
Featured
Magnesium: 7 Forms Compared — Which One Do You Need?
Magnesium glycinate vs threonate vs taurate and 4 more forms compared. Dosing, deficiency signs, and why serum testing is unreliable. A physician's guide.
Condition
Mitochondrial dysfunction, immune exhaustion, and evidence-based treatment for ME/CFS and persistent fatigue. An integrative approach addressing root causes, not just symptoms.
A physician's complete guide to chronic fatigue syndrome. Mitochondrial dysfunction, immune dysregulation, diagnostic criteria, and the stepwise treatment approach we use at Klinik St. Georg.

How to read a lymphocyte subset panel. What CD4, CD8, CD19, and CD56 cells do, what abnormal ratios mean in chronic illness, and when this test changes your treatment.

Understanding low natural killer cell function in chronic illness. What NK cells do, why function drops, how to test, and evidence-based strategies to restore immune surveillance.

Complete guide to the Organic Acids Test. What the 70+ markers mean, what OAT reveals about mitochondrial function, neurotransmitters, and gut health, and when to order it.
Why Epstein-Barr virus reactivates in chronic illness, how it drives fatigue and immune dysfunction, and what treatment options exist for reactivated EBV.
Evidence-based protocol to increase deep sleep and slow-wave sleep. Temperature, light, exercise timing, supplements, and what actually works according to sleep research.
NAD+ IV, NMN, and NR compared by a physician. Bioavailability, evidence, cost, and who benefits from which approach based on clinical experience.
Physician guide to sleep stages, deep sleep and REM targets by age, and what your sleep tracker data actually means for longevity and cognitive health.
Physician-ranked guide to sleep supplements. Magnesium glycinate, glycine, apigenin, L-theanine, and ashwagandha compared by evidence quality for deep sleep enhancement.
Why Zone 2 cardio is the single most important exercise modality for longevity. Mitochondrial biogenesis, fat oxidation, VO2 max, and practical programming.

Brain fog treatment options from neuroinflammation workup to neuromodulation. Causes include post-COVID, Lyme, MCAS, and mold. TPS, NAD+, and hyperbaric oxygen covered.

What to expect during brain fog recovery after Lyme treatment — the multi-system recovery approach, realistic timelines, and evidence-based strategies.
What causes brain fog in Lyme disease — Johns Hopkins PET scan findings showing glial activation, neuroinflammation mechanisms, and treatment implications.

How neurofeedback retrains dysregulated brainwave patterns in Lyme disease patients. qEEG findings, clinical evidence, and what to expect from treatment.

Clear comparison of neurofeedback and biofeedback. What each measures, how they work, conditions they treat, and how to choose the right one for your situation.

When to get neuropsychological testing for brain fog. What the evaluation measures, how it differs from standard neurology exams, and what the results mean for treatment.
How photobiomodulation targets mitochondrial dysfunction to clear brain fog. Mechanism, clinical evidence, and practical application for chronic illness patients.
Evidence-based review of transcranial photobiomodulation for brain health. Wavelengths, mechanisms, clinical trial data, and what I see in practice.

Complete guide to quantitative EEG brain mapping. What the test measures, how it identifies brain dysregulation, and why it matters for neurofeedback and brain fog treatment.

How vagus nerve stimulation restores autonomic balance in chronic fatigue and POTS — the cholinergic anti-inflammatory pathway, clinical evidence, and treatment options.
Evidence-based DSIP dosing guide for sleep. Subcutaneous protocols, timing, cycling, and realistic expectations from Dr. Julian Douwes.

DSIP vs melatonin comparison by Dr. Julian Douwes. Sleep architecture modulation vs circadian timing — mechanisms, evidence levels, and when to use each.
Evidence-based guide to CoQ10 supplementation. Ubiquinol vs ubiquinone, absorption differences, statin interactions, mitochondrial function, and what I recommend in clinical practice.
Physician guide to CoQ10 dosing by condition. Ubiquinol vs ubiquinone, heart health, male fertility, migraine prevention, energy, and statin users. Evidence-based protocols.
Physician guide to CoQ10 depletion from statins. Why it happens, symptoms of statin-induced CoQ10 deficiency, optimal dosing with ubiquinol, and what the evidence shows.

Physician comparison of magnesium glycinate vs magnesium L-threonate. Which form for sleep, which for cognition, absorption differences, dosing, and evidence quality.

Physician guide to magnesium supplement timing. When to take glycinate, threonate, citrate, and other forms for maximum absorption and effect. Morning vs night, food interactions.
Why COVID-19 causes persistent cognitive dysfunction and what can be done about it. Mechanisms, assessment, and treatment strategies.

How IHHT simulates altitude training to improve mitochondrial function. Evidence, protocols, and clinical applications.
Why mitochondrial dysfunction underlies fatigue, cognitive decline, and aging. Testing, treatment, and what actually improves mitochondrial function.
How NAD+ IV therapy supports mitochondrial function and cellular repair. Evidence, clinical experience, and what patients should know.
How sleep stages affect aging, recovery, and healthspan. Optimization strategies grounded in evidence and clinical experience.

Evidence-based strategies for improving sleep quality -- environment, timing, supplements, and habits. By Dr. Julian Douwes.
Schedule a consultation to discuss your case with Dr. Julian Douwes and the clinical team at St. George Hospital.
Complete Guide
In-depth reference by Dr. Julian Douwes
I want to begin with something that should not need saying in 2026, but unfortunately still does: Chronic Fatigue Syndrome, or Myalgic Encephalomyelitis (ME/CFS), is a real, measurable, biological disease. It is not depression. It is not laziness. It is not “all in your head.”
The World Health Organization has classified ME/CFS as a neurological disease since 1969 (ICD-10 G93.3). The US Institute of Medicine published a landmark report in 2015 confirming it as a serious, chronic, complex systemic disease. And yet, many patients who walk through our doors at St. George Hospital in Bad Aibling have spent years — sometimes decades — being told by physicians that nothing is wrong with them.
I find this unacceptable. When we run the right tests, we find measurable abnormalities in nearly every patient: disrupted immune markers, impaired mitochondrial function, abnormal organic acid profiles, reactivated viral infections, dysregulated cortisol rhythms. The evidence is there. The problem has been that most conventional medicine does not look for it.
The fatigue in ME/CFS is qualitatively different from ordinary tiredness. My patients describe it as a profound, bone-deep exhaustion that does not improve with rest. Many wake up feeling as though they have not slept at all, regardless of how many hours they were in bed. Cognitive function deteriorates — patients use the term “brain fog,” but what they are describing is measurable impairment in processing speed, working memory, and concentration.
The hallmark feature is post-exertional malaise (PEM): a disproportionate worsening of symptoms after physical or cognitive exertion. A patient might manage a short walk one day and spend the next three days in bed. This is not deconditioning. It is a failure of cellular energy production, and it is one of the most important clinical features that distinguishes ME/CFS from depression or simple fatigue.
Other common symptoms include orthostatic intolerance (difficulty standing), muscle pain, headaches, sore throat, tender lymph nodes, and new food sensitivities. The severity varies enormously — some patients maintain partial function, while others are bedbound.
At St. George Hospital, we do not treat chronic fatigue as a single disease with a single cause. We treat it as a syndrome — a convergence of multiple dysfunctions that collectively overwhelm the body’s capacity to produce and regulate energy. Our diagnostic workup is designed to identify which of these mechanisms are active in each individual patient.
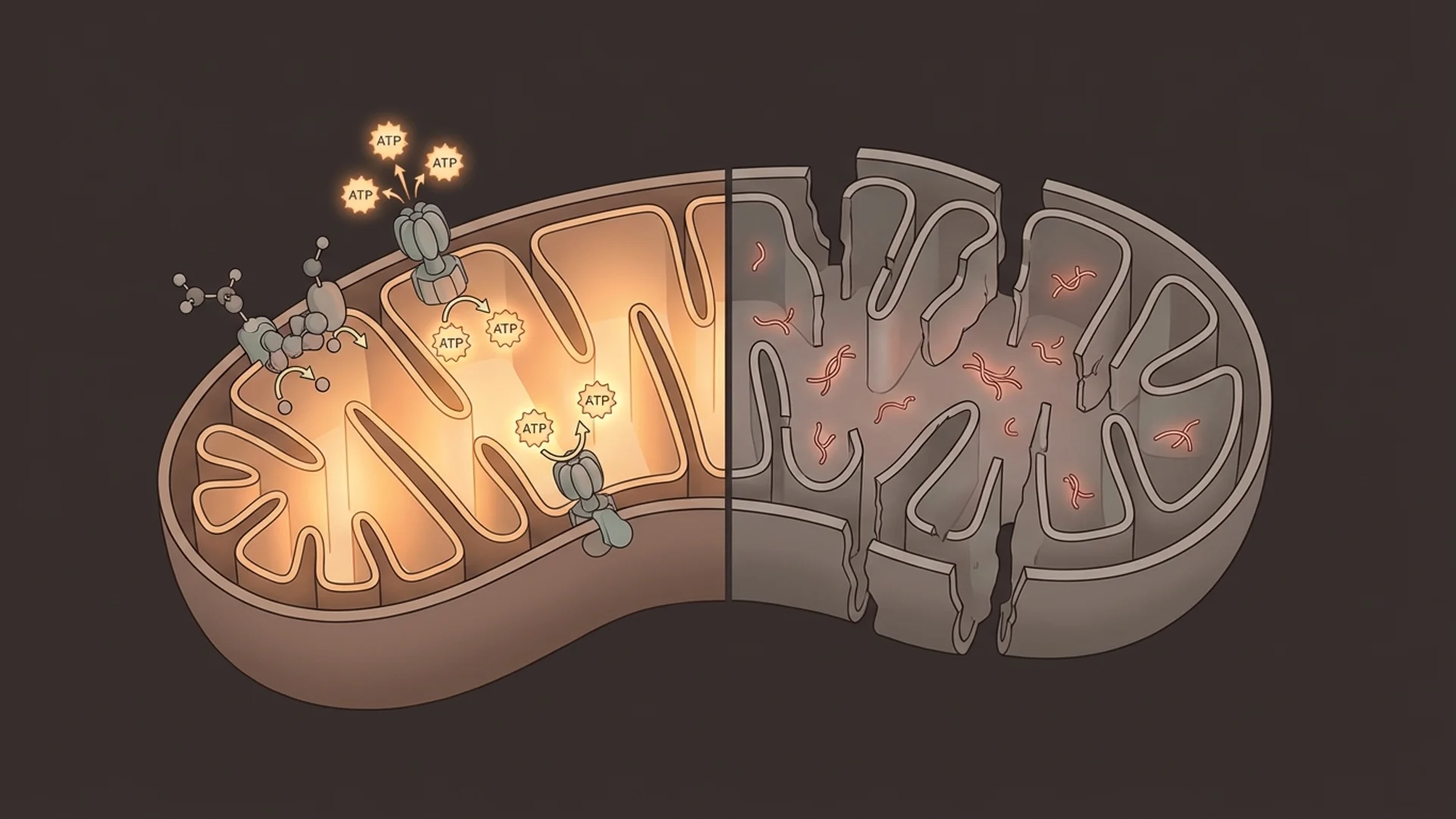
Mitochondria are the energy factories of every cell in your body. They convert nutrients and oxygen into adenosine triphosphate (ATP), the molecule that powers virtually every biological process. In ME/CFS patients, multiple studies have demonstrated that this process is impaired.
We see reduced activity in mitochondrial enzyme complexes, elevated lactate-to-pyruvate ratios, depleted coenzyme Q10, and low NAD+ levels. The organic acids test often reveals a metabolic profile consistent with mitochondrial dysfunction: elevated succinic acid, elevated suberic acid, and abnormal citric acid cycle intermediates.
The practical consequence is straightforward: when your cells cannot produce sufficient ATP, everything slows down. Muscles fatigue rapidly. The brain, one of the most energy-hungry organs, loses processing capacity. The immune system, which requires enormous energy to function, becomes dysregulated. Understanding this mechanism is central to our treatment approach.
The immune system in ME/CFS is not simply “weak” — it is chronically activated in an unproductive way. We consistently find elevated inflammatory cytokines, altered natural killer (NK) cell function, and shifts in T-cell subsets that suggest the immune system is locked in a state of persistent, low-grade activation.
This chronic immune activation is enormously energy-expensive. The immune system, when fully engaged, can consume up to 25-30% of basal metabolic energy. In ME/CFS, the immune system appears to be running at high alert without ever resolving the threat it perceives. The result is an energy drain that compounds the mitochondrial dysfunction.
We measure this through comprehensive immune panels including NK cell activity, CD4/CD8 ratios, cytokine profiles (TNF-alpha, IL-6, IL-1beta, IFN-gamma), and immunoglobulin levels. These results guide our immunomodulatory treatment strategies.
A significant proportion of our ME/CFS patients have identifiable chronic infections that are either triggering or perpetuating their symptoms. Epstein-Barr virus (EBV) reactivation is the most common — we see elevated early antigen (EA) antibodies indicating active viral replication in patients whose primary infection may have occurred decades ago.
Other infections we screen for include Mycoplasma pneumoniae, Chlamydia pneumoniae, HHV-6, Cytomegalovirus, and Borrelia burgdorferi (Lyme disease) along with its common co-infections. Many patients carry multiple concurrent infections, each contributing to immune activation and energy depletion.
I want to be clear: not every ME/CFS patient has an identifiable infection, and eradicating an infection does not always resolve the fatigue. The relationship is complex. But when we find active infections, addressing them is often a necessary step in recovery.
The hypothalamic-pituitary-adrenal (HPA) axis governs the body’s stress response, and it is frequently disrupted in ME/CFS. We do not see the dramatic cortisol deficiency of Addison’s disease, but rather a flattened diurnal cortisol curve — the normal morning peak is blunted, and cortisol levels may be inappropriately low throughout the day.
This manifests as difficulty waking, inability to handle stress, orthostatic intolerance, and worsening of symptoms during periods of physical or emotional demand. We assess this through four-point salivary cortisol testing along with DHEA-S levels, which together give us a picture of adrenal reserve and HPA axis integrity.
The gut contains approximately 70% of the body’s immune tissue, and we increasingly recognize that intestinal dysfunction plays a significant role in ME/CFS. Increased intestinal permeability (“leaky gut”), dysbiosis, small intestinal bacterial overgrowth (SIBO), and reduced secretory IgA are common findings.
When the gut barrier is compromised, bacterial endotoxins (lipopolysaccharides) enter the bloodstream and trigger systemic immune activation — adding fuel to the already overactive immune response. We assess gut function through comprehensive stool analysis, zonulin levels, breath testing for SIBO, and food sensitivity panels.
Many ME/CFS patients have measurable dysfunction of the autonomic nervous system, which controls heart rate, blood pressure, digestion, and temperature regulation. This manifests as postural orthostatic tachycardia syndrome (POTS), neurally mediated hypotension, temperature dysregulation, and abnormal sweating patterns.
Autonomic dysfunction contributes directly to fatigue through impaired cerebral blood flow — when blood pressure regulation fails, the brain receives insufficient oxygen and glucose, exacerbating cognitive symptoms.
When a patient comes to St. George Hospital with chronic fatigue, we conduct a thorough investigation that typically includes:
This is not a fishing expedition. Each test is targeted based on clinical presentation, and the results create an individualized map of dysfunction that guides treatment.
Our treatment approach is layered and sequential. We address the most fundamental dysfunctions first, then build on that foundation.
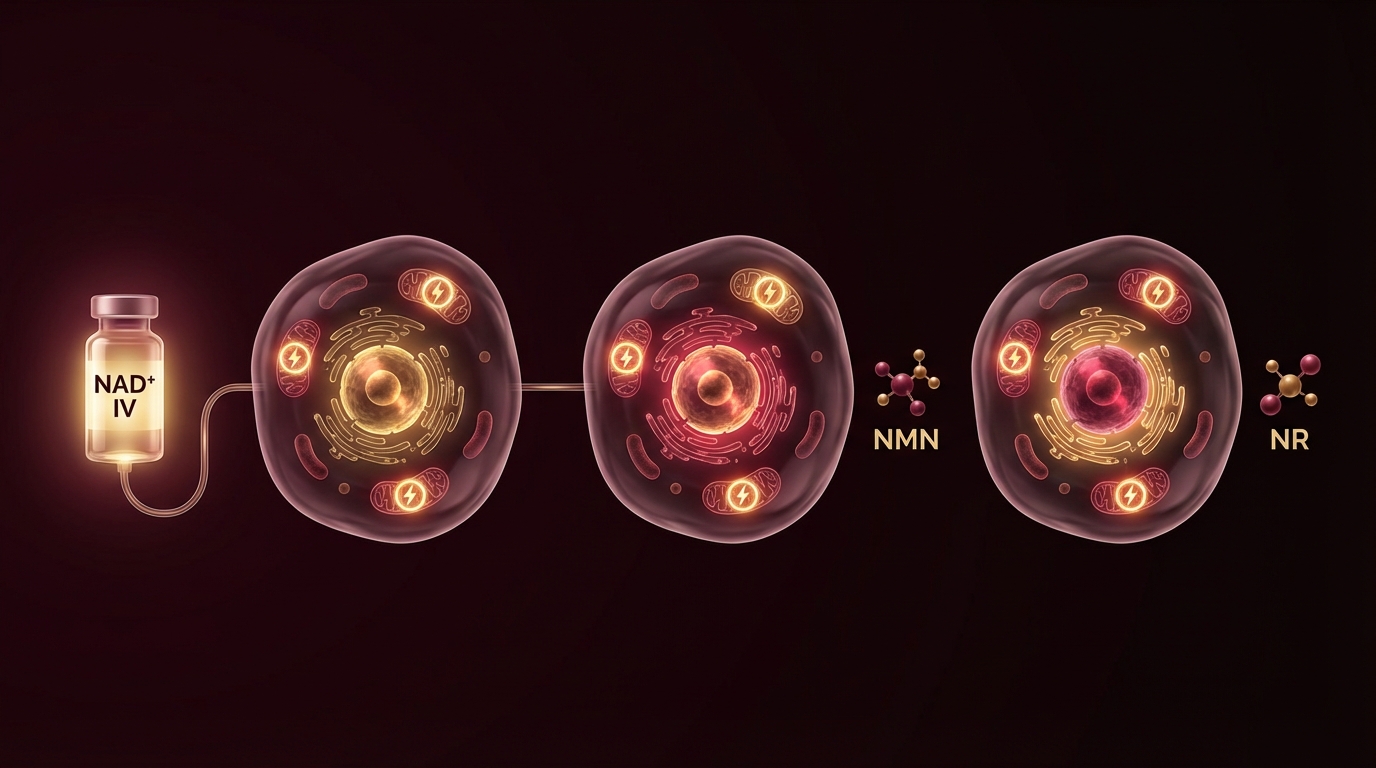
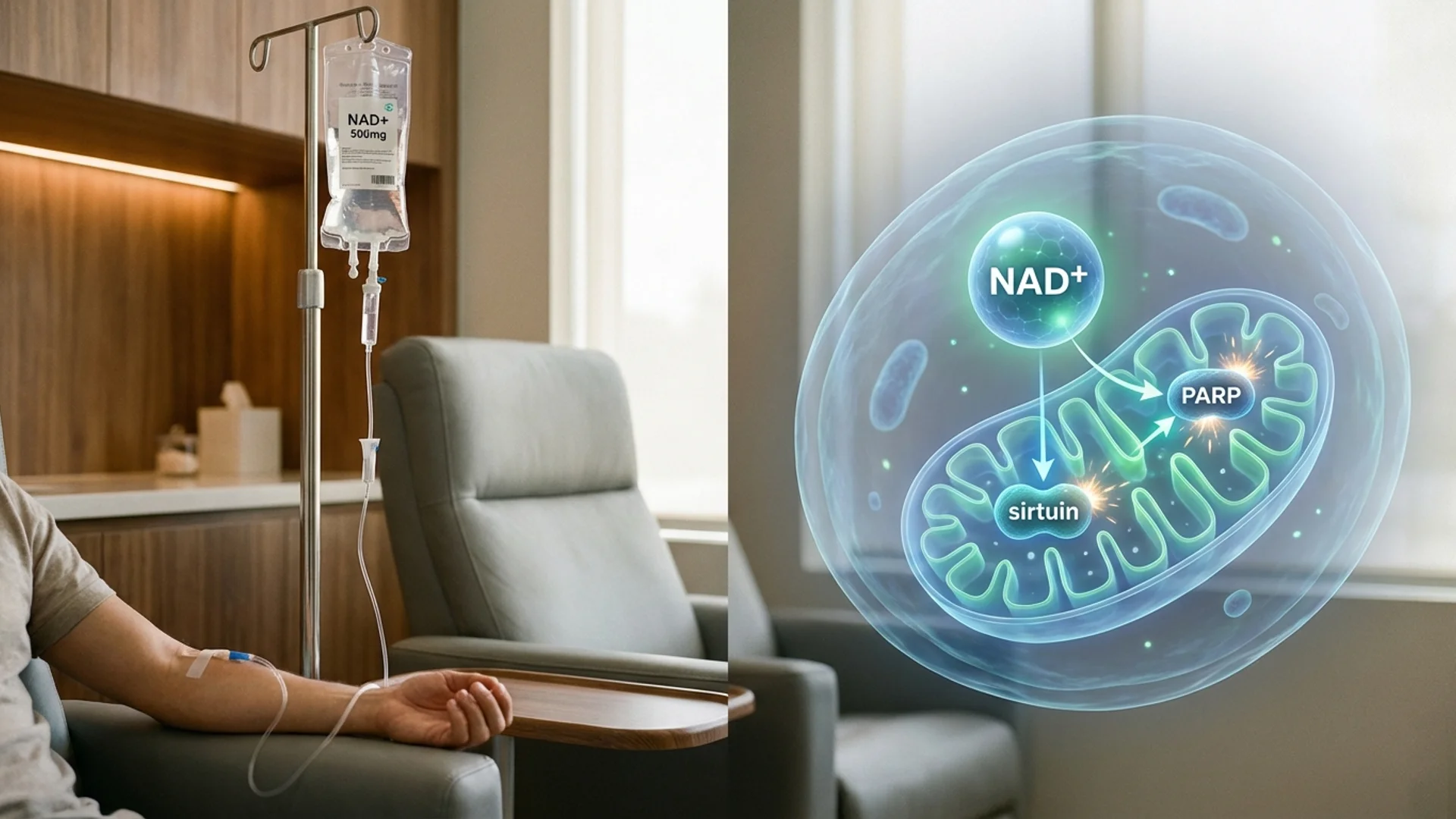
Nicotinamide adenine dinucleotide (NAD+) is a coenzyme essential for mitochondrial energy production. It declines with age and is often severely depleted in ME/CFS. We use intravenous NAD+ infusions to rapidly restore cellular levels, which many patients experience as a noticeable improvement in energy and cognitive clarity within days.
NAD+ IV therapy is not a cure. It is a tool to restore a depleted substrate while we address the underlying causes of depletion. We typically begin with a series of loading doses followed by maintenance infusions, adjusting frequency based on response.
IHHT, sometimes called altitude training, involves breathing alternating periods of low-oxygen and high-oxygen air while resting comfortably. This controlled hypoxic stimulus triggers mitochondrial biogenesis — the creation of new, healthy mitochondria — and promotes the elimination of damaged mitochondria through a process called mitophagy.
Over a typical course of 10-15 sessions, patients often experience progressive improvement in energy, exercise tolerance, and sleep quality. The evidence base for IHHT in chronic fatigue is growing, and we have seen consistently positive results in our clinical practice.
For patients with documented immune dysregulation, we use thymic peptide therapy to help restore balanced immune function. Thymic peptides support T-cell maturation and differentiation, helping to shift the immune system from its state of unproductive chronic activation toward a more regulated, effective response.
This is particularly valuable in patients with chronic viral reactivation, where improved immune surveillance can help bring latent infections under control.
When gut dysfunction is identified, we address it systematically: antimicrobial treatment for SIBO or dysbiosis where indicated, followed by a structured restoration protocol including mucosal healing nutrients (L-glutamine, zinc carnosine, butyrate), targeted probiotics, and dietary modifications to reduce inflammatory triggers.
For patients with flattened cortisol rhythms, we implement strategies to restore normal HPA axis function: adaptogenic herbs, phosphatidylserine for evening cortisol reduction, morning light exposure, and in some cases low-dose hydrocortisone on a temporary basis. Thyroid optimization is also critical — many ME/CFS patients have suboptimal free T3 levels even when TSH appears normal.
I want to address the question of exercise directly. The discredited PACE trial recommended graded exercise therapy (GET) as a treatment for ME/CFS. Subsequent analysis and patient evidence have made clear that pushing through PEM is harmful. We take a different approach: activity pacing within the patient’s current energy envelope, with gradual expansion only as mitochondrial function improves and biomarkers normalize. Exercise is medicine, but the dose must be appropriate to the patient’s capacity.
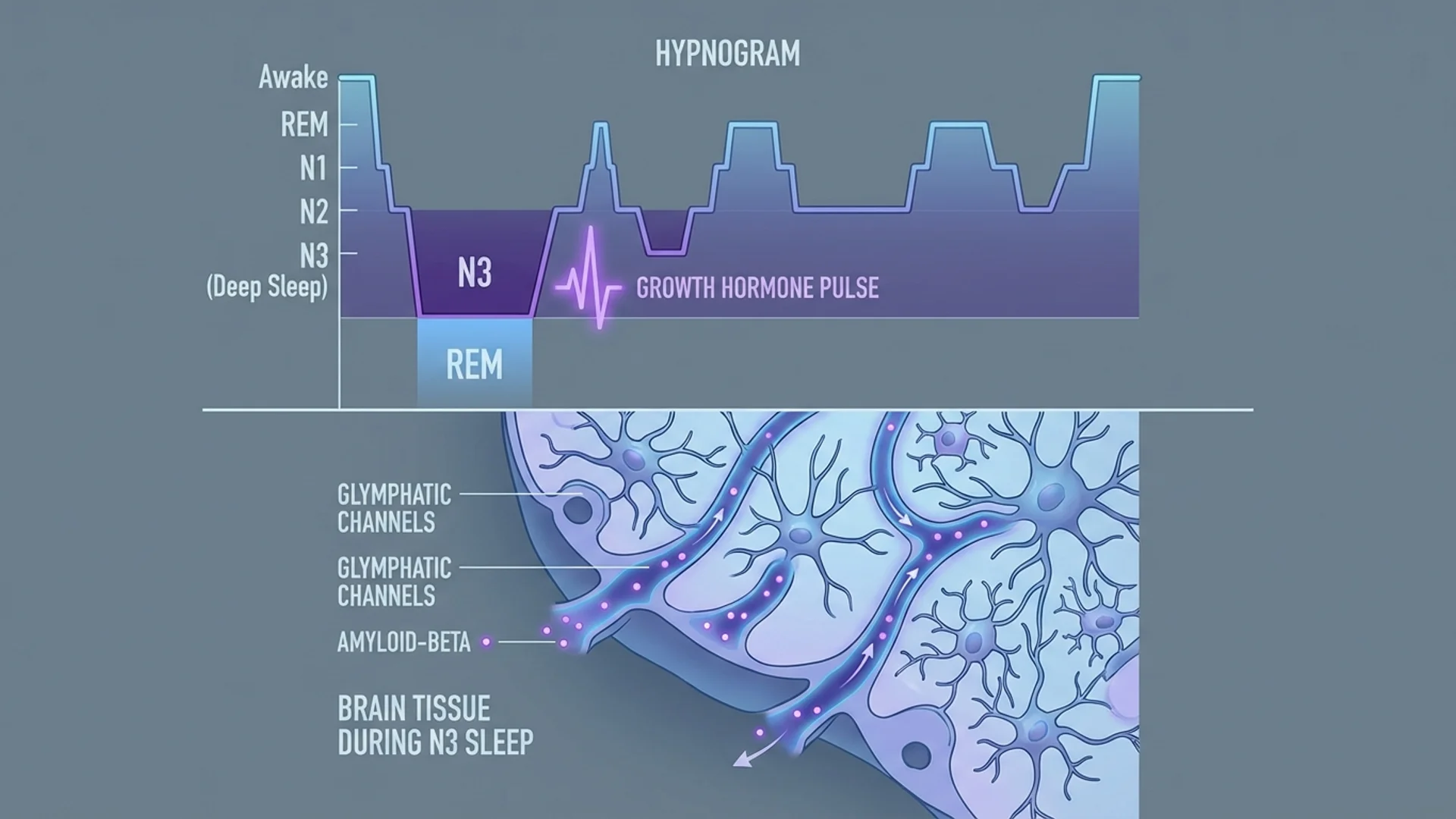
Poor sleep is both a symptom and a perpetuating factor in ME/CFS. We address sleep architecture through a combination of sleep hygiene optimization, targeted supplementation (magnesium glycinate, phosphatidylserine, low-dose melatonin where appropriate), and neurofeedback training to improve brainwave regulation.
I cannot discuss ME/CFS without addressing its overlap with Post-COVID syndrome and chronic Lyme disease. The mechanisms are strikingly similar: persistent immune activation, mitochondrial dysfunction, autonomic dysregulation, microclot formation, and impaired microcirculation.
At St. George Hospital, we see many patients whose chronic fatigue began after a COVID-19 infection, a tick bite, or another acute infectious trigger. The diagnostic and treatment frameworks overlap substantially, and our research colleagues — including Dr. Beate Jaeger, whose work on microclots and endothelial dysfunction has been an important research direction in understanding these conditions — are helping to illuminate the shared pathophysiology.
This convergence is actually encouraging. It means that advances in understanding Post-COVID fatigue inform our treatment of ME/CFS, and vice versa. The biological mechanisms are real, measurable, and increasingly treatable.
I believe in honesty with my patients. Here is what I can tell you:
We can identify and quantify the biological dysfunctions underlying your fatigue. We can implement targeted treatments that address those specific dysfunctions. The majority of our ME/CFS patients experience meaningful improvement in energy, cognitive function, and quality of life.
What I cannot promise is a complete cure for every patient. ME/CFS exists on a spectrum of severity, and outcomes depend on the duration of illness, the number and severity of contributing factors, and individual biological variability. Some patients achieve full recovery. Others achieve substantial improvement but need ongoing maintenance. A small number improve only modestly despite our best efforts.
What I can promise is that we will take your condition seriously, investigate it thoroughly, and treat it based on evidence rather than dismissal. If you have been told there is nothing wrong with you, and you know in your body that something is profoundly wrong, I encourage you to seek evaluation. The biology is real, and targeted treatment can make a meaningful difference.
If you would like to discuss whether our approach may be appropriate for your situation, our international patient team can arrange a preliminary consultation. You can reach us at info@clinicum-stgeorg.de or +49 (0)8061 398-0.