optimization.
For men who are interested not only in treating current symptoms but in optimizing long-term healthspan, we offer evidence-based longevity-focused assessments and interventions.
Exercise programming: A combination of resistance training, zone 2 cardiovascular training (3-4 hours weekly), and VO2 max efforts has the strongest evidence base for all-cause mortality reduction. We provide exercise prescriptions based on current fitness testing and goals.
Metabolic health: Fasting insulin, HbA1c, continuous glucose monitoring data, and HOMA-IR assessment guide dietary and lifestyle recommendations. Metabolic health is arguably the most modifiable determinant of healthspan.
Targeted supplementation: Based on individual lab results, we may recommend specific evidence-supported supplements: vitamin D (titrated to 40-60 ng/mL), magnesium, omega-3 fatty acids, creatine, and others as indicated by testing. We do not recommend large, untargeted supplement regimens.
Sleep optimization: Sleep is the foundation of recovery, hormone production, cognitive function, and immune health. We assess and optimize sleep architecture through a combination of behavioral strategies, environmental modifications, and targeted interventions.
Our men’s health program is structured as a comprehensive evaluation and treatment program. It begins with an extensive initial consultation and laboratory workup, followed by a personalized treatment plan that addresses the specific areas where intervention will have the greatest impact.
We see men at every stage: those in their 40s who want to optimize proactively, those in their 50s and 60s dealing with hormone decline and emerging health concerns, and those at any age who have specific complaints — fatigue, sexual dysfunction, cognitive decline, body composition changes — that deserve thorough investigation.
What distinguishes our approach is the integration of endocrinology, functional medicine, cardiovascular risk assessment, and performance optimization into a single, coherent program. Rather than seeing a urologist for prostate concerns, an endocrinologist for hormones, a cardiologist for heart risk, and a psychiatrist for mood, you work with a medical team that understands how these systems interconnect.
If you would like to learn more about our men’s health programs or discuss whether an evaluation would be appropriate for your situation, please contact our international patient team at info@clinicum-stgeorg.de or +49 (0)8061 398-0. Consultations can be arranged in person at our hospital in Bad Aibling, Germany, or as a preliminary remote consultation to determine next steps.
Your health is not a luxury. It is the foundation upon which everything else in your life depends. I encourage you to invest in understanding it.