Among the co-infections that accompany tick-borne disease, Bartonella may be the most underdiagnosed and the most consequential. In my clinical experience, Bartonella is frequently the primary driver of a patient’s symptoms — particularly the neuropsychiatric symptoms that make chronic tick-borne disease so distressing.
Bartonella species are gram-negative, facultative intracellular bacteria. The most common species affecting humans are Bartonella henselae (cat scratch disease), Bartonella quintana (trench fever), and at least a dozen other species with varying degrees of pathogenicity. Transmission occurs through ticks, fleas, lice, cat scratches, and potentially other vectors.
Why Bartonella Is Missed
The diagnostic sensitivity for Bartonella by standard serology is estimated at 20-50% [1]. This means that more than half of infected patients may test negative. The reasons include:

- Bartonella modulates the host immune response, reducing antibody production
- Serology tests are typically limited to B. henselae and B. quintana, missing other pathogenic species
- The organism has a low-level, fluctuating bacteremia that makes PCR detection challenging
- Many physicians do not test for Bartonella unless the patient reports a cat scratch or presents with classic lymphadenopathy
The result is that many chronically ill patients carrying Bartonella are diagnosed only with “Lyme disease” or “chronic fatigue” while the Bartonella goes unaddressed.
Clinical Presentation
Bartonella produces a distinctive symptom pattern that, once recognized, is often identifiable on clinical grounds:
Neuropsychiatric symptoms are frequently the most prominent feature:
- Anxiety, often sudden in onset and disproportionate to circumstance
- Irritability and rage episodes
- Cognitive dysfunction — difficulty with word-finding, processing speed, short-term memory
- Insomnia, particularly difficulty initiating sleep
- Depression, often treatment-resistant
- Seizure-like episodes in severe cases
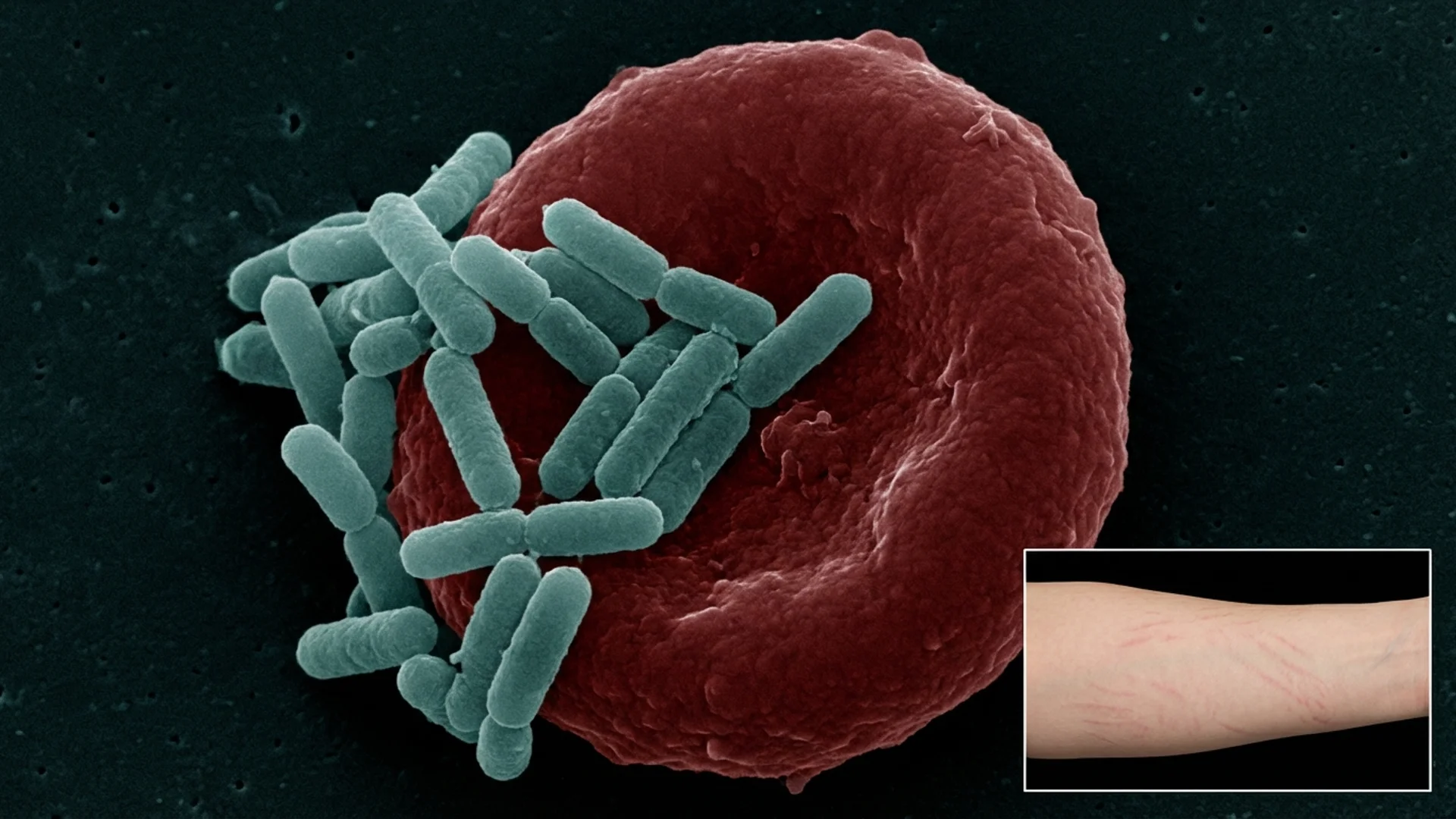
Skin findings:
- Striae-like marks resembling stretch marks, often in unusual locations (back, chest, inner arms) unrelated to weight change
- Subcutaneous nodules
- Papular or vesicular eruptions
Pain patterns:
- Bone pain, characteristically in the shins and soles of the feet
- Headache, often occipital
- Joint pain that migrates
Other features:
- Lymphadenopathy
- Visual disturbances (blurry vision, floaters, photophobia)
- Abdominal pain
- Endocarditis (in severe cases, particularly with B. quintana)
The Neurotropic Nature
What makes Bartonella particularly concerning is its affinity for neural tissue and vascular endothelium. Bartonella stimulates abnormal angiogenesis (new blood vessel formation) — it is one of the only bacteria known to do this — and invades endothelial cells, where it can persist for extended periods [2].
The neuropsychiatric manifestations are real and can be severe. I have treated patients whose personality changes were attributed to psychiatric illness for years before Bartonella was identified. In several cases, appropriate antimicrobial treatment resolved or substantially improved symptoms that had not responded to psychiatric medications.
I want to be measured about this claim. Not every case of anxiety or irritability is Bartonella. But in patients with tick exposure history, other co-infections, and a neuropsychiatric symptom pattern consistent with Bartonella, the diagnosis deserves serious consideration.
Treatment
Bartonella treatment is notoriously challenging. The organism is intracellular, forms biofilms, and has intrinsic resistance to many single-agent antibiotic regimens. Key principles:
Combination therapy is essential. Monotherapy for chronic Bartonella has a high failure rate. Common combinations include:
- Rifampin plus a macrolide (azithromycin or clarithromycin)
- Rifampin plus doxycycline
- Rifampin plus a fluoroquinolone (in select cases)
Rifampin’s ability to penetrate intracellular compartments and biofilms makes it a cornerstone of most Bartonella protocols.
Treatment duration is prolonged. Unlike acute cat scratch disease (which often resolves spontaneously), chronic Bartonella typically requires months of treatment — often four to six months minimum, sometimes longer.
Herxheimer reactions can be intense. Bartonella die-off frequently produces significant symptom flares, particularly neuropsychiatric symptoms. This requires careful management and should not be interpreted as treatment failure.
Biofilm disruption improves outcomes. Given Bartonella’s biofilm-forming capability, incorporating biofilm disruption strategies enhances antibiotic efficacy.
Clinical Observations
In my practice, Bartonella is the co-infection I find most rewarding to identify because treatment can produce dramatic improvement in patients who have suffered for years with unexplained neuropsychiatric symptoms.
However, I also observe that Bartonella is among the most difficult co-infections to fully eradicate. Relapse is common if treatment is too short or if the immune system remains compromised. I emphasize to patients that treatment is a marathon, not a sprint, and that concurrent immune support is essential.
References
- Maggi RG, et al. Bartonella spp. bacteremia in high-risk immunocompetent patients. Diagnostic Microbiology and Infectious Disease. 2011;71(4):430-437.
- Harms A, Dehio C. Intruders below the radar — molecular pathogenesis of Bartonella spp. Clinical Microbiology Reviews. 2012;25(1):42-78.
This content is educational and does not constitute medical advice. Bartonella diagnosis and treatment should be managed by a physician experienced in chronic tick-borne and vector-borne infections.