At a Glance
| Property | Rapamycin | Metformin |
|---|---|---|
| Primary Target | mTOR (mTORC1 inhibition) | AMPK activation, Complex I inhibition |
| Key Mechanism | Autophagy, cellular repair | Metabolic efficiency, insulin sensitivity |
| Animal Lifespan Data | Extends maximum lifespan in normal mammals (strongest data) | Extends median lifespan in some models; inconsistent for maximum lifespan |
| Human Safety Data | Limited (transplant/oncology patients at higher doses) | Extensive (60+ years in diabetes) |
| Longevity Dosing | 3-6mg once weekly (intermittent) | 500-1500mg daily |
| Evidence Level | Moderate (strong animal, limited human longevity) | Moderate (strong human safety, mixed longevity signal) |
| Can Combine? | Potentially yes (different mechanisms) | Potentially yes |
Two Drugs, Two Pathways, One Question
This is the comparison every longevity-interested person eventually arrives at: rapamycin or metformin? Which one has better evidence? Can you take both? Should you take either?
Let me be direct. Neither drug has been proven to extend human lifespan in a randomized controlled trial. That trial does not exist. What we have is a body of mechanistic research, animal data, and human observational data that supports different conclusions about each drug. The honest answer is more nuanced than most longevity influencers will tell you.
Here is what the evidence actually shows.
Rapamycin: The mTOR Inhibitor
The Mechanism
Rapamycin’s longevity potential centers on its inhibition of mTORC1 — one of two complexes of the mTOR (mechanistic Target Of Rapamycin) kinase. mTORC1 is the body’s master nutrient-sensing switch. When activated (by amino acids, insulin, growth factors), it promotes:
- Cell growth and proliferation
- Protein synthesis
- Lipid synthesis
- Suppression of autophagy
When mTORC1 is inhibited by rapamycin, the cell shifts toward:
- Autophagy — the cellular recycling process that clears damaged proteins, dysfunctional mitochondria, and other cellular debris
- Stress resistance — upregulation of protective heat shock proteins and antioxidant defenses
- Reduced inflammation — suppression of the SASP (senescence-associated secretory phenotype) from senescent cells
- Mitochondrial optimization — improved mitochondrial quality through mitophagy
The longevity hypothesis is straightforward: aging is driven in part by the accumulation of cellular damage. mTORC1 inhibition shifts cells from “growth mode” to “repair mode,” slowing this accumulation [1].
The Animal Evidence
This is where rapamycin stands alone.
The National Institute on Aging’s Interventions Testing Program (ITP) — the most rigorous drug-testing program in aging research, using genetically heterogeneous mice across three independent sites — has repeatedly demonstrated that rapamycin extends lifespan [2]:
- Extends maximum lifespan: Not just median (average) lifespan, but the maximum — meaning the longest-lived animals live even longer. This is the gold standard in aging research because it suggests a fundamental slowing of aging processes rather than just preventing a specific disease.
- Works when started late in life: Even when begun at 20 months (equivalent to roughly 60 human years), rapamycin extends lifespan. This is remarkable because most interventions only work when started early.
- Reproducible across sites: The ITP results have been confirmed at three independent laboratories — this is not a single-lab finding.
- Dose-response relationship: Higher doses produce greater lifespan extension, up to a point.
No other drug has achieved this in normal, genetically diverse mammals. Metformin has not. Resveratrol has not. NAD+ precursors have not. This is why rapamycin occupies a unique position in longevity pharmacology.
The Human Evidence
Here is where the picture becomes less clear.
Rapamycin (as sirolimus or everolimus) has been used in humans for decades — but primarily in organ transplant recipients and cancer patients, at doses much higher than those proposed for longevity, and in chronically immunosuppressed patients. This makes it difficult to extrapolate safety and efficacy to healthy aging adults.
The most relevant human data for longevity comes from:
- The PEARL study (Mannick et al., 2014): Low-dose everolimus (a rapamycin analog) improved immune function in elderly volunteers, as measured by response to influenza vaccination [3]. This was counterintuitive — an “immunosuppressant” that improved immune function — and it suggested that low-dose mTOR inhibition might rejuvenate rather than suppress the aging immune system.
- Follow-up studies confirmed improved immune response to viral antigens in elderly subjects treated with mTOR inhibitors at low doses.
- Off-label use data: A growing community of physicians prescribing low-dose intermittent rapamycin (3-6mg weekly) for longevity purposes. Published case series report generally favorable safety profiles, but this is uncontrolled observational data [4].
What we do not have: a randomized controlled trial measuring whether rapamycin extends human lifespan or healthspan. The VALIDATE trial and other studies are in progress, but results are years away.

Metformin: The AMPK Activator
The Mechanism
Metformin’s primary mechanism is activation of AMPK (AMP-activated protein kinase) — the cell’s energy-sensing enzyme. When cellular energy is low (high AMP-to-ATP ratio), AMPK activates and promotes:
- Glucose uptake and utilization — improving insulin sensitivity
- Fatty acid oxidation — shifting from fat storage to fat burning
- Mitochondrial biogenesis — production of new mitochondria
- Inhibition of mTORC1 — yes, metformin partially inhibits mTOR as a downstream effect of AMPK activation, creating some mechanistic overlap with rapamycin
- Reduced hepatic glucose production — the primary therapeutic effect in diabetes
- Anti-inflammatory effects — reduction of NF-kB signaling and pro-inflammatory cytokines [5]
Metformin also inhibits Complex I of the mitochondrial electron transport chain, which is the proximate trigger for AMPK activation and may independently contribute to its effects.
The Animal Evidence
Metformin’s longevity data in animals is genuinely mixed:
Positive findings:
- Extended lifespan in C. elegans (nematode worm) by approximately 40% [6]
- Extended lifespan in some mouse strains, particularly when combined with rapamycin
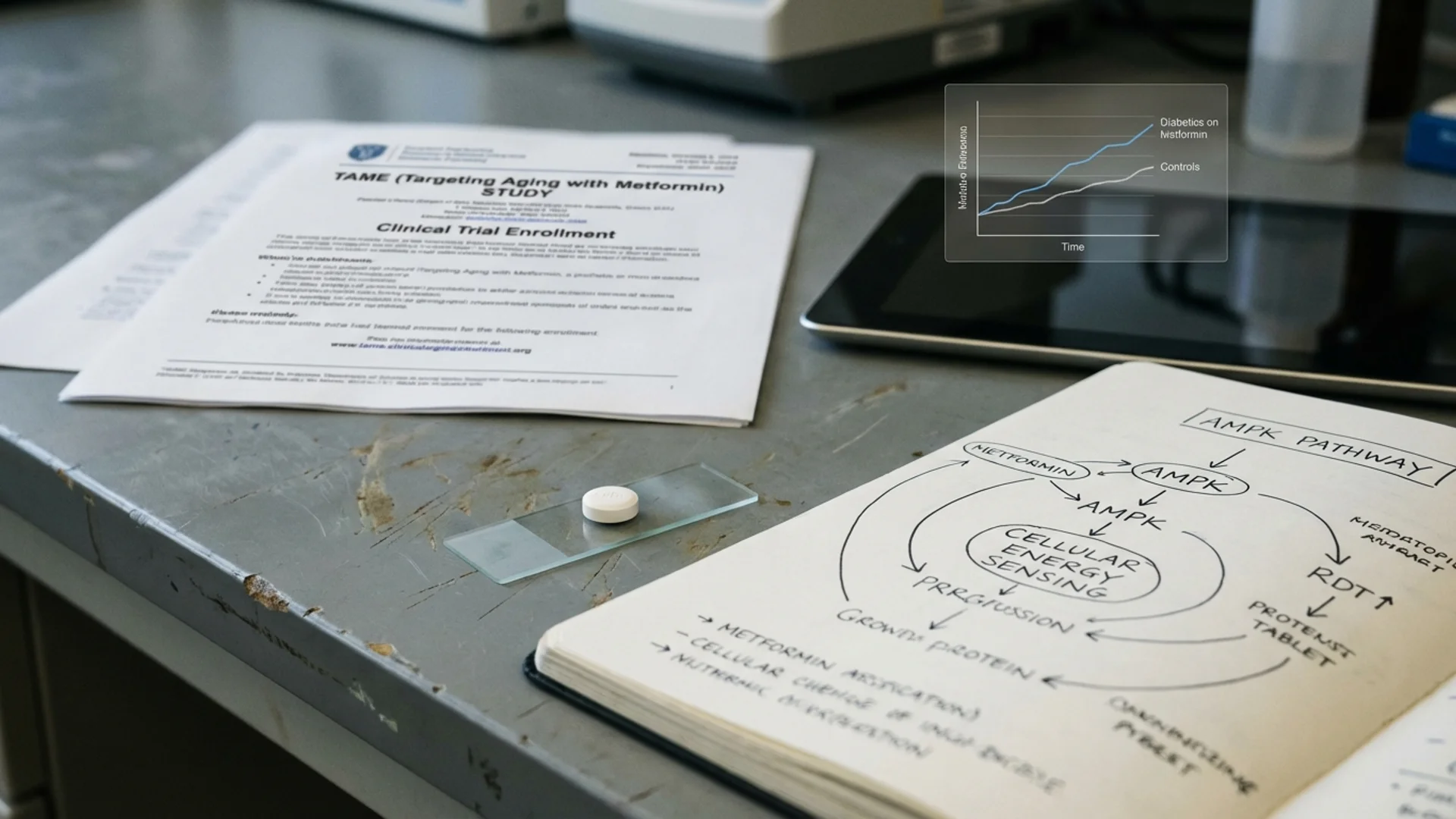
- The Bannister et al. (2014) observational study found that diabetics on metformin lived longer than non-diabetic controls — a striking finding, though confounded by selection bias [7]
Negative or null findings:
- The NIA Interventions Testing Program found that metformin did NOT significantly extend lifespan in genetically heterogeneous mice at the doses tested [8]
- In some mouse strains, metformin had no lifespan effect or even slightly negative effects
- Metformin does not consistently extend maximum lifespan — only median lifespan in some models
This is the critical distinction. The animal data for metformin is nowhere near as strong as for rapamycin. The ITP — the most rigorous testing platform available — found a significant effect for rapamycin but not for metformin.
The Human Evidence
Here, metformin has a massive advantage: sixty-plus years of human use in millions of diabetic patients.
What we know from diabetes data:
- Metformin is remarkably safe in long-term use. Side effects are primarily gastrointestinal (nausea, diarrhea) and generally manageable.
- Metformin reduces cardiovascular events and cancer incidence in diabetic patients [9].
- The Bannister observational data showing longer survival in metformin-treated diabetics vs. non-diabetic controls generated enormous interest, though this study has significant confounders.
- Metformin use is associated with reduced all-cause mortality in multiple observational cohorts.
The TAME trial: The Targeting Aging with Metformin (TAME) trial is the first FDA-sanctioned clinical trial explicitly targeting aging rather than a specific disease. Led by Nir Barzilai at Albert Einstein College of Medicine, TAME will test whether metformin delays the onset of age-related diseases in non-diabetic elderly adults [10]. This trial is historically significant because it represents regulatory recognition that aging itself can be a treatment target. However, it has been slow to complete, and results are not yet available.
The exercise interaction concern: An important and underappreciated finding: metformin may blunt the beneficial adaptations to exercise. A 2019 study showed that older adults taking metformin had attenuated improvements in VO2 max and mitochondrial respiration after an exercise training program compared to placebo [11]. If confirmed, this is a significant concern for healthy, active individuals who exercise regularly — metformin might negate some of the very benefits they are seeking.
Head-to-Head Comparison
Evidence Quality for Lifespan Extension
Rapamycin wins clearly. No other drug matches its ITP data — extension of both median and maximum lifespan in normal mammals, reproducible across multiple sites, effective even when started late in life. Metformin failed to achieve this in the same testing program.
However, rapamycin has far less human data in healthy aging populations. The human evidence for rapamycin longevity is early-stage; the human evidence for metformin safety is extensive.
Safety Profile for Healthy Adults
Metformin wins clearly. Sixty years of human use in millions of patients provides a safety dataset that no rapamycin longevity study can match. Metformin’s side effects are well-characterized and generally benign.
Rapamycin’s safety in low-dose intermittent use for healthy longevity is still being established. Potential concerns include:
- Impaired wound healing (observed at higher doses in transplant patients)
- Mouth ulcers (the most common complaint at longevity doses)
- Lipid profile changes (transient increases in LDL and triglycerides)
- Theoretical long-term immunosuppressive effects (though low-dose data suggests immune enhancement rather than suppression)
Mechanism Depth
Rapamycin is more direct. It targets mTORC1, the master switch of the growth-repair axis, with high specificity. The downstream effects on autophagy, senescent cell clearance, and inflammation are well-characterized.
Metformin’s mechanism is more diffuse. It activates AMPK, which has pleiotropic effects. It inhibits Complex I. It reduces inflammation through multiple pathways. This breadth may be a strength (multiple targets) or a weakness (less potent at any single target).
Dosing for Longevity
Rapamycin longevity dosing:
- Typical protocol: 3-6mg once weekly (some use every 5 days)
- The intermittent schedule is key — it allows mTORC1 inhibition (beneficial) while minimizing chronic mTORC2 inhibition (which causes insulin resistance and immunosuppression at higher continuous doses)
- No established “optimal” longevity dose — this is based on extrapolation from animal data and clinical observation
- Requires physician supervision and periodic blood monitoring (lipids, glucose, CBC)
Metformin longevity dosing:
- Typical protocol: 500mg once or twice daily (lower than diabetic doses of 1500-2000mg)
- Extended-release formulation preferred (fewer GI side effects)
- Some longevity physicians recommend 500mg daily as a starting and maintenance dose
- Well-tolerated by most people; GI side effects usually resolve with dose titration

Can You Combine Them?
This is the question I hear most frequently. The answer: potentially yes, and there is mechanistic rationale for doing so.
Rapamycin and metformin target different primary pathways (mTOR and AMPK, respectively), though there is downstream overlap. In animal studies, the combination has shown additive or synergistic lifespan effects in some models [12]. The theoretical advantage is dual-pathway modulation: rapamycin drives autophagy and cellular repair from the mTOR side, while metformin improves metabolic efficiency and insulin sensitivity from the AMPK side.
The practical consideration: If you are already taking rapamycin, which partially inhibits mTORC1 and can transiently raise glucose, adding metformin provides metabolic counterbalance by improving insulin sensitivity and reducing hepatic glucose output.
The caution: There is no published clinical trial of the rapamycin-metformin combination specifically for longevity in healthy humans. This is theoretical and based on animal data plus clinical reasoning. In my clinical experience, the combination is tolerated by most patients, but it requires monitoring.
Who Should Use Which
Here is how I think about this in clinical practice.
Consider rapamycin if:
- You are highly motivated by the strength of the animal lifespan data
- You are comfortable with a drug that has less human safety data in healthy populations
- You are willing to be monitored regularly (blood panels every 3-6 months)
- You do not have uncontrolled metabolic syndrome or diabetes (rapamycin can worsen insulin resistance)
- You understand that this is investigational use based on moderate evidence
Consider metformin if:
- You prioritize safety and want a drug with decades of human data
- You have metabolic syndrome, insulin resistance, or are pre-diabetic (where metformin has the strongest benefit)
- You want a low-risk, low-monitoring-burden intervention
- You are not a competitive athlete or someone whose exercise adaptations you want to maximize (given the exercise blunting concern)
- You want a starting point before potentially adding rapamycin
Consider both if:
- You want dual-pathway coverage
- You tolerate both individually
- You have a physician who can monitor you appropriately
- You accept that the combination is based on animal data and clinical reasoning, not human longevity trials
Consider neither if:
- Your lifestyle fundamentals (sleep, exercise, nutrition, stress management) are not optimized — fix those first; they have better evidence than either drug
- You are looking for a guarantee — neither drug has been proven to extend human lifespan
- You have medical contraindications to either drug
What I Tell My Patients
Here is my honest assessment.
Rapamycin has the best mechanistic and animal evidence of any longevity drug we know. If I had to bet on one drug to extend human lifespan, it would be rapamycin. But we do not have the human data yet, and the risk profile in healthy populations is still being defined.
Metformin is the safer bet — extensively tested in humans, well-tolerated, with plausible but weaker longevity evidence. It is the more conservative choice, and there is nothing wrong with conservative in an area where the research is still emerging.
The exercise interaction with metformin gives me pause for active, fit individuals. If your primary longevity strategy is vigorous exercise (which has excellent evidence for healthspan), adding a drug that may blunt exercise adaptations requires careful thought.
The nuance matters. This is not a binary choice between a “winner” and a “loser.” It is a decision that depends on your individual risk profile, metabolic status, lifestyle, and comfort with investigational use. Any physician who tells you the answer is obvious is not being honest with you.
The Bottom Line
Rapamycin inhibits mTOR to promote autophagy and cellular repair. Metformin activates AMPK to improve metabolic efficiency. Rapamycin has stronger animal lifespan data; metformin has far more human safety data. They can potentially be combined. Neither has been proven to extend human lifespan. The right choice depends on your individual profile, and both require physician supervision and honest expectations about what the current evidence does and does not support.
Every conventional medicine was once alternative medicine. These drugs may one day be standard longevity interventions. Today, they are promising, evidence-informed, and investigational. That is the honest picture.
References
- Johnson SC, Rabinovitch PS, Kaeberlein M. mTOR is a key modulator of ageing and age-related disease. Nature. 2013;493(7432):338-345.
- Harrison DE, Strong R, Sharp ZD, et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature. 2009;460(7253):392-395.
- Mannick JB, Del Giudice G, Lattanzi M, et al. mTOR inhibition improves immune function in the elderly. Sci Transl Med. 2014;6(268):268ra179.
- Blagosklonny MV. Rapamycin for longevity: opinion article. Aging. 2019;11(19):8048-8067.
- Foretz M, Guigas B, Viollet B. Understanding the glucoregulatory mechanisms of metformin in type 2 diabetes mellitus. Nat Rev Endocrinol. 2019;15(10):569-589.
- Onken B, Driscoll M. Metformin induces a dietary restriction-like state and the oxidative stress response to extend C. elegans healthspan via AMPK, LKB1, and SKN-1. PLoS ONE. 2010;5(1):e8758.
- Bannister CA, Holden SE, Jenkins-Jones S, et al. Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non-diabetic controls. Diabetes Obes Metab. 2014;16(11):1165-1173.
- Strong R, Miller RA, Antebi A, et al. Longer lifespan in male mice treated with a weakly estrogenic agonist, an antioxidant, an alpha-glucosidase inhibitor or a Nrf2-inducer. Aging Cell. 2016;15(5):872-884.
- UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352(9131):854-865.
- Barzilai N, Crandall JP, Kritchevsky SB, et al. Metformin as a tool to target aging. Cell Metab. 2016;23(6):1060-1065.
- Konopka AR, Laurin JL, Schoenberg HM, et al. Metformin inhibits mitochondrial adaptations to aerobic exercise training in older adults. Aging Cell. 2019;18(1):e12880.
- Fang J, Yang J, Wu X, et al. Metformin alleviates human cellular aging by upregulating the endoplasmic reticulum glutathione peroxidase 7. Aging Cell. 2018;17(4):e12765.