Hormonal assessment is one of the areas where the gap between standard medical practice and functional medicine is widest. Standard practice often checks one or two hormones in isolation — TSH for thyroid, total testosterone for male hormone health. Functional assessment checks the complete hormonal picture, including metabolites, binding proteins, and circadian patterns.
The difference in clinical utility is significant. Let me walk through what a comprehensive hormonal evaluation includes and why it matters.
Thyroid: Beyond TSH
I have written about this elsewhere, but it bears repeating: TSH alone is an insufficient thyroid assessment. A complete thyroid panel includes:
Marker What It Measures Optimal Range
Free T4 Active thyroid prohormone 1.0-1.5 ng/dL
Free T3 Active thyroid hormone 3.0-4.0 pg/mL
Reverse T3 Inactive T4 metabolite Below 15 ng/dL
Anti-TPO Autoimmune thyroid marker Below 9 IU/mL
Anti-TG Autoimmune thyroid marker Below 4 IU/mL
Common patterns missed by TSH-only screening:
- Poor T4-to-T3 conversion: Normal TSH, normal free T4, low free T3. The patient has adequate thyroid hormone production but is not converting T4 to the active T3 form. Common causes: nutrient deficiency (selenium, zinc, iron), chronic inflammation, and stress.
- Elevated reverse T3: The body converts T4 to reverse T3 (inactive) instead of T3 (active). This is a stress response — it conserves metabolic energy during illness, caloric restriction, or chronic stress. The patient may have “normal” TSH and free T4 but is functionally hypothyroid.
- Hashimoto’s thyroiditis: Elevated anti-TPO antibodies indicate autoimmune thyroid destruction. TSH may be normal for years before it rises above the reference range, while the autoimmune process is already active and potentially addressable.
Sex Hormones
For Men
Marker What It Measures Optimal Range (adult male)
Free testosterone Biologically active fraction 15-25 pg/mL
SHBG Sex hormone binding globulin 20-40 nmol/L
Estradiol (E2) Primary estrogen 20-35 pg/mL
DHEA-S Adrenal androgen precursor 250-500 mcg/dL
Prolactin Pituitary hormone Below 15 ng/mL
LH / FSH Pituitary gonadotropins Contextual
Why total testosterone alone is insufficient: SHBG binds testosterone, making it biologically unavailable. A man with total testosterone of 600 ng/dL and an SHBG of 60 nmol/L has significantly less bioavailable testosterone than a man with the same total testosterone and an SHBG of 25 nmol/L. Free testosterone and SHBG complete the picture.
Estradiol in men: Often overlooked but clinically important. Excessive aromatase conversion of testosterone to estradiol can produce symptoms of estrogen excess (gynecomastia, water retention, mood changes) even when testosterone levels are normal. Elevated estradiol relative to testosterone also increases cardiovascular risk.
For Women
Hormonal assessment in women must account for the menstrual cycle:
- Follicular phase (days 2-5): optimal for baseline FSH, LH, estradiol, and AMH
- Mid-luteal phase (day 19-22): optimal for progesterone assessment
- Any time: DHEA-S, testosterone, SHBG, thyroid
Low progesterone relative to estradiol (“estrogen dominance”) is one of the most common hormonal imbalances I see in women of reproductive age. It manifests as PMS, heavy periods, breast tenderness, anxiety, and sleep disruption. Standard testing often misses it because progesterone is not measured or is measured at the wrong point in the cycle.
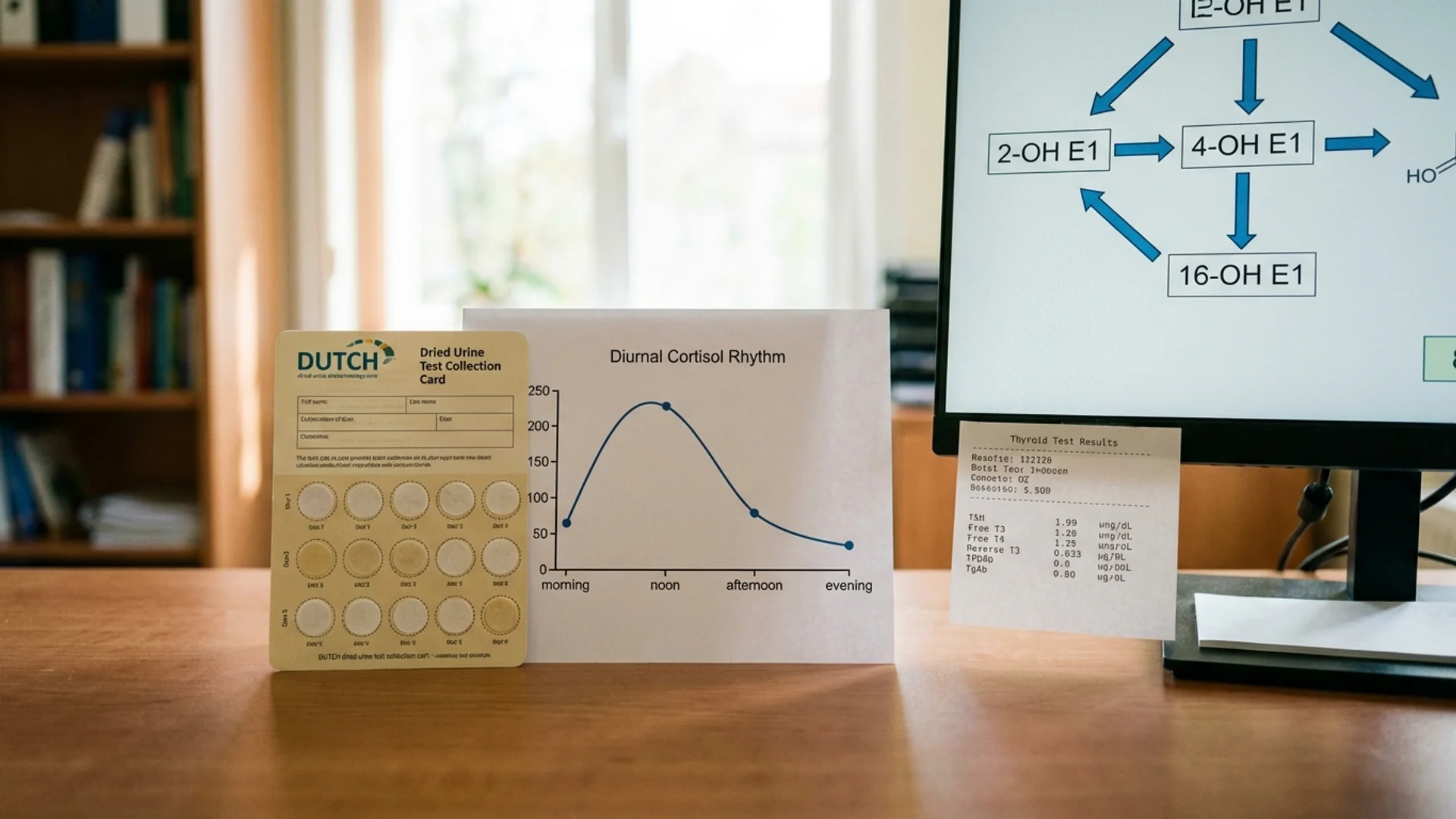
Cortisol: The Rhythm Matters
Cortisol follows a circadian rhythm — highest in the morning (cortisol awakening response), declining throughout the day, lowest at midnight. A single morning serum cortisol measurement tells you only one point on this curve.
The DUTCH Test (Dried Urine Test for Comprehensive Hormones)
The DUTCH test measures cortisol and cortisol metabolites from dried urine samples collected at four time points throughout the day. It provides:
- Free cortisol pattern — morning, midday, evening, night
- Cortisol metabolites — total cortisol production (which can be normal even when free cortisol is low, or vice versa)
- Cortisone — the inactive form, revealing cortisol-cortisone interconversion
- Sex hormone metabolites — estrogen, progesterone, and testosterone metabolic pathways
Clinical patterns:
- Flat cortisol curve (low morning, relatively unchanged throughout the day) — suggests HPA axis dysfunction, often seen in chronic fatigue and burnout
- Elevated evening cortisol — suggests chronic stress, contributes to insomnia
- High total cortisol production with normal free cortisol — suggests high cortisol clearance, often missed by standard testing
Salivary Cortisol
A four-point salivary cortisol panel (morning, midday, evening, bedtime) is a more accessible alternative to DUTCH for assessing cortisol rhythm. It does not provide metabolite data but gives a clinically useful picture of the cortisol curve.
Evidence level for salivary cortisol in HPA axis assessment: strong (used in endocrinology research and clinical practice).
Insulin and Metabolic Hormones
Fasting insulin is the most important metabolic marker that standard panels omit. Optimal fasting insulin is 3-8 mIU/L. Above 10 mIU/L indicates insulin resistance. HOMA-IR (calculated from fasting glucose and insulin) provides a standardized measure.
Leptin — the satiety hormone produced by adipose tissue. Elevated leptin with persistent hunger suggests leptin resistance, a pattern common in obesity and metabolic syndrome.
IGF-1 — a downstream marker of growth hormone activity. Age-appropriate IGF-1 levels reflect growth hormone axis function without requiring provocative testing.
When to Test
Morning fasting blood draw (before 10:00 AM) is optimal for most hormones, particularly cortisol, testosterone, and metabolic markers.
Consistent timing between tests is essential for meaningful comparison. A testosterone drawn at 7:00 AM is not comparable to one drawn at 3:00 PM (testosterone has a diurnal variation of 25-40%).
Menstrual cycle timing for women, as described above.
Repeat testing at 6-12 week intervals to assess treatment response. Hormonal interventions take time to produce measurable changes, and testing too frequently leads to premature protocol adjustments.
The Interpretation Framework
Hormone results must be interpreted in clinical context, not in isolation. A testosterone level of 450 ng/dL is “normal” by reference range standards, but in a 35-year-old man with fatigue, reduced libido, and difficulty maintaining muscle mass, it may be suboptimal. The same level in a 70-year-old man with no symptoms may be entirely adequate.
What I tell my patients: hormones are a system, not a collection of individual numbers. The relationships between hormones — testosterone to estradiol, cortisol to DHEA, T3 to reverse T3 — are often more informative than any single value. This is why comprehensive testing, not isolated markers, is the standard in my practice.
Disclaimer: This article is provided for educational purposes and reflects one physician’s clinical perspective. It is not a substitute for individualized medical care. Hormone testing and therapy should be supervised by a qualified physician.
