Ehrlichia and Anaplasma are obligate intracellular bacteria transmitted by ticks — the same ticks that carry Borrelia and Babesia. They share a fundamental strategy: they invade white blood cells, the very cells the immune system uses to fight infection. Ehrlichia monocytogenes targets monocytes. Anaplasma phagocytophilum targets neutrophils.
By parasitizing immune cells, these organisms simultaneously suppress the immune response and create a protected intracellular niche. This is one of the reasons that patients with Ehrlichia or Anaplasma co-infections often have more severe immune compromise and slower recovery from other tick-borne diseases.
Clinical Presentation
Both infections produce a similar acute syndrome:

- Flu-like illness — fever, chills, severe headache, myalgia, malaise
- Onset typically 5-14 days after tick exposure
- Leukopenia (low white blood cell count) — characteristic and clinically useful as a diagnostic clue
- Thrombocytopenia (low platelet count)
- Elevated liver transaminases (AST, ALT)
- Rash in some cases of ehrlichiosis (less common in anaplasmosis)
In the chronic setting — when these infections persist as co-infections alongside Lyme disease — the presentation may be subtler: persistent cytopenias, unexplained elevated liver enzymes, recurrent flu-like episodes, and disproportionate immune suppression.
Diagnostic Clues
Laboratory findings. The combination of leukopenia, thrombocytopenia, and elevated liver enzymes in a patient with tick exposure is highly suggestive. I always review the complete blood count carefully in tick-borne disease patients — these findings may be the first indication of Ehrlichia or Anaplasma involvement.
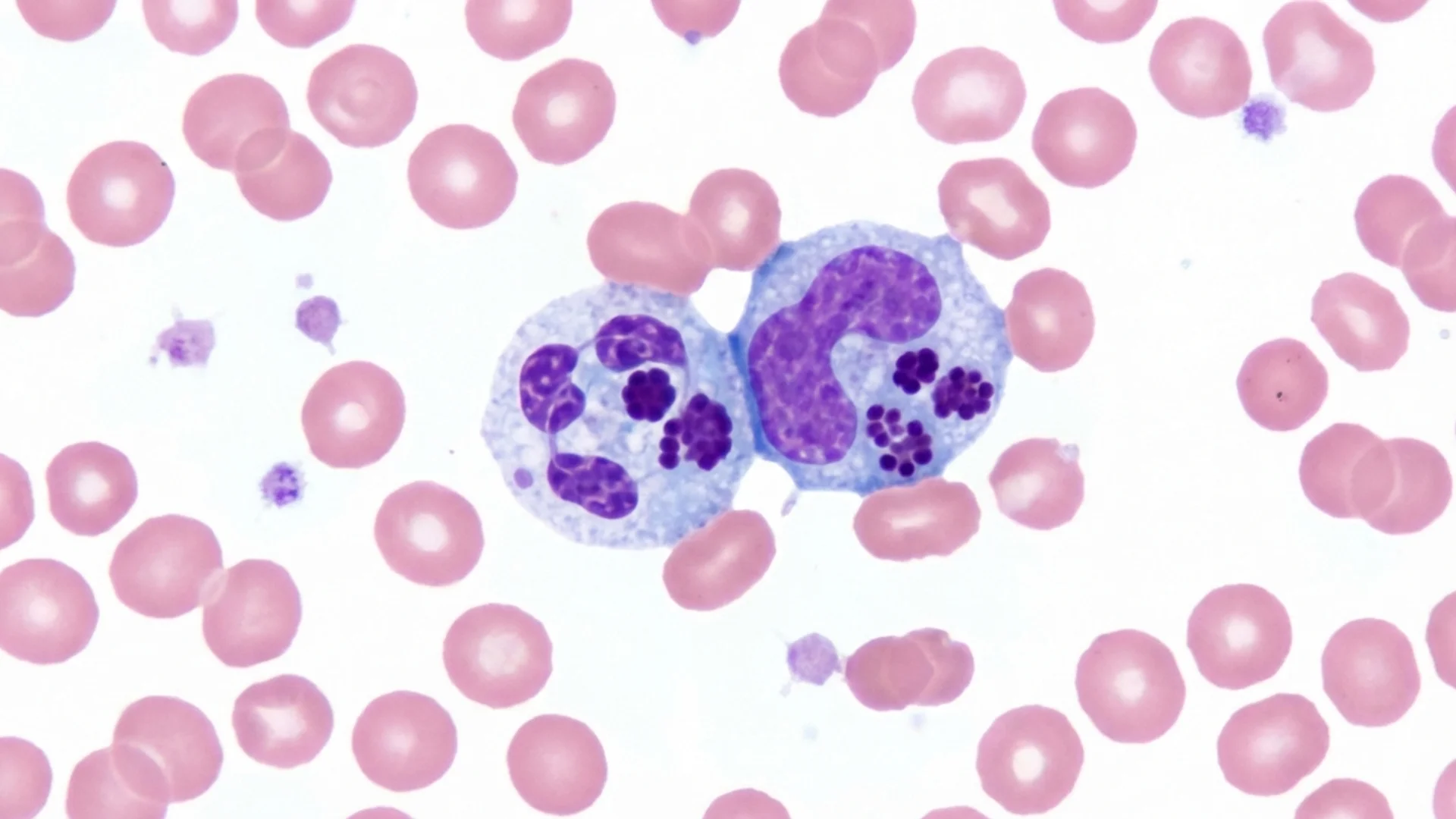
Blood smear. Morulae — clusters of organisms within white blood cells — can sometimes be identified on peripheral blood smear, though sensitivity is low.
Serology. IFA testing for Ehrlichia and Anaplasma antibodies. As with other tick-borne serology, sensitivity in early disease is limited.
PCR. The most sensitive test in acute infection. Less reliable in chronic, low-level infection.
Treatment
Both Ehrlichia and Anaplasma respond well to doxycycline, which is fortunate because doxycycline also treats Borrelia. Typical treatment:
- Doxycycline 100 mg twice daily for a minimum of 10-14 days for acute infection
- Longer courses (four to six weeks or more) in chronic or co-infected presentations
- Response is usually rapid — clinical improvement within 24-48 hours of starting doxycycline is characteristic and can be diagnostically useful
Important: Ehrlichia and Anaplasma do not respond to beta-lactam antibiotics (amoxicillin, cephalosporins). A patient receiving amoxicillin for Lyme disease will not treat concurrent Ehrlichia or Anaplasma. This is another reason why identifying all co-infections before selecting a treatment regimen is essential.
For patients who cannot tolerate doxycycline, rifampin is an alternative, though the evidence base is smaller.
Clinical Significance in the Context of Co-Infections
In my practice, Ehrlichia and Anaplasma are among the more straightforward co-infections to identify and treat. The laboratory clues are often present on routine blood work, and the response to doxycycline is usually gratifying.
Their greater significance lies in the immune suppression they cause. By parasitizing white blood cells, these organisms compromise the immune response to other co-infections. Treating Ehrlichia/Anaplasma early in a co-infection treatment program can improve the patient’s immune capacity to address remaining pathogens.
I always evaluate for Ehrlichia and Anaplasma when initiating a tick-borne disease workup. The investment in testing is minimal, and missing these infections can undermine the entire treatment program.
This content is educational and does not constitute medical advice. Ehrlichiosis and anaplasmosis are treatable conditions that require proper medical diagnosis and management.