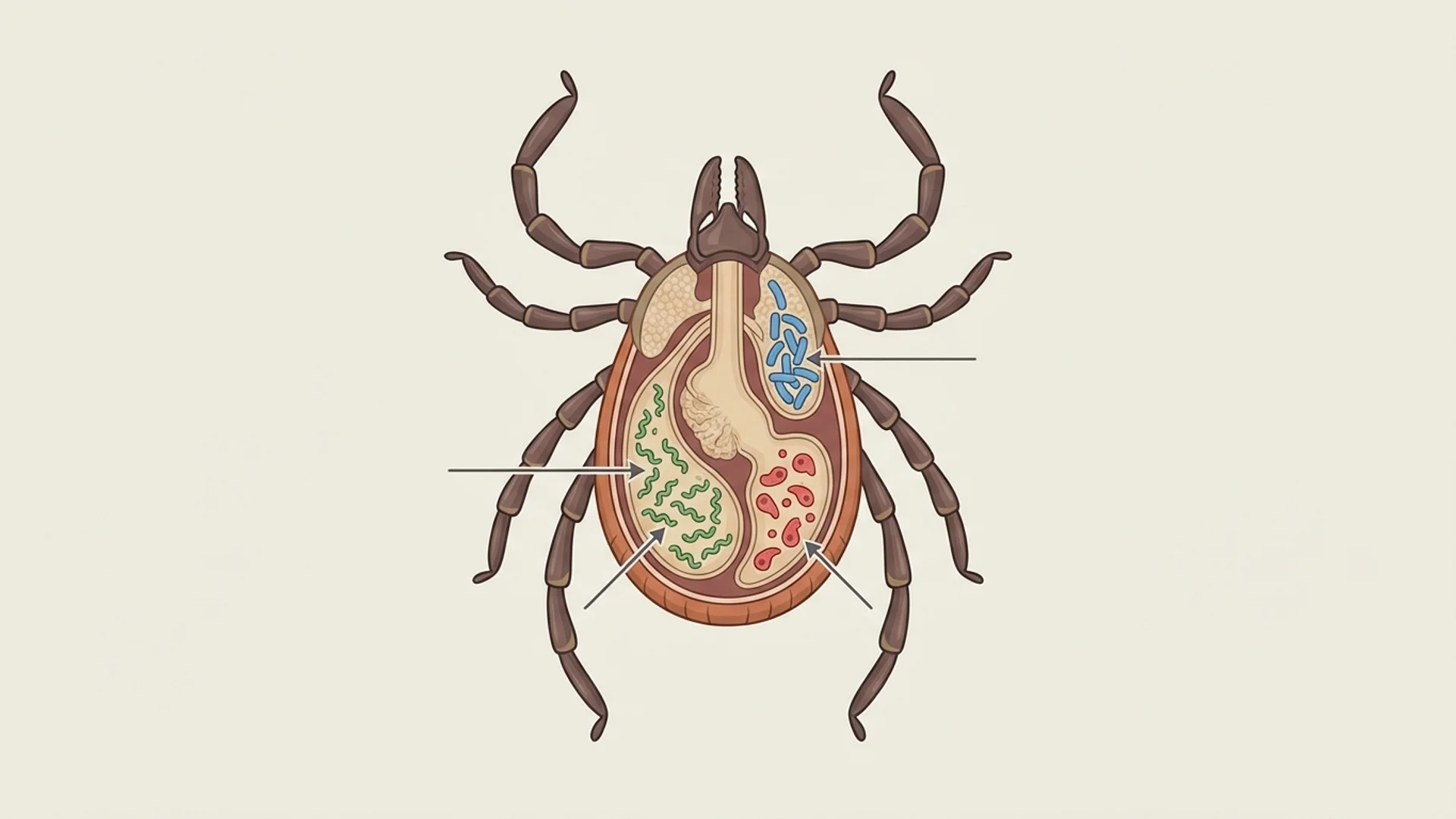
One of the most common reasons that Lyme disease treatment fails is that the treating physician is addressing only one of multiple infections. The tick that transmits Borrelia burgdorferi is a remarkably efficient vector — a single Ixodes tick can carry and transmit multiple pathogens simultaneously. Treating Borrelia while Bartonella, Babesia, or Ehrlichia remain unaddressed is like treating pneumonia in one lung while ignoring the other.
In my clinical experience, the majority of patients with chronic Lyme disease carry at least one co-infection. Some carry three or four. The clinical picture becomes exponentially more complex — and treatment more difficult — with each additional pathogen.
The Most Common Co-Infections
Bartonella
Bartonella species are intracellular gram-negative bacteria transmitted by multiple vectors including ticks, fleas, lice, and cat scratches. Bartonella is increasingly recognized as one of the most clinically significant co-infections, and in some cases, the primary driver of a patient’s symptoms.
Key clinical features that suggest Bartonella involvement:
- Neuropsychiatric symptoms: anxiety, irritability, cognitive dysfunction, mood swings
- Characteristic skin findings: striae-like marks (bartonella “stretch marks”), subcutaneous nodules
- Lymphadenopathy
- Bone pain, particularly in the shins and soles of the feet
- Visual disturbances
Bartonella is covered in depth in a dedicated article.
Babesia
Babesia is not a bacterium but a protozoan parasite — a relative of the malaria parasite. It infects red blood cells and produces symptoms that do not respond to standard Lyme antibiotics because they require antiparasitic treatment.
Key clinical features:
- Air hunger (sighing respiration) — highly characteristic
- Drenching night sweats
- High fevers, often cyclical
- Severe fatigue disproportionate to other findings
- Hemolytic anemia in severe cases
Babesia is covered in detail in a dedicated article.
Ehrlichia and Anaplasma
These obligate intracellular bacteria infect white blood cells. Ehrlichia monocytogenes targets monocytes; Anaplasma phagocytophilum targets neutrophils. Both cause:
- Acute flu-like illness (often the initial presentation)
- Leukopenia and thrombocytopenia (low white cells and platelets)
- Elevated liver enzymes
- Headache and myalgia
Covered in a dedicated article.
Mycoplasma
Mycoplasma species, particularly Mycoplasma pneumoniae, are cell-wall-deficient bacteria that can establish chronic, intracellular infection. They are covered in a dedicated article.
Chlamydia Pneumoniae
Not to be confused with the sexually transmitted Chlamydia trachomatis. Chlamydia pneumoniae is a common respiratory pathogen that can establish chronic, intracellular infection associated with fatigue, respiratory symptoms, and neurological complaints.
Why Co-Infections Matter Clinically
Diagnostic Complexity
Each co-infection has its own diagnostic challenges:
- Bartonella testing has a sensitivity estimated at only 20-50% by standard serology
- Babesia may not appear on a standard blood smear unless parasitemia is high
- Ehrlichia and Anaplasma can cause characteristic laboratory findings (cytopenias) that provide indirect clues
- Mycoplasma serology may show “past infection” patterns even during active disease
In my practice, I use a combination of serological testing, PCR when available, functional immune testing (Elispot/LTT), and — critically — clinical pattern recognition. The symptom signatures of different co-infections are often distinctive enough to guide diagnostic and therapeutic decisions even when serology is equivocal.
Treatment Implications
This is the most important practical point: different co-infections require different antimicrobial treatments.
- Borrelia responds to doxycycline, amoxicillin, cephalosporins, macrolides
- Bartonella requires longer treatment courses, often with rifampin-based combinations
- Babesia requires antiparasitic therapy (atovaquone plus azithromycin, or quinine plus clindamycin)
- Ehrlichia/Anaplasma respond to doxycycline
- Mycoplasma responds to macrolides, fluoroquinolones, or tetracyclines
A patient receiving doxycycline for “Lyme disease” may see partial improvement (because doxycycline addresses Borrelia and Ehrlichia) but continue to suffer from untreated Babesia or Bartonella. This pattern — partial response to treatment — should always prompt consideration of undiagnosed co-infections.
Immune Impact
Multiple simultaneous infections place an enormous burden on the immune system. Each pathogen has evolved its own immune evasion strategy:
- Borrelia changes surface antigens
- Bartonella modulates the host’s vascular endothelial growth factor
- Babesia varies its surface antigens on infected red blood cells
- Mycoplasma varies surface lipoproteins
The cumulative immune suppression can create a state where the patient’s own defenses are insufficient to control any of the infections effectively, even with antimicrobial support. This is why immune modulation is an important component of comprehensive treatment.
My Approach to Co-Infection Evaluation
When a patient presents with suspected tick-borne disease, I evaluate for all common co-infections, not just Borrelia. My standard co-infection workup includes:
- Borrelia serology (ELISA, immunoblot) plus Elispot/LTT
- Bartonella serology (IgG/IgM for B. henselae and B. quintana), PCR when available
- Babesia serology (B. microti, B. divergens/duncani), blood smear, PCR
- Ehrlichia/Anaplasma serology and PCR
- Mycoplasma pneumoniae serology
- Chlamydia pneumoniae serology
- Complete blood count (looking for characteristic cytopenias)
- Liver function (elevated transaminases suggest Ehrlichia or Babesia)
I also evaluate for reactivated viruses (EBV, CMV, HHV-6), which frequently reactivate in the context of immune suppression from tick-borne disease.
Treatment Sequencing
When multiple co-infections are identified, treatment order matters. In general:
- Address life-threatening or acute conditions first (severe Babesia, Ehrlichia with cytopenias)
- Treat Babesia before or alongside Borrelia, because parasitic infections impair the immune response needed to clear bacteria
- Address Bartonella, which often requires the longest treatment courses
- Manage Herxheimer reactions throughout
- Support immune function, mitochondrial health, and nutritional status concurrently
The specifics are always individualized. Treatment is complex, requires monitoring, and benefits from the kind of experienced clinical judgment that comes from treating these conditions thousands of times.
The Bottom Line
Chronic tick-borne disease is rarely a single-pathogen problem. Comprehensive evaluation for co-infections is not optional — it is essential for effective treatment. The patients who recover most fully are those whose treatment addresses all identified pathogens, not just the one that tested positive first.
This content is educational and does not constitute medical advice. Co-infection evaluation and treatment should be managed by a physician experienced in complex tick-borne disease.