At a Glance
| Property | Value |
|---|---|
| Evidence Level | Strong (decades of safety data in diabetics; moderate for longevity-specific concerns) |
| Primary Concerns | GI disturbance, B12 depletion, exercise adaptation blunting, theoretical lean mass effects |
| Key Mitigation | Extended-release formulation, B12 supplementation, strategic timing around exercise |
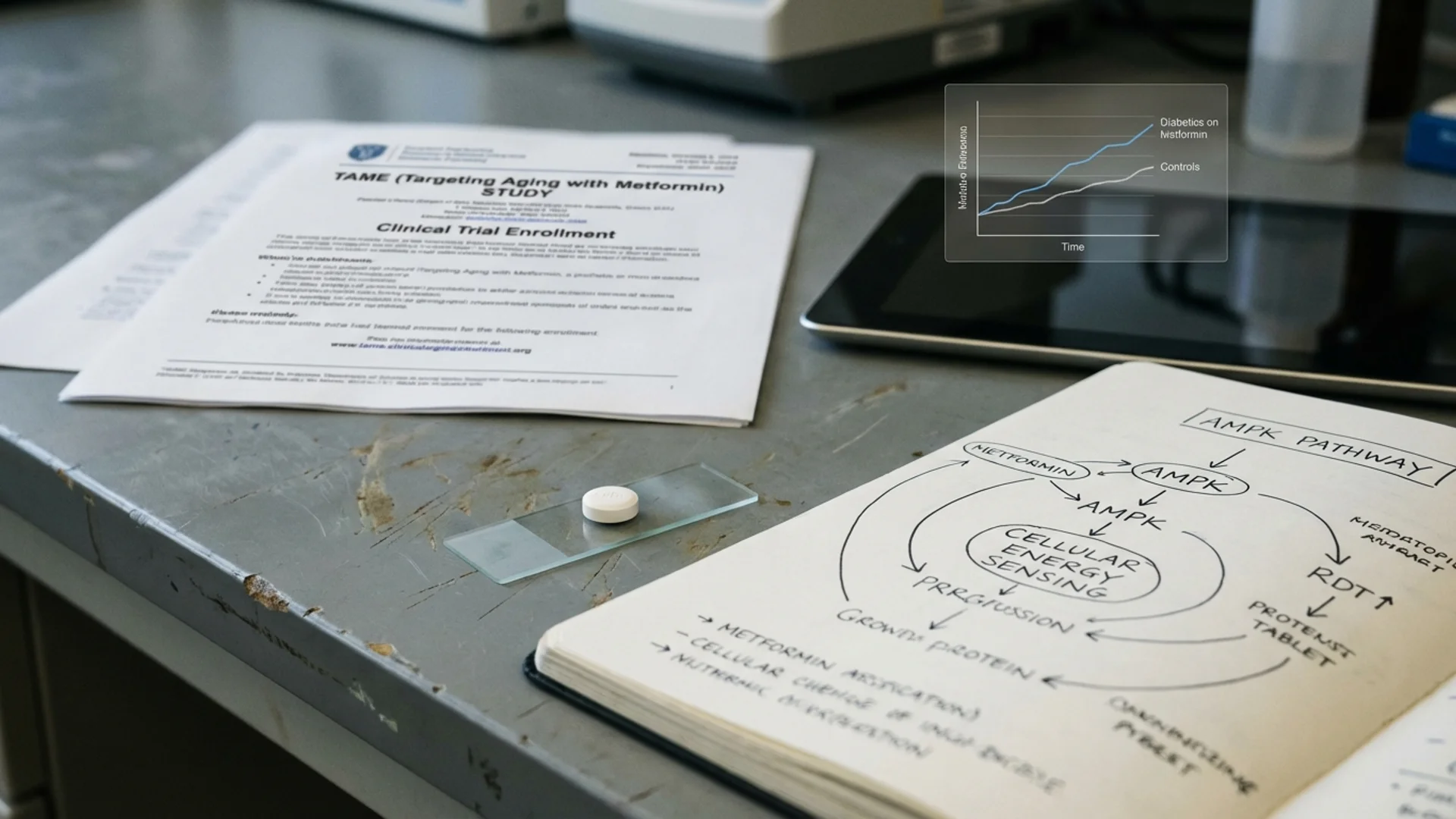
Metformin Side Effects: Why the Anti-Aging Context Is Different
Most of what you read about metformin side effects comes from diabetic populations — people who are typically older, heavier, and metabolically compromised. If you are a non-diabetic taking metformin at 1,000-1,500 mg/day for longevity, your risk profile is meaningfully different. You are healthier at baseline. Your doses are lower. And your goals are different — you are not managing blood sugar, you are attempting to modulate aging pathways.
That said, metformin is not a vitamin. It is a pharmaceutical that alters fundamental metabolic processes, and it has real side effects that deserve honest discussion. Here is what the evidence shows.
GI Disturbance: The Most Common Issue
What Happens
Gastrointestinal side effects are the most frequent reason people discontinue metformin. The mechanism involves metformin’s accumulation in the intestinal mucosa, where it alters gut microbiome composition, increases serotonin secretion in the gut, and affects bile acid metabolism. Symptoms include:
- Nausea (especially after meals)
- Diarrhea or loose stools
- Abdominal bloating and cramping
- Metallic taste
- Reduced appetite
How Common Is It?
With immediate-release (IR) metformin: 25-30% of users experience meaningful GI symptoms. With extended-release (ER/XR): approximately 10-15%. This difference alone makes the formulation choice critical for longevity users, where adherence over years matters more than cost savings.
How to Mitigate It
- Always use extended-release. This is non-negotiable for longevity use. The slower intestinal release dramatically reduces mucosal irritation.
- Take with food. Specifically with your largest meal, ideally dinner. This slows absorption further and provides a food buffer.
- Titrate slowly. Start at 500 mg and increase by 500 mg every 2 weeks. Rushing the titration is the most common mistake. See my full metformin dosing protocol for details.
- Wait it out. GI symptoms typically peak in weeks 1-3 and resolve by week 6. If symptoms persist beyond 8 weeks at the same dose, that dose may be your ceiling.
- Consider a probiotic. Metformin alters gut microbiome composition, reducing Bacteroidetes and increasing Firmicutes. A quality probiotic may help restore balance. See my guide on choosing the right probiotic strains.
B12 Depletion: The Silent Concern
Why This Matters More Than You Think
Metformin inhibits vitamin B12 absorption in the terminal ileum by interfering with the calcium-dependent ileal membrane receptor that mediates B12-intrinsic factor uptake. This is not a rare effect — it is a predictable pharmacological consequence that develops gradually over months to years.
The DPP (Diabetes Prevention Program) Outcomes Study found that after 5 years of metformin use, B12 deficiency (serum B12 < 203 pg/mL) was present in 4.3% of metformin users versus 2.3% of placebo users. Low B12 (203-298 pg/mL) was present in an additional 19.1% of metformin users (1).
Why This Is Especially Dangerous for Anti-Aging Users
The symptoms of B12 deficiency — fatigue, cognitive fog, peripheral neuropathy, mood changes, impaired balance — overlap almost perfectly with symptoms of aging. If you are taking metformin to slow aging and develop B12 deficiency, you may attribute the deficiency symptoms to aging itself, creating a vicious cycle where the treatment appears to cause the very thing you are trying to prevent.
Peripheral neuropathy from B12 deficiency can become irreversible if not caught early. In my clinical experience, this is the single most important monitoring parameter for longevity metformin users.
Prevention and Monitoring
- Supplement prophylactically. Methylcobalamin 1,000 mcg/day sublingually. This bypasses the impaired intestinal absorption pathway.
- Test annually. Serum B12 plus methylmalonic acid (MMA). MMA is a more sensitive marker of functional B12 status — it rises before serum B12 drops to overtly deficient levels.
- Target levels. Keep serum B12 above 400 pg/mL for optimal neurological function, not just above the lower reference limit of 200 pg/mL.
Exercise Adaptation Blunting: The Inconvenient Finding
The Konopka Study
In 2019, Konopka et al. published a study that sent ripples through the longevity community. Older adults (aged 62-70) were randomized to metformin 2,000 mg/day or placebo during a 12-week aerobic exercise training program. The metformin group showed significantly blunted improvements in whole-body insulin sensitivity, VO2 max, and skeletal muscle mitochondrial respiration compared to placebo (2).
This is not a trivial finding. Exercise is the most robustly demonstrated longevity intervention. If metformin partially counteracts exercise benefits, the net effect on lifespan could be negative for physically active individuals — even though metformin alone shows longevity signals.
The Nuance
Several important caveats:
- The dose was 2,000 mg/day — higher than most longevity protocols (1,000-1,500 mg). Dose-dependent effects are plausible but unconfirmed.
- The study was 12 weeks. Long-term adaptation patterns may differ.
- The mechanism is understood. Metformin inhibits mitochondrial complex I, which is the same complex that exercise training upregulates. The conflict is mechanistically logical.
- Not all outcomes were blunted. Some metabolic markers still improved in the metformin group, just to a lesser degree.
My Clinical Approach
For patients who exercise seriously (>4 hours/week structured training):
- Option A: Skip metformin on training days. Take it only on rest days (3-4 days/week). This preserves exercise adaptation while maintaining some AMPK activation.
- Option B: Use metformin only in the evening, separated from morning/afternoon training by 8+ hours.
- Option C: Consider berberine as an alternative AMPK activator — it may have less exercise interference, though the evidence is preliminary.
- Option D: Forgo metformin entirely if you are already achieving excellent metabolic health through exercise, sleep, and nutrition. The marginal benefit of adding metformin to an already-optimized lifestyle may not justify the exercise blunting risk.
Lean Mass and Body Composition
The Concern
Metformin suppresses mTOR signaling, which is part of its anti-aging mechanism — reduced mTOR activity is associated with longevity in virtually every model organism studied. However, mTOR is also essential for muscle protein synthesis. The concern: could chronic mTOR suppression via metformin accelerate age-related sarcopenia?
What the Data Shows
The evidence here is mixed and mostly indirect:
- Metformin users in diabetic cohorts do not show clinically significant lean mass loss in most studies.
- However, diabetic populations are not the best proxy for fit longevity seekers who are also exercising.
- The combination of exercise blunting (reduced mitochondrial adaptation) plus mTOR suppression (reduced protein synthesis signaling) creates a theoretical double hit on muscle that has not been adequately studied in healthy, exercising adults.
Practical Recommendation
If you are taking metformin for longevity and resistance training for muscle preservation:
- Ensure protein intake of 1.6-2.2 g/kg/day.
- Prioritize leucine-rich protein sources post-training.
- Monitor body composition with DEXA annually.
- Consider separating metformin dosing from post-training protein intake by at least 2-3 hours.
Lactic Acidosis: Rare but Worth Understanding
Lactic acidosis is the most feared metformin side effect, and it deserves context. The incidence is approximately 3-10 cases per 100,000 patient-years — extremely rare. It almost exclusively occurs in the setting of:
- Renal impairment (eGFR < 30 mL/min)
- Acute illness causing dehydration or hypoxia
- Excessive alcohol use
- Hepatic impairment
For a healthy non-diabetic with normal kidney function taking 1,000-1,500 mg/day, the risk of lactic acidosis is vanishingly small. Nevertheless, monitor creatinine and eGFR every 6 months, and hold metformin during any acute illness, surgery, or radiologic contrast dye procedures.
Other Side Effects Worth Noting
Taste Changes
A metallic taste is reported by roughly 3% of users. It is benign but annoying. It typically resolves with continued use or dose reduction.
Reduced Testosterone (Theoretical)
Some studies in diabetic men have shown modest testosterone reductions with metformin. The clinical significance in non-diabetic men at longevity doses is unclear. If you are monitoring hormones, track total and free testosterone at baseline and 6 months.
Gut Microbiome Changes
Metformin significantly alters gut microbiome composition — increasing Akkermansia muciniphila (generally considered beneficial) while reducing overall microbial diversity. Some researchers have proposed that metformin’s metabolic benefits are partly mediated through these microbiome changes. The long-term implications of chronic microbiome alteration in healthy individuals are not fully understood.
Safety and Monitoring Summary
| Parameter | Frequency | Target | Action if Abnormal |
|---|---|---|---|
| Serum B12 + MMA | Every 12 months | B12 > 400 pg/mL | Increase methylcobalamin supplementation |
| Creatinine / eGFR | Every 6 months | eGFR > 45 mL/min | Dose reduce if 30-45; discontinue if < 30 |
| Fasting glucose / HbA1c | Every 6 months | Glucose > 70 mg/dL | Reduce dose if hypoglycemic |
| Lactate | Baseline + annually | < 2.0 mmol/L | Evaluate renal and hepatic function |
| Body composition (DEXA) | Annually | Stable lean mass | Reassess dose and exercise protocol |
| VO2 max (optional) | Baseline + 6 months | No decline | Consider exercise-day skipping protocol |
The Bottom Line
Metformin is remarkably safe for a drug that has been used by hundreds of millions of people. But “safe” does not mean “side-effect free,” and the side effect profile matters differently when healthy people take it indefinitely for longevity. B12 depletion, exercise adaptation blunting, and GI disturbance are real concerns that require proactive management. What I tell my patients: if you choose metformin for longevity, you are also choosing to monitor it properly. The drug without the monitoring is not a complete protocol.
References
-
Aroda VR, Edelstein SL, Goldberg RB, et al. Long-term metformin use and vitamin B12 deficiency in the Diabetes Prevention Program Outcomes Study. Journal of Clinical Endocrinology & Metabolism. 2016;101(4):1754-1761. doi:10.1210/jc.2015-3754
-
Konopka AR, Laurin JL, Schoenberg HM, et al. Metformin inhibits mitochondrial adaptations to aerobic exercise training in older adults. Aging Cell. 2019;18(1):e12880. doi:10.1111/acel.12880
-
DeFronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin-dependent diabetes mellitus. New England Journal of Medicine. 1995;333(9):541-549. doi:10.1056/NEJM199508313330902
-
Lalau JD. Lactic acidosis induced by metformin: incidence, management, and prevention. Drug Safety. 2010;33(9):727-740. doi:10.2165/11536790-000000000-00000