At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate |
| Primary Use | Symptom recognition and diagnostic guidance |
| Key Mechanism | Intraerythrocytic parasitemia causing hemolysis, autonomic dysregulation, and respiratory center signaling disruption |
Why Babesia Makes You Feel Like You Cannot Breathe
You are lying in bed at night, lungs clear, oxygen saturation reading 97%, and yet you cannot take a satisfying breath. You yawn repeatedly, trying to get that one deep inhale that feels complete — and it never comes. Your pulmonologist says your spirometry is normal. Your cardiologist says your heart is fine. But the sensation persists, sometimes for weeks or months.
This is air hunger. And if no one has tested you for Babesia, they may be missing the diagnosis.
Let me be direct: air hunger is the single most characteristic symptom of Babesia infection, and it is the symptom that most reliably distinguishes it from other tick-borne co-infections. In our clinical experience treating thousands of patients with tick-borne diseases, this symptom pattern — unexplained dyspnea with normal cardiopulmonary workup — is the clinical signal that sends us looking for Babesia.
What Babesia Actually Does to Your Blood
Babesia species — primarily Babesia microti in the northeastern United States and Babesia divergens in Europe — are intraerythrocytic parasites. That means they invade your red blood cells and reproduce inside them, much like malaria parasites do.
Here is the cascade that produces air hunger:
1. Red blood cell destruction (hemolysis)
As Babesia merozoites multiply inside red blood cells, they eventually rupture the cell to release new parasites. This ongoing hemolysis reduces the oxygen-carrying capacity of your blood. Even when parasitemia is low — sometimes below the detection threshold of a standard blood smear — the cumulative effect of ongoing red cell destruction creates a subtle but persistent oxygen delivery deficit [1].
2. Altered hemoglobin function
Parasitized red blood cells do not carry oxygen normally even before they lyse. The parasite’s metabolic activity within the erythrocyte alters hemoglobin’s oxygen-binding characteristics. Your pulse oximeter may read normally because it measures saturation of available hemoglobin, not the total oxygen delivery to tissues.
3. Autonomic dysregulation
Babesia infection triggers significant autonomic nervous system disruption. The inflammatory cytokine cascade — particularly elevated TNF-alpha and IL-6 — affects the brainstem respiratory centers that regulate the sensation of breathing satisfaction. This is why air hunger feels disproportionate to any measurable gas exchange abnormality. The respiratory drive signaling itself is dysregulated [2].
4. Microvasculature impairment
Parasitized erythrocytes are less deformable than healthy red blood cells. They do not flow smoothly through capillaries, creating microcirculatory impairment. This is the same mechanism that causes complications in malaria, and it means that even with adequate hemoglobin levels, oxygen delivery at the tissue level may be compromised.

Why Standard Testing Misses It
Here is what I tell my patients: the reason air hunger from Babesia is so often missed is that physicians are looking for the wrong things.
A standard workup for shortness of breath includes:
- Pulmonary function tests (normal in Babesia)
- Chest X-ray (normal in Babesia)
- Cardiac echocardiography (normal in Babesia)
- Pulse oximetry (often normal in Babesia)
- Complete blood count (may show mild anemia, but often within normal range)
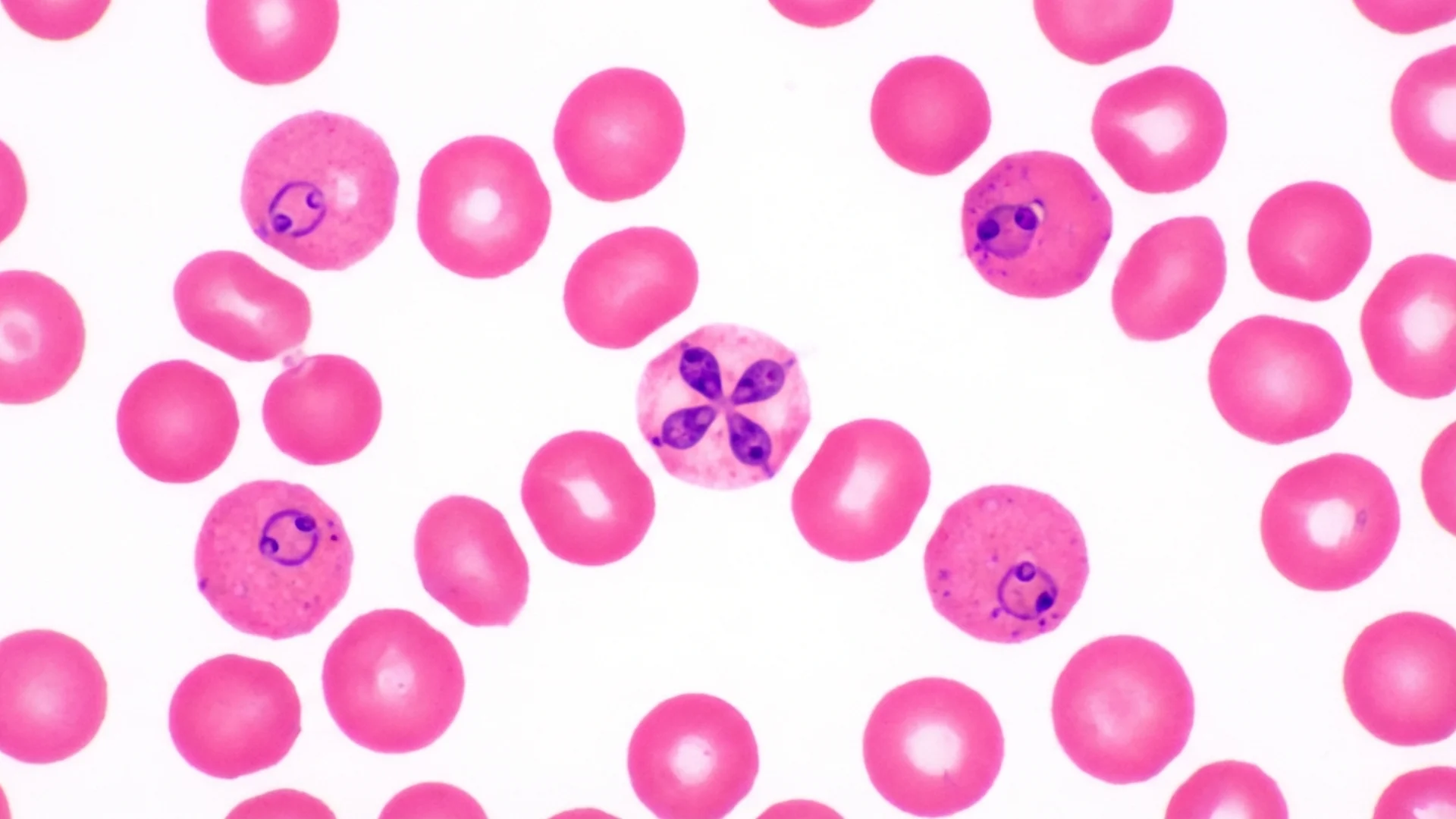
None of these will identify Babesia as the cause. The parasite load in chronic babesiosis is often too low to appear on a routine blood smear — the standard diagnostic method taught in medical school assumes the high parasitemia seen in acute cases.
What catches it:
- Babesia-specific PCR — detects parasite DNA even at low levels
- Babesia IgM and IgG antibodies — though seronegativity does not rule it out
- FISH (fluorescent in situ hybridization) — more sensitive than standard smear
- Clinical suspicion — in a patient with air hunger, night sweats, and a history of tick exposure or known Lyme disease, Babesia should be on the differential regardless of initial test results
In our clinical experience, approximately 30-40% of our chronic Lyme patients have evidence of Babesia co-infection. Among those with the specific complaint of air hunger, that percentage is significantly higher.
The Evidence
What We Know (Human Data)
The Jarisch-Herxheimer-like reactions and clinical presentations of babesiosis have been well-characterized in immunocompetent and immunocompromised populations. A seminal case series by Krause et al. documented that patients co-infected with Borrelia burgdorferi and Babesia microti experienced more severe and prolonged symptoms than those with either infection alone — including significantly more respiratory complaints [1].
Hemolytic anemia in babesiosis has been documented to range from subclinical to life-threatening. In immunocompromised patients, parasitemia can exceed 10% of red blood cells, but in chronic low-grade infection, parasitemia below 1% is common and easily missed on standard peripheral smear [3].
The autonomic dysfunction component has been less formally studied in Babesia-specific cohorts, but the inflammatory cytokine profiles documented in babesiosis (TNF-alpha, IL-1beta, IL-6 elevation) are known to directly affect brainstem respiratory center function [2].
What I See in Practice
In our clinical experience treating over 12,000 patients with tick-borne diseases since 1994, air hunger is the symptom that most reliably points to Babesia as a co-infection. It has a different quality than the dyspnea of cardiac or pulmonary disease — patients describe it as an unsatisfied breath, a need to yawn that never resolves, or a feeling of suffocation that occurs at rest.
What I observe in practice is that this symptom often responds rapidly once appropriate anti-Babesia therapy is initiated. Within the first one to two weeks of treatment, many patients report that the air hunger begins to lift — even before other symptoms improve. This rapid response to targeted therapy is itself a diagnostic clue.
I also observe that air hunger frequently worsens at night. Patients report it interfering with sleep — not because of sleep apnea, but because the sensation of incomplete breathing creates anxiety that prevents relaxation. This nocturnal pattern is consistent with the autonomic shifts that occur during parasympathetic predominance in sleep.

Practical Application
When to Suspect Babesia-Related Air Hunger
Consider Babesia if:
- Air hunger is present with a normal cardiopulmonary workup
- There is a history of tick exposure, known Lyme disease, or co-infection
- Night sweats accompany the air hunger (particularly drenching sweats)
- Fatigue is disproportionate to any identifiable cause
- Symptoms are cyclical — worsening every 2-4 days (reflecting parasite reproductive cycles)
Testing to Request
- Babesia microti IgM and IgG (and Babesia duncani if West Coast exposure)
- Babesia PCR (blood)
- Babesia FISH assay
- CBC with reticulocyte count (look for subtle hemolysis)
- Haptoglobin and LDH (hemolysis markers)
- Peripheral blood smear with specific request for Babesia evaluation
Treatment That Addresses Air Hunger
Standard first-line therapy for Babesia is atovaquone plus azithromycin. For treatment-resistant cases, combination protocols involving clindamycin plus quinine, or herbal adjuncts such as Cryptolepis sanguinolenta and Artemisia annua, may be considered under physician supervision.
In our clinical experience, whole-body hyperthermia has shown particular promise as an adjunctive therapy for patients with persistent babesiosis. The thermal sensitivity of Babesia — like its relative the malaria parasite — makes hyperthermia a logical addition to antimicrobial protocols.
Safety and Considerations
- Air hunger can also be a symptom of anxiety, hyperventilation syndrome, cardiac disease, or pulmonary embolism. Always ensure appropriate cardiopulmonary workup before attributing the symptom to Babesia.
- Babesia can be severe or fatal in asplenic patients, elderly individuals, and immunocompromised patients. These populations require urgent management.
- Treatment can trigger Herxheimer-like reactions. Managing die-off reactions requires clinical guidance.
- Self-treatment is not recommended. Babesia requires prescription antimicrobials under physician monitoring.
The Bottom Line
Air hunger is Babesia’s calling card. If you have unexplained shortness of breath that does not match any cardiopulmonary diagnosis, especially in the context of tick exposure or known Lyme disease, Babesia co-infection should be on the diagnostic radar. The nuance matters — this is not simple shortness of breath, it is a specific, recognizable pattern that responds to targeted therapy.
References
- Krause PJ, Telford SR, Spielman A, et al. Concurrent Lyme disease and babesiosis: evidence for increased severity and duration of illness. JAMA. 1996;275(21):1657-1660. PMID: 8637139
- Hemmer RM, Ferrick DA, Conrad PA. Role of T cells and cytokines in fatal and resolving experimental babesiosis. Infect Immun. 2000;68(4):1875-1882. PMID: 10722576
- Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366(25):2397-2407. PMID: 22716978
- Krause PJ, Auwaerter PG, Bannuru RR, et al. Clinical Practice Guidelines by the Infectious Diseases Society of America: 2020 Guideline on Diagnosis and Management of Babesiosis. Clin Infect Dis. 2021;72(2):e49-e64. PMID: 33252652