At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate (oncology RCTs; Lyme clinical observation) |
| Primary Use | Lyme disease eradication, cancer adjunct, post-COVID recovery |
| Key Mechanism | Controlled core temperature elevation exploiting pathogen thermolability and immune activation |
| Protocols | Extreme (41.6-41.8°C, 2 sessions) for Lyme; Moderate (40°C, 3h) for cancer; 2-4 moderate for post-COVID |
| Device | Heckel HT3000 water-filtered infrared system |
| Experience | 30+ years at St. George Hospital, Bad Aibling |
What Is Whole-Body Hyperthermia Treatment?
If you are reading this at 2am because someone mentioned hyperthermia as a treatment for your chronic Lyme, your oncologist suggested it as an adjunct, or you are searching for post-COVID recovery options — let me give you the direct answer first.
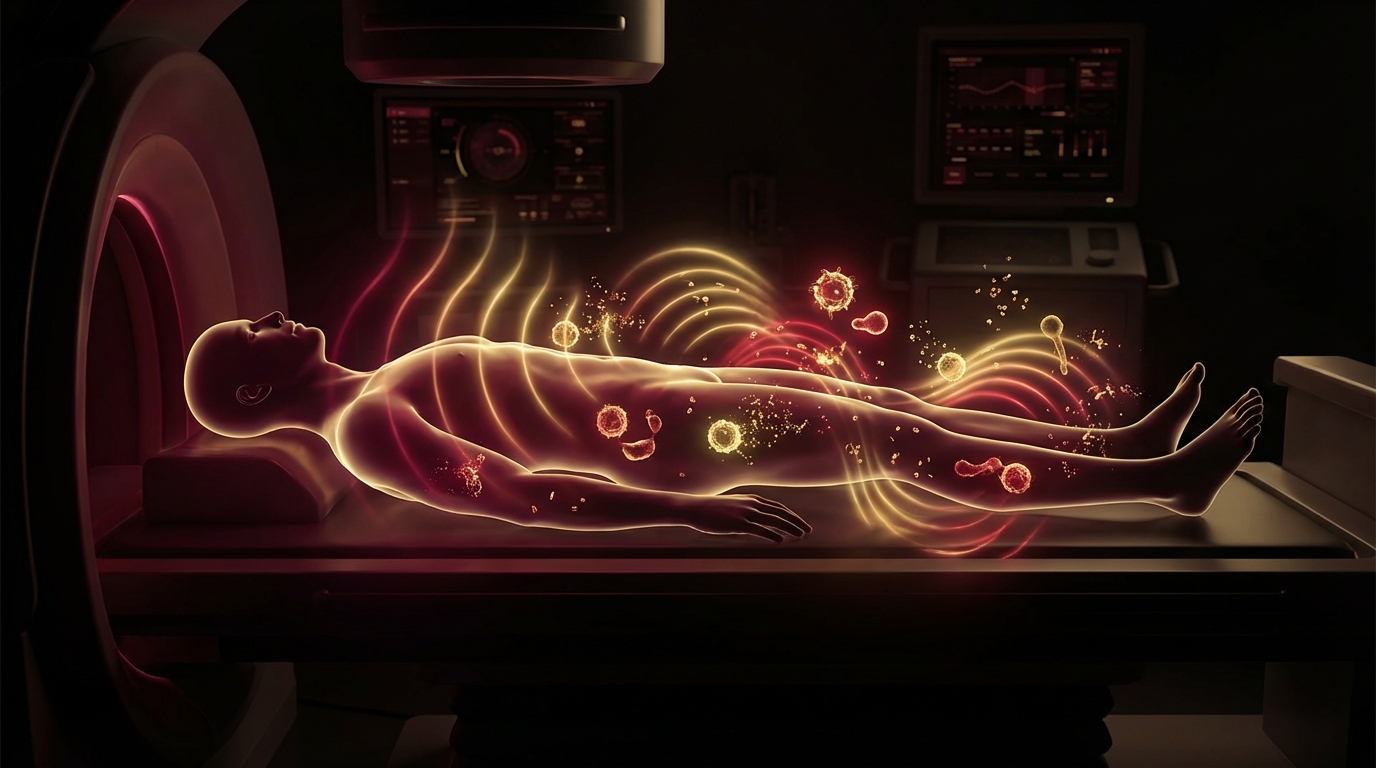
Whole-body hyperthermia (WBH) is a controlled, medically supervised procedure that raises your core body temperature to a specific therapeutic target. It is not a sauna. It is not a hot bath. It is a precise medical intervention performed under continuous monitoring, using a device that delivers water-filtered infrared-A radiation to achieve and maintain an exact core temperature for a defined duration.
The principle is simple, and it is as old as medicine itself. Hippocrates wrote: “Give me a fever, and I can cure any disease.” That was 2,400 years ago. What has changed is our ability to control the fever precisely, and our understanding of why it works at the molecular level.
At our hospital, we have used whole-body hyperthermia for over three decades. My father, Friedrich Douwes, was among the first physicians in Europe to integrate controlled hyperthermia into comprehensive treatment protocols for cancer and, later, for chronic infections. I have continued and refined this work, and it remains one of the most powerful tools in our clinical toolshed.
Here is what the evidence shows — and where clinical observation extends beyond what published trials have confirmed.
The Biology of Therapeutic Heat
To understand why hyperthermia works, you need to understand what heat does to the body at multiple levels.
Pathogen Thermolability
Many microorganisms, including Borrelia burgdorferi (the spirochete that causes Lyme disease), are thermolabile — they cannot survive above certain temperatures. This is not speculation. The thermolability of Borrelia has been studied systematically, most notably by Prof. Reisinger and colleagues at the University of Graz in Austria, who demonstrated that Borrelia spirochetes lose viability at temperatures above 41.0°C and are effectively killed at 41.6-41.8°C.
This research forms the scientific foundation for our extreme whole-body hyperthermia protocol for Lyme disease. We are not modulating the immune system at those temperatures. We are eradicating the pathogen directly by exploiting a biological vulnerability that antibiotics alone cannot reliably reach — particularly in tissues with poor antibiotic penetration and within biofilm communities.
Immune System Activation
Heat has profound effects on immune function. When core body temperature rises:
- Heat shock proteins (HSPs) are upregulated. HSP70 and HSP90 act as molecular chaperones that enhance antigen presentation to the immune system. They also serve as danger signals that activate dendritic cells and natural killer cells.
- Interleukin production increases. IL-1, IL-6, and TNF-alpha rise during fever, orchestrating a coordinated immune response. This is the body’s natural defense amplifier.
- Neutrophil and macrophage activity increases. Phagocytic capacity improves. The immune system becomes more efficient at clearing debris, dead pathogens, and damaged tissue.
- Lymphocyte trafficking improves. Heat increases blood flow and vascular permeability, allowing immune cells to reach tissues they might otherwise struggle to penetrate.
Tissue Permeability and Detoxification
At elevated core temperatures, vascular permeability increases throughout the body. This has two important consequences:
First, it allows therapeutic agents — whether antibiotics, chemotherapy drugs, or immune cells — to penetrate tissues more effectively. This is one reason hyperthermia synergizes so powerfully with other treatments.
Second, it facilitates the mobilization and clearance of toxins, metabolic waste products, and the debris created by pathogen die-off. In my clinical experience, this detoxification effect is underappreciated in the literature but clinically significant.
Biofilm Disruption
Bacterial biofilms — the protective polysaccharide matrices that shield chronic infections from both antibiotics and the immune system — are temperature-sensitive structures. Elevated temperatures destabilize biofilm architecture, exposing the organisms within to both heat and immune attack. This is particularly relevant for chronic Lyme disease, where biofilm-protected Borrelia communities are a major reason for treatment failure.
The Three Protocols: Different Goals, Different Temperatures
This is where the nuance matters. Whole-body hyperthermia is not one treatment. It is a platform with distinct protocols calibrated to different therapeutic objectives.
1. Extreme Whole-Body Hyperthermia (41.6-41.8°C)
Primary indication: Lyme disease (Borrelia eradication)
This is the protocol we developed at St. George Hospital specifically for chronic Lyme disease. The target temperature is 41.6-41.8°C, maintained for a defined duration under continuous monitoring with general anesthesia support.
The goal is straightforward: reach and sustain the temperature at which Borrelia spirochetes lose viability. Based on Reisinger’s thermolability research, this temperature window is lethal to the organism.
We perform two sessions, typically 48-72 hours apart. The rationale for two sessions — and specifically why two, not five or six — is addressed in detail in our dedicated article on the two-session protocol.
In brief: the first session targets direct pathogen eradication at the lethal temperature. The second session serves multiple purposes — it triggers a powerful HSP and interleukin cascade for immune stimulation, it disrupts biofilm structures that may have partially survived the first session, and it increases tissue permeability to facilitate clearance of pathogen debris and toxins.
We use the Heckel HT3000, a water-filtered infrared-A hyperthermia system manufactured in Germany. This device delivers controlled, uniform heating through water-filtered infrared radiation, which penetrates tissue without surface burns. The water filter removes the wavelengths most likely to cause thermal skin damage while allowing the therapeutic infrared-A wavelengths to pass through. Temperature is monitored continuously via rectal probe, and vital signs are tracked throughout.
2. Moderate Whole-Body Hyperthermia (39.5-40.5°C, 3 hours)
Primary indication: Cancer (adjunctive)
For oncology patients, we use moderate whole-body hyperthermia at approximately 40°C, sustained for approximately 3 hours. The goal here is not pathogen eradication — it is immune modulation and treatment sensitization.
At this temperature range, cancer cells become more susceptible to both chemotherapy and radiation through several mechanisms:
- Impaired DNA repair in tumor cells. Cancer cells are already genetically unstable. Heat further compromises their ability to repair DNA damage, making concurrent or sequential chemotherapy and radiation more effective.
- Increased blood flow to tumors. Many solid tumors have chaotic, inadequate vasculature. Hyperthermia increases blood flow to these regions, improving both oxygenation (which enhances radiation efficacy) and drug delivery.
- Direct cytotoxic effects on cancer cells. Tumor cells are often more heat-sensitive than normal cells due to their disordered vasculature and higher metabolic rate.
- Immune activation. The HSP and cytokine response described above is particularly relevant in oncology. Heat shock proteins released from heat-stressed tumor cells can enhance antigen presentation, potentially improving the immune system’s ability to recognize and attack cancer.
Our hospital has over 35 years of experience combining hyperthermia with conventional oncology treatments. The evidence for this combination — particularly hyperthermia plus chemotherapy and hyperthermia plus radiation — is supported by randomized controlled trials across multiple tumor types.
3. Moderate Whole-Body Hyperthermia for Post-COVID (2-4 sessions)
Primary indication: Long COVID / post-COVID syndrome
For post-COVID patients, we typically perform 2-4 moderate whole-body hyperthermia sessions at approximately 40°C. These sessions are often integrated between therapeutic apheresis treatments (blood filtration procedures targeting microclots and inflammatory mediators).
The rationale in post-COVID is multifaceted:
- Microcirculation improvement. Post-COVID patients frequently suffer from impaired microcirculation due to endothelial dysfunction and microclot formation. The vascular effects of moderate hyperthermia — vasodilation, increased blood flow, improved tissue perfusion — directly address this pathology.
- Inflammatory modulation. The controlled immune activation from moderate hyperthermia can help reset a dysregulated immune system. Many post-COVID patients are stuck in a state of chronic low-grade inflammation. A controlled fever can paradoxically help resolve this.
- Detoxification support. Enhanced tissue permeability facilitates clearance of spike protein fragments, inflammatory mediators, and metabolic waste products.
The number of sessions — 2 to 4 — is determined by clinical response. Some patients respond robustly after 2 sessions. Others benefit from additional treatments.
The Heckel Device: Why It Matters
Not all hyperthermia systems are created equal. The device matters enormously.
We use the Heckel HT3000, manufactured by Heckel Medizintechnik in Esslingen, Germany. This is a water-filtered infrared-A (wIRA) system. The distinction between wIRA and other heating methods is clinically important.
Water-filtered infrared-A radiation has specific properties that make it superior to other heating approaches:
- Deep tissue penetration without surface burning. The water filter removes the infrared-B and infrared-C wavelengths that cause superficial thermal damage, while allowing infrared-A wavelengths (780-1400nm) to penetrate 2-3cm into tissue.
- Uniform heating. The patient lies in an enclosed chamber with radiation delivered from multiple angles, producing even core temperature elevation without hot spots.
- Precise temperature control. The system allows gradual, controlled temperature elevation with real-time monitoring and adjustment.
- Patient comfort. Despite the high temperatures achieved, the wIRA approach is better tolerated than contact-based heating systems because it avoids surface overheating.
What I tell my patients: the device is not a luxury detail. When you are raising core body temperature to 41.8°C, precision and safety engineering are not optional.
The Evidence
What We Know From Controlled Trials (Oncology)
The strongest published evidence for whole-body hyperthermia comes from oncology. Multiple randomized controlled trials have demonstrated benefit when hyperthermia is combined with chemotherapy or radiation:
- Issels et al. (2010) published a landmark randomized trial in The Lancet Oncology demonstrating that regional hyperthermia combined with chemotherapy significantly improved local progression-free survival in high-risk soft tissue sarcomas compared to chemotherapy alone.
- A 2015 Cochrane review examined hyperthermia combined with radiotherapy for locally advanced cervical cancer and found significant improvement in complete response rates and overall survival.
- Van der Zee et al. (2000) demonstrated in a randomized trial that adding hyperthermia to radiation therapy for locally advanced pelvic tumors significantly improved complete response and overall survival.
The evidence for hyperthermia as a cancer treatment adjunct is not emerging — it is established. The European Society for Hyperthermic Oncology (ESHO) recognizes hyperthermia as a validated treatment modality. The challenge has been implementation and accessibility, not evidence.
What We Know From Clinical Observation (Lyme Disease)
For Lyme disease, the evidence base is different. There are no large randomized controlled trials of extreme whole-body hyperthermia for chronic Lyme. The reasons are complex — Lyme disease treatment is politically contentious, funding is scarce, and the logistics of randomizing patients to a procedure involving general anesthesia are substantial.
What we have is:
- The fundamental thermolability research from the University of Graz (Reisinger et al.), demonstrating the temperature sensitivity of Borrelia in vitro and in animal models.
- Over 30 years of institutional clinical experience at St. George Hospital, treating thousands of Lyme patients with this protocol.
- Consistent clinical observation of symptom improvement, serological changes, and sustained recovery in the majority of treated patients.
In our clinical experience treating over 12,000 Lyme patients, extreme whole-body hyperthermia is the most effective single intervention in our protocol. I am being honest about the evidence level — this is institutional clinical observation, not multicenter RCT data — but the consistency and magnitude of what we observe is not something I can ignore as a clinician.
What We See in Post-COVID (Emerging)
The post-COVID application is the newest, and the evidence is the most preliminary. Published case series and early clinical reports support the use of hyperthermia as part of multimodal post-COVID treatment, but large trials are not yet available.
What I observe in practice is that moderate whole-body hyperthermia, particularly when combined with therapeutic apheresis, produces meaningful improvement in fatigue, brain fog, and exercise intolerance in the majority of post-COVID patients we treat. Dr. Beate Jaeger’s research on microclots and endothelial dysfunction provides a compelling mechanistic framework for why this works, though this remains an important research direction rather than established fact.
What to Expect During Treatment
Patients consistently ask what the experience is like. Here is what happens:
Before the Session
- Comprehensive medical evaluation, including cardiac assessment, blood work, and medication review.
- IV access is established.
- For extreme WBH (Lyme protocol), anesthesia preparation begins. The patient is sedated for the procedure.
- For moderate WBH, the patient remains conscious but relaxed. Mild sedation may be offered.
During the Session
- The patient lies in the Heckel chamber, which looks somewhat like a large enclosed bed.
- For extreme WBH: core temperature is raised gradually over 60-90 minutes to the target of 41.6-41.8°C, then maintained for the prescribed duration.
- For moderate WBH: temperature is raised to approximately 40°C and maintained for approximately 3 hours.
- Continuous monitoring: core temperature (rectal probe), heart rate, blood pressure, oxygen saturation, ECG.
- IV fluids run throughout to maintain hydration.
After the Session
- Controlled cool-down period.
- Monitoring continues until vital signs and temperature normalize.
- IV fluids and electrolyte support.
- Rest period of 4-24 hours depending on the protocol intensity.
- Blood work is repeated to assess physiological response.
The most common side effects are fatigue (expected — your body just experienced a controlled fever), mild dehydration (managed with IV fluids), and occasionally transient headache or nausea. Serious adverse events are rare when the procedure is performed by an experienced team with proper monitoring equipment.
Safety and Contraindications
Whole-body hyperthermia is a serious medical procedure. It is not appropriate for everyone.
Absolute Contraindications
- Severe cardiac insufficiency or recent myocardial infarction
- Unstable angina
- Severe pulmonary disease with reduced respiratory reserve
- Active brain metastases or elevated intracranial pressure
- Pregnancy
- Acute infection with sepsis
Relative Contraindications (Require Individual Assessment)
- Cardiac arrhythmias (case-by-case evaluation)
- Epilepsy
- Severe anemia
- Implanted cardiac devices (pacemakers, defibrillators)
- Recent surgery (wound healing considerations)
- Advanced age (physiological reserve assessment)
Required Pre-Treatment Workup
- ECG and cardiac evaluation
- Complete blood count
- Comprehensive metabolic panel
- Coagulation studies
- Thyroid function
- Medication review (certain drugs interact with hyperthermia)
Practical Considerations
How Many Sessions Do You Need?
This depends entirely on the indication:
- Lyme disease: 2 extreme sessions, typically 48-72 hours apart. This is not arbitrary — it is based on the biology of both pathogen eradication and immune activation.
- Cancer: Varies by protocol. Typically integrated with chemotherapy or radiation cycles. May be 4-8 sessions over the course of treatment.
- Post-COVID: 2-4 moderate sessions, often scheduled between apheresis treatments.
What Does It Cost?
Hyperthermia is covered by some European insurance systems, particularly in oncology where it is a recognized treatment. For international patients, it is typically a self-pay procedure. Costs vary by protocol complexity and whether anesthesia is required. Our patient coordination team provides detailed cost information during the consultation process.
Can It Be Combined With Other Treatments?
Yes — and in most cases, it should be. Hyperthermia is most powerful as part of a comprehensive treatment protocol, not as a standalone intervention. For Lyme disease, we combine it with targeted antimicrobial therapy, detoxification support, and immune modulation. For cancer, it is combined with chemotherapy and/or radiation. For post-COVID, it is combined with apheresis and targeted supplementation.
The Bottom Line
Whole-body hyperthermia is a precise, evidence-based medical intervention that uses controlled core temperature elevation to achieve therapeutic goals ranging from pathogen eradication to immune modulation to treatment sensitization. It is one of the most versatile tools in medicine — but it requires proper equipment, experienced practitioners, and careful patient selection.
The evidence is strongest in oncology, where randomized trials support its use as a chemotherapy and radiation sensitizer. For Lyme disease, three decades of institutional experience at St. George Hospital support the extreme WBH protocol, though large randomized trials are lacking. For post-COVID, the application is newer and the evidence is still developing, but early clinical observations are encouraging.
This is not a fringe therapy. It is a therapy that mainstream medicine has been slow to adopt, despite the evidence. Every conventional medicine was once alternative medicine. Hyperthermia is further along that journey than most people realize.
References
-
Issels RD, et al. Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: a randomised phase 3 multicentre study. Lancet Oncol. 2010;11(6):561-570. PMID: 20434400.
-
Van der Zee J, et al. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: a prospective, randomised, multicentre trial. Lancet. 2000;355(9210):1119-1125. PMID: 10791373.
-
Reisinger EC, et al. In vitro activity of thermotherapy against Borrelia burgdorferi. Infection. 1996;24(4):308-309. PMID: 8875286.
-
Wust P, et al. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002;3(8):487-497. PMID: 12147435.
-
Douwes FR, et al. Whole-body hyperthermia in combination with platinum-containing drugs in patients with recurrent ovarian cancer. Int J Clin Oncol. 2004;9(2):85-91. PMID: 15108029.
-
Hildebrandt B, et al. The cellular and molecular basis of hyperthermia. Crit Rev Oncol Hematol. 2002;43(1):33-56. PMID: 12098606.
This content is educational and does not constitute medical advice. Whole-body hyperthermia is a medical procedure that should only be performed by qualified medical teams with appropriate equipment and monitoring. Consult a physician to determine whether hyperthermia is appropriate for your specific condition.