One of the most confusing aspects of chronic infection treatment is that effective therapy can temporarily intensify symptoms. Patients begin antibiotics, feel significantly worse, and understandably question whether the treatment is helping or harming. Physicians unfamiliar with the phenomenon may interpret the worsening as treatment failure or an adverse drug reaction.
The Jarisch-Herxheimer reaction is neither of these. Understanding what it is, why it happens, and how to manage it is essential for anyone undergoing treatment for chronic tick-borne disease.
What the Herxheimer Reaction Is
The Jarisch-Herxheimer reaction was first described in the late 1800s in the context of syphilis treatment with mercury, and later with penicillin. Physicians observed that patients with syphilis often experienced an acute worsening of symptoms — fever, chills, hypotension, tachycardia, and exacerbation of existing lesions — within hours of beginning treatment [1].
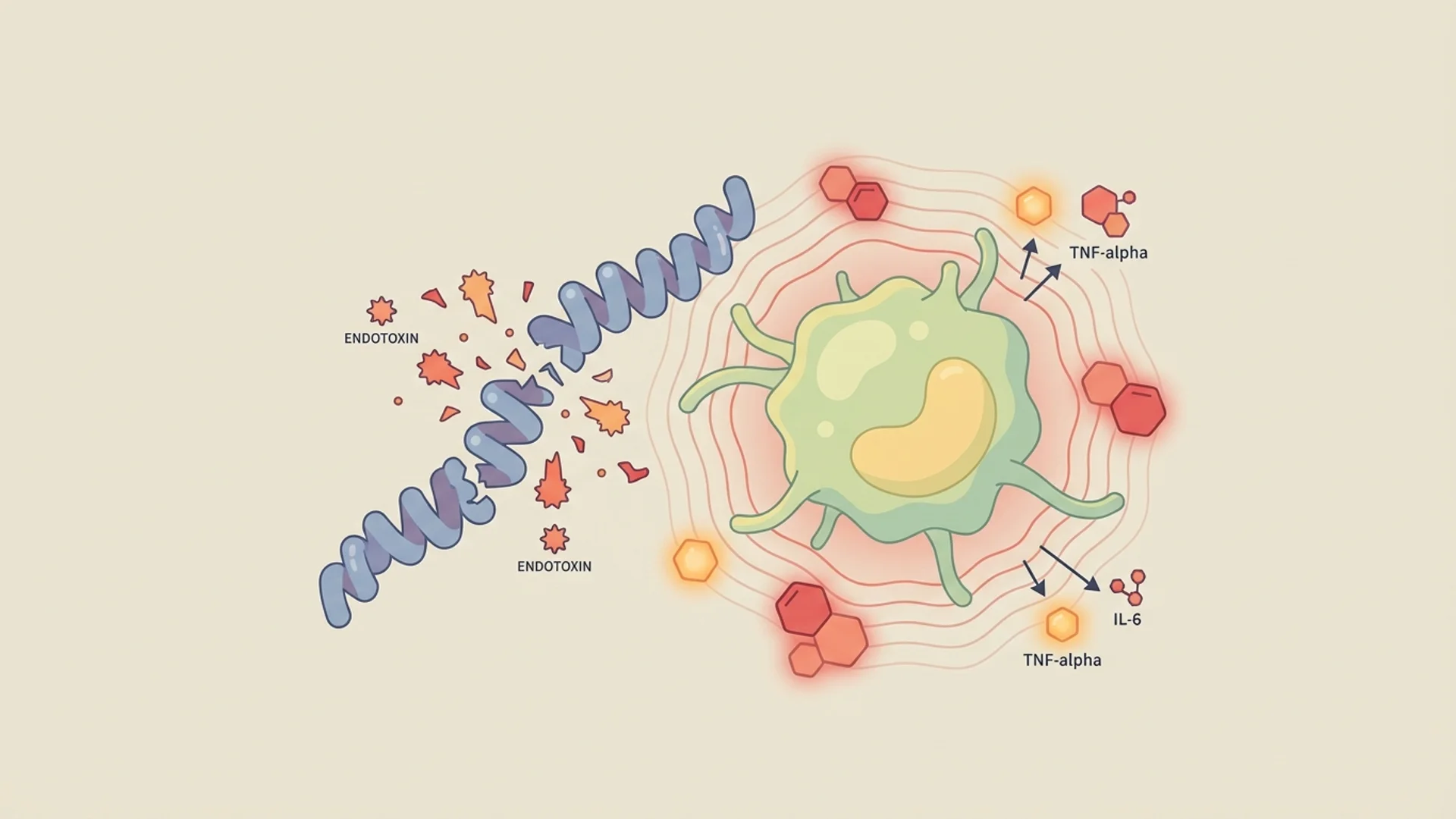
The mechanism is now understood to involve the rapid release of endotoxins, lipoproteins, and other microbial components when organisms are killed by antimicrobial therapy. This sudden release triggers a surge of pro-inflammatory cytokines — particularly TNF-alpha, IL-6, and IL-8 — producing what is essentially a systemic inflammatory flare.
In Lyme disease and other tick-borne infections, the Herxheimer reaction follows the same principle: as Borrelia, Bartonella, or other organisms are killed, their structural components flood the system, triggering an inflammatory response that can be more intense than the chronic symptoms the patient was experiencing before treatment.
What It Feels Like
Herxheimer reactions in chronic tick-borne disease can manifest as:
- Intensification of existing symptoms: Whatever the patient’s primary complaints — fatigue, joint pain, cognitive dysfunction, headache — may worsen
- Flu-like symptoms: Fever, chills, body aches, malaise
- Neurological symptoms: Increased brain fog, headache, dizziness, neuropathic pain
- Musculoskeletal: Joint and muscle pain, often migratory
- Gastrointestinal: Nausea, diarrhea, abdominal discomfort
- Neuropsychiatric: Increased anxiety, irritability, mood swings (particularly with Bartonella die-off)
- Skin: Rashes, flushing
- Cardiovascular: Heart palpitations, blood pressure fluctuations
The onset is typically within hours to days of starting or intensifying antimicrobial therapy. Reactions can last from hours to several weeks, depending on the pathogen burden, the speed of kill, and the patient’s detoxification capacity.
Herxheimer vs. Adverse Drug Reaction: How to Tell
This is a critical clinical distinction. Both Herxheimer reactions and adverse drug reactions occur after starting medication. The differentiating features:
Herxheimer reaction:
- Symptoms resemble an exacerbation of the patient’s existing complaints
- Onset within hours to days of treatment initiation
- Often fluctuating — better on some days, worse on others
- May correlate with the timing of antibiotic doses
- Improves over time with continued treatment
- Can sometimes be provoked or intensified by biofilm-disrupting agents (suggesting pathogen release)
Adverse drug reaction:
- New symptoms not previously experienced (rash, hives, organ-specific toxicity)
- May worsen continuously without fluctuation
- Does not improve with continued treatment
- Resolves when the medication is stopped
When the distinction is unclear, I err on the side of caution. Pausing the medication for a few days can be informative: if symptoms resolve, it may be an adverse reaction; if symptoms fluctuate regardless of medication status, a Herxheimer reaction is more likely.
Management Strategies
Reducing the Kill Rate
The most effective way to manage severe Herxheimer reactions is to slow the rate of pathogen killing. This can mean:
- Reducing antibiotic doses temporarily
- Spacing doses further apart
- Starting at very low doses and titrating up gradually (“start low, go slow”)
- Pulsing treatment (medication on some days, off others) to allow recovery between doses
Supporting Detoxification
The inflammatory load of a Herxheimer reaction is proportional to the body’s ability to process and eliminate the released microbial debris. Supporting detoxification includes:
- Adequate hydration — essential for renal elimination
- Glutathione support — oral liposomal glutathione (500-1,000 mg daily) or IV glutathione to support hepatic detoxification
- Binding agents — activated charcoal, chlorella, or cholestyramine to bind toxins in the gastrointestinal tract, taken at least two hours apart from medications
- Liver support — milk thistle (silymarin), NAC, alpha-lipoic acid
- Lymphatic support — gentle movement, dry brushing, lymphatic massage
- Alkalinization — adequate mineral intake, alkaline water or bicarbonate supplementation
Symptomatic Relief
- Anti-inflammatory support (curcumin, omega-3 fatty acids)
- Epsom salt baths (magnesium sulfate absorption, relaxation)
- Adequate rest — this is not the time to push through
- Gentle movement but not intense exercise
When to Seek Medical Attention
While most Herxheimer reactions are manageable, severe reactions require medical evaluation:
- High fever (above 39 degrees C / 102 degrees F)
- Significant hypotension
- Severe cardiac symptoms
- Severe neurological symptoms (seizures, altered consciousness)
- Respiratory distress
- Signs of anaphylaxis (rare, but possible)
The Clinical Perspective
In my experience, Herxheimer reactions are actually informative. A patient who experiences a clear Herxheimer reaction when starting treatment for a suspected chronic infection has, in effect, provided a therapeutic confirmation of the diagnosis. The reaction indicates that the antimicrobial is reaching and killing the target organism.
Patients who do not experience any Herxheimer reaction may have a lower pathogen burden, excellent detoxification capacity, or — in some cases — may not be infected with the suspected organism.
What I tell my patients: the Herxheimer reaction is uncomfortable but meaningful. It indicates that treatment is working. The goal is not to avoid it entirely but to manage it so that it remains tolerable while treatment progresses. This requires communication between patient and physician, willingness to adjust protocols, and patience.

References
- Butler T. The Jarisch-Herxheimer Reaction After Antibiotic Treatment of Spirochetal Infections: A Review of Recent Cases and Our Understanding of Pathogenesis. American Journal of Tropical Medicine and Hygiene. 2017;96(1):46-52.
This content is educational and does not constitute medical advice. Herxheimer reactions should be managed in consultation with the prescribing physician. Severe reactions require medical evaluation.