At a Glance
| Property | Value |
|---|---|
| Evidence Level | Metformin: Strong. Berberine: Moderate (smaller trials, shorter follow-up) |
| Primary Mechanism | Both: AMPK activation, improved insulin sensitivity |
| Key Difference | Evidence depth (1,600+ vs ~34 trials), drug interaction profile, exercise compatibility |
Metformin vs. Berberine: An Honest Comparison
This is one of the most searched comparison queries in the longevity space right now, and for good reason. Both metformin for longevity and berberine activate AMPK — the master metabolic sensor that sits at the intersection of caloric restriction, exercise, and aging pathways. Both lower blood glucose. Both have been proposed as geroprotective agents.
But treating them as interchangeable is a mistake that ignores the massive asymmetry in evidence quality between these two compounds. Let me be direct about what we know, what we do not know, and how to make a rational choice.
The AMPK Connection
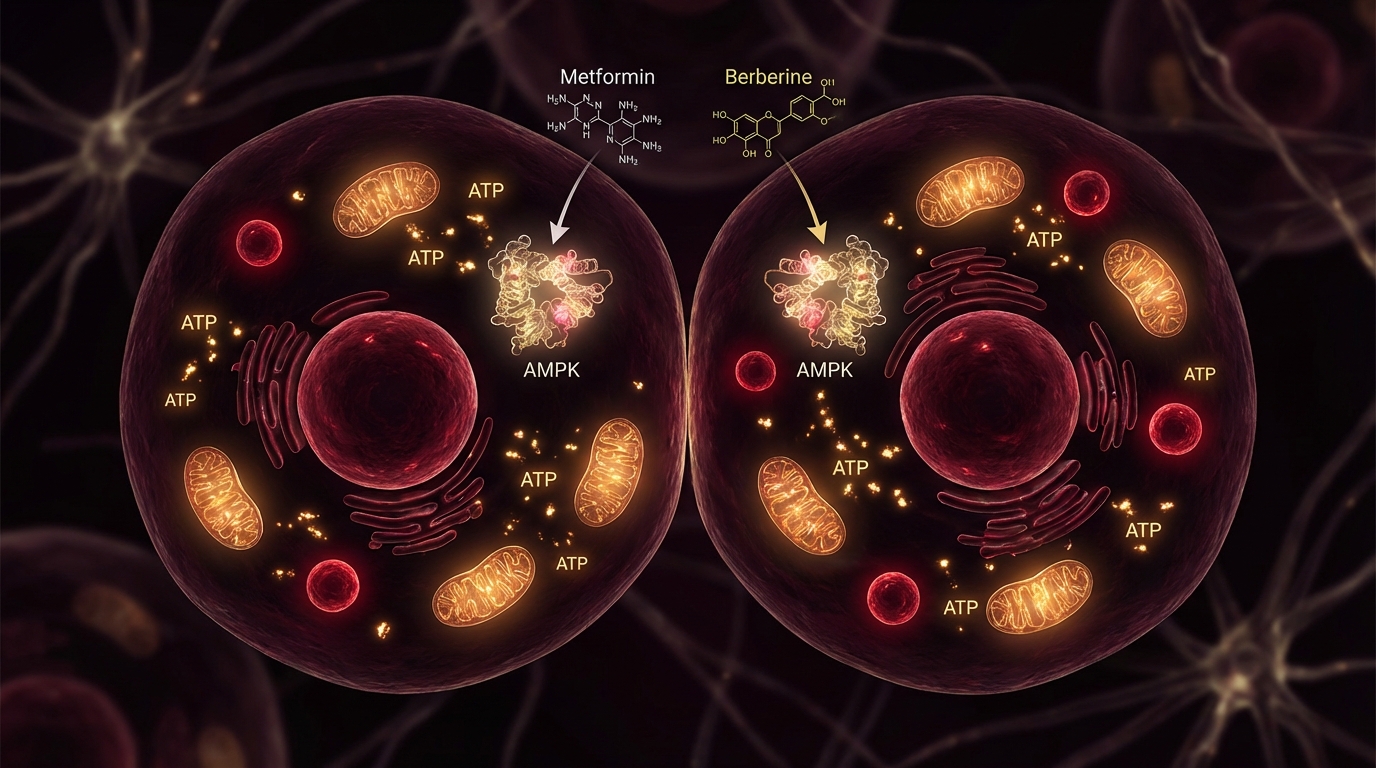
Both metformin and berberine activate AMPK, but they do so through different upstream mechanisms:
Metformin inhibits mitochondrial complex I in the electron transport chain. This reduces ATP production, increasing the AMP:ATP ratio, which activates AMPK. The effect is relatively specific and well-characterized after six decades of pharmacological study.
Berberine also inhibits mitochondrial complex I, but additionally activates AMPK through direct interaction with the AMPK gamma subunit and through effects on gut microbiome composition. Berberine also inhibits protein-tyrosine phosphatase 1B (PTP1B), enhancing insulin receptor signaling through a mechanism independent of AMPK (1).
The downstream effects of AMPK activation include:
- Improved insulin sensitivity and glucose uptake
- Inhibition of mTOR pathway and longevity (reducing cellular proliferation, promoting autophagy)
- Enhanced mitochondrial biogenesis
- Activation of SIRT1 and FOXO transcription factors
- Improved lipid metabolism
Both compounds trigger these pathways. The question is not mechanism — it is magnitude, reliability, and safety.
The Evidence Gap
This is where the comparison becomes uncomfortable for berberine advocates. Let me state the numbers plainly.
Metformin
- Clinical trials: 1,600+ registered on ClinicalTrials.gov
- Years of human use: 60+ (approved in France 1957, US 1995)
- Patient exposure: Hundreds of millions of patients globally
- Safety database: Massive. Every rare side effect has been characterized.
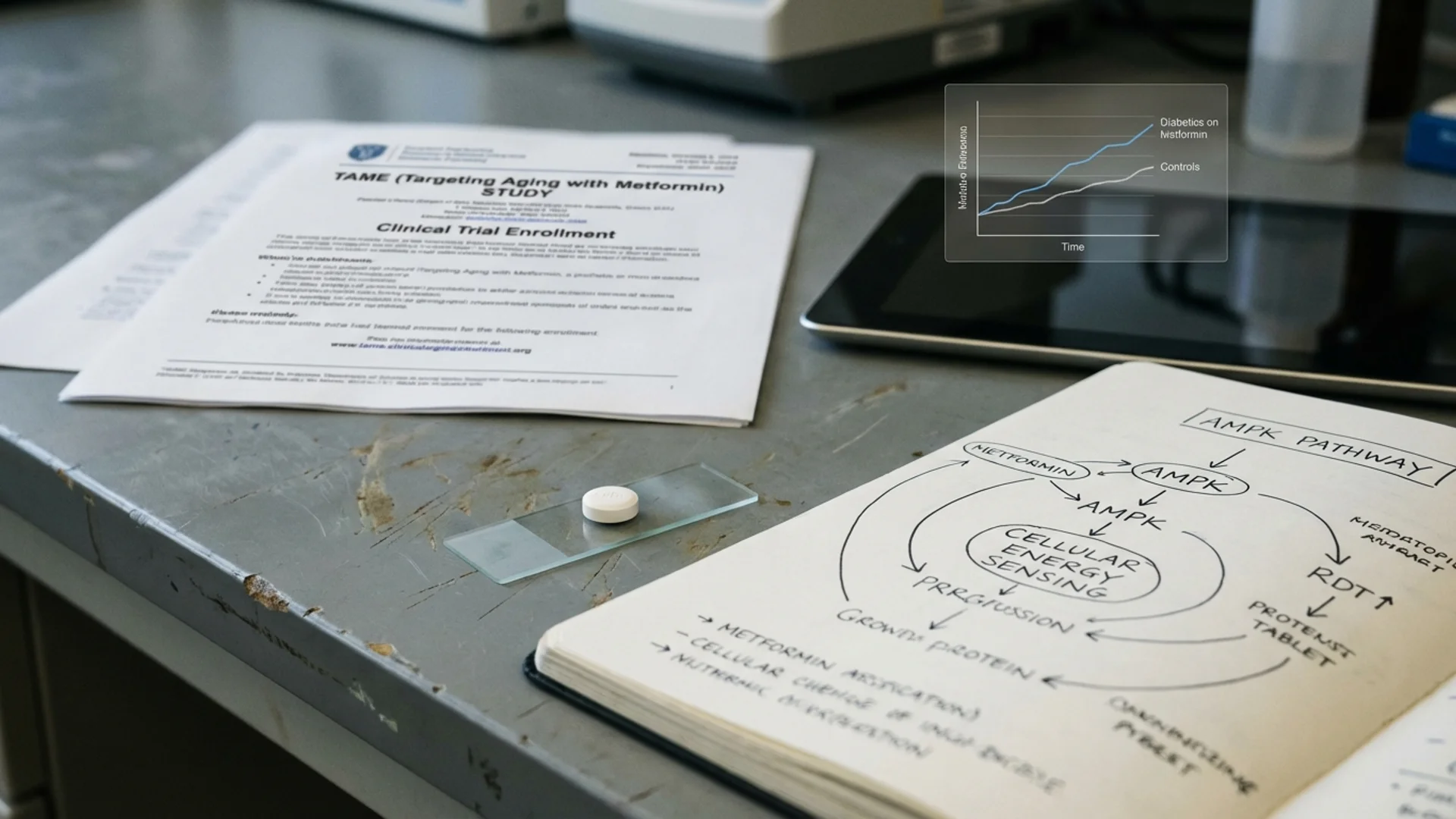
- Longevity-specific evidence: The TAME trial (3,000 participants, 6-year follow-up, FDA-approved) is the first-ever aging trial for any drug
- Observational longevity data: Bannister et al. showed diabetics on metformin outliving non-diabetic controls (2)
Berberine
- Clinical trials: Approximately 34 RCTs, mostly in Chinese populations
- Years of human use: Traditional medicine use for centuries; modern clinical study for ~20 years
- Patient exposure in trials: Typically 50-200 participants per trial
- Safety database: Limited. Long-term safety in healthy Western populations is not established.
- Longevity-specific evidence: None. No aging trials. No long-term mortality data.
- Best glucose data: Yin et al. (2008) showed 500 mg berberine 3x/day reduced HbA1c comparably to metformin 500 mg 3x/day over 3 months in type 2 diabetics (3)
The Yin study is frequently cited as evidence that “berberine is as good as metformin.” Let me be precise about what it actually showed: in a small (n=36 per group), short-term (3 months) trial in newly diagnosed Chinese type 2 diabetics, berberine produced comparable glucose reduction to metformin. That is a useful data point. It is not equivalence across the full spectrum of metformin’s demonstrated effects.
Head-to-Head Comparison
| Parameter | Metformin | Berberine |
|---|---|---|
| AMPK activation | Yes (via complex I inhibition) | Yes (via complex I + direct AMPK binding) |
| Glucose reduction | Well-established (HbA1c reduction ~1-1.5%) | Comparable in small trials (~0.9-1.2%) |
| Lipid effects | Modest (slight LDL reduction) | Stronger (LDL reduction + triglyceride reduction) |
| Bioavailability | 50-60% oral | ~5% oral (extensive first-pass metabolism) |
| Half-life | 4-8 hours | 2-4 hours |
| Dosing | 500-1,500 mg/day (longevity) | 500 mg 2-3x/day (typical) |
| GI side effects | 15-30% (formulation dependent) | 10-25% (similar GI effects) |
| Drug interactions | Few significant | Extensive CYP2D6, CYP3A4 inhibition |
| Exercise blunting | Documented (Konopka 2019) | Not studied; theoretically less |
| B12 depletion | Yes (5-10% long-term) | No |
| Regulatory status | FDA-approved prescription drug | Dietary supplement (unregulated quality) |
| Cost | $4-15/month (generic) | $15-40/month (varies by brand) |
The Exercise Question: Berberine’s Potential Advantage
The most compelling argument for berberine over metformin in the longevity context is exercise compatibility. Metformin has been shown to blunt mitochondrial adaptation to aerobic exercise training. Berberine has not been studied in this context — which means we do not know either way — but there are theoretical reasons to think it may be less problematic:
- Berberine’s very poor oral bioavailability (5%) means systemic exposure is lower than metformin’s at equivalent doses. The muscle-level concentration may be insufficient to meaningfully inhibit complex I in exercising tissue.
- Berberine’s additional mechanisms (PTP1B inhibition, gut microbiome effects) may provide metabolic benefits without requiring the same degree of mitochondrial complex I inhibition.
- Berberine’s shorter half-life (2-4 hours vs 4-8 hours) means timing separation from exercise may be more effective.
This is theoretical. I want to be clear: there are zero published studies comparing berberine and metformin for exercise adaptation blunting. The argument is mechanistically plausible, not evidence-confirmed. In my clinical experience, patients who switch from metformin to berberine often report subjectively better exercise tolerance, but this is anecdotal and subject to placebo effects.
The Lipid Advantage
Berberine has a genuine edge in lipid modulation. Meta-analyses show berberine reduces LDL cholesterol by approximately 20-25 mg/dL and triglycerides by 35-45 mg/dL — effects that are clinically meaningful and comparable to low-dose statins. Metformin has modest lipid effects by comparison.
The mechanism involves berberine’s upregulation of hepatic LDL receptor expression via PCSK9 pathway inhibition — the same pathway targeted by the expensive PCSK9 inhibitor drugs. If cardiovascular risk reduction through lipid management is a primary goal, berberine has a pharmacological advantage in this specific domain.
The Drug Interaction Problem
Here is something that rarely gets discussed in the berberine-vs-metformin conversation: berberine is a potent inhibitor of CYP2D6 and CYP3A4, two of the most important drug-metabolizing enzymes in the liver.
This means berberine can significantly increase blood levels of:
- Statins (atorvastatin, simvastatin) — increasing myopathy risk
- Blood thinners (warfarin) — increasing bleeding risk
- Many antidepressants (SSRIs, tricyclics)
- Immunosuppressants (cyclosporine, tacrolimus)
- Some blood pressure medications
Metformin has almost no CYP-mediated drug interactions. For patients taking multiple medications, this difference is clinically significant.
Quality Control: The Supplement Problem
Berberine is sold as a dietary supplement, not a pharmaceutical. This means:
- No standardized manufacturing requirements
- No FDA pre-market approval for safety or efficacy
- Variable potency between brands and even between batches
- No guarantee that what is on the label is in the bottle
This is something that makes me genuinely angry about the supplement industry. Berberine is real pharmacology — it has real drug interactions and real biological effects — being sold without pharmaceutical quality controls. If you use berberine, buy from a manufacturer that provides third-party testing (USP, NSF, or ConsumerLab verification). This matters.
Who Should Choose What
Based on the evidence, here is my clinical framework:
Choose Metformin If:
- You want the most evidence-supported option
- You are over 50 with metabolic risk factors
- You take few other medications (minimal interaction concern)
- You exercise moderately (<4 hours/week structured training)
- You have access to a physician who will prescribe and monitor appropriately
Choose Berberine If:
- You exercise intensely (>4 hours/week) and are concerned about exercise blunting
- You cannot tolerate metformin despite extended-release and slow titration
- You want additional lipid-lowering effects
- You prefer a non-prescription option (with awareness of quality control limitations)
- You do not take medications with significant CYP2D6/3A4 metabolism
Consider Both (Alternating or Combined) If:
- This approach has no published evidence. I mention it because some longevity physicians use it, but I cannot recommend it without data.
Berberine Dosing Protocol
If you choose berberine:
- Standard dose: 500 mg, 2-3 times daily, with meals
- Start conservatively: 500 mg once daily for 1 week, then twice daily for 1 week, then three times daily
- Take with food: Reduces GI effects and improves the already-poor absorption
- Use quality brands: Look for third-party testing certifications
- Consider berberine phytosome formulations: Enhanced bioavailability products may achieve therapeutic levels at lower doses
The Bottom Line
Metformin has an evidence base for metabolic health and potential longevity that berberine cannot match — not because berberine does not work, but because it has not been studied with anything approaching the same rigor. Berberine is a legitimate pharmacological agent with real AMPK-activating, glucose-lowering, and lipid-improving effects, but it operates in a regulatory gray zone with quality control issues and significant drug interaction potential.
What I tell my patients: if I had to choose one for myself, I would choose metformin — because I trust the depth of the evidence. But I would not dismiss a patient who chose berberine for exercise compatibility reasons, provided they used a quality product and understood the limitations.
References
-
Zhang Y, Li X, Zou D, et al. Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. Journal of Clinical Endocrinology & Metabolism. 2008;93(7):2559-2565. doi:10.1210/jc.2007-2404
-
Bannister CA, Holden SE, Jenkins-Jones S, et al. Can people with type 2 diabetes live longer than those without? Diabetes, Obesity and Metabolism. 2014;16(11):1165-1173. doi:10.1111/dom.12354
-
Yin J, Xing H, Ye J. Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. 2008;57(5):712-717. doi:10.1016/j.metabol.2008.01.013
-
Lan J, Zhao Y, Dong F, et al. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. Journal of Ethnopharmacology. 2015;161:69-81. doi:10.1016/j.jep.2014.09.049