At a Glance
| Property | Value |
|---|---|
| Evidence Level | Moderate (published sensitivity/specificity data, limited large-scale validation) |
| Primary Use | Detecting T-cell immune response to Borrelia when antibody tests are negative or inconclusive |
| Key Mechanism | Measures individual T cells that produce interferon-gamma in response to Borrelia-specific antigens |
Beyond Antibodies: Why T-Cell Testing Matters
Standard Lyme disease testing — ELISA and Western Blot — measures antibodies. But antibodies are only one arm of the immune response. The other arm — cellular immunity mediated by T cells — is actually the first responder.
When Borrelia burgdorferi enters the body, T cells recognize the pathogen and mount a cellular immune response within 1-2 weeks. Antibody production comes later, typically 4-6 weeks after infection. This means there is a window of 2-4 weeks during which the patient has an active T-cell response but negative antibody tests.
The iSpot Lyme test (technically an enzyme-linked immunospot assay, or ELISpot) captures this cellular arm of immunity. Instead of measuring antibodies floating in serum, it counts individual T cells that have been primed to recognize Borrelia and respond by producing interferon-gamma — a cytokine that T cells release when they encounter their specific antigen [1].
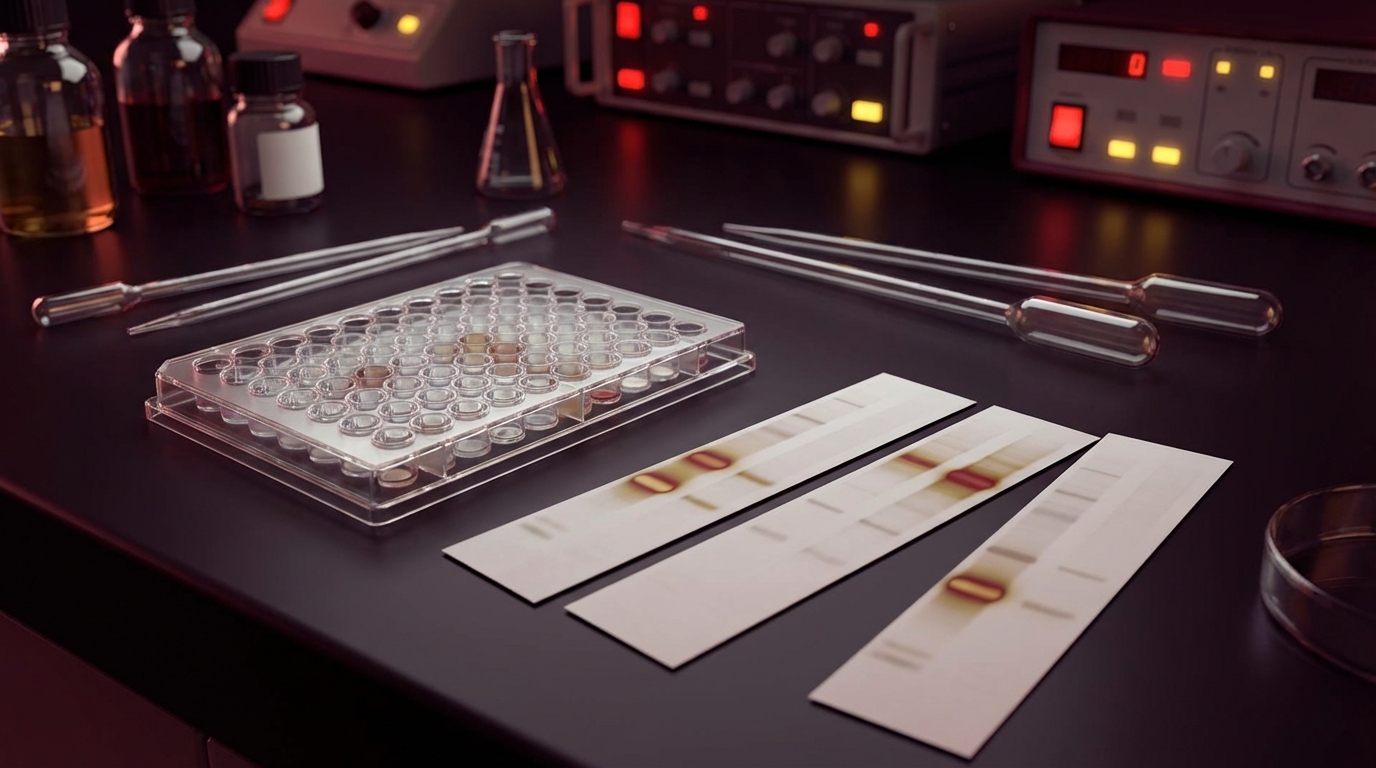
How the Test Works
The Procedure
- A blood sample is drawn (standard venipuncture)
- Peripheral blood mononuclear cells (PBMCs — containing T cells) are isolated
- The T cells are placed in wells coated with Borrelia-specific antigens (typically recombinant proteins from the outer surface proteins and flagellin of B. burgdorferi)
- The wells are incubated for 16-20 hours
- T cells that recognize Borrelia antigens produce interferon-gamma, which is captured by antibodies on the plate surface
- Each responding T cell creates a visible “spot” on the plate
- Spots are counted — above a threshold number of spots indicates a positive Borrelia-specific T-cell response
What Makes It Different from ELISA/Western Blot
| Feature | ELISA/Western Blot | iSpot Lyme / ELISpot |
|---|---|---|
| What it measures | Antibodies (IgM, IgG) | T-cell interferon-gamma response |
| Time to positivity | 4-6 weeks post-infection | 1-2 weeks post-infection |
| Detection window | After seroconversion | Before and during seroconversion |
| Sensitivity (early) | 35-50% | ~84% |
| Specificity | 96-99% (two-tier) | ~94% |
| Seronegative patients | Negative by definition | May be positive |
| Post-treatment | May remain positive for years | May become negative sooner (debated) |
The Evidence
Published Sensitivity and Specificity
The pivotal study supporting the iSpot Lyme test was published in Clinical Infectious Diseases and demonstrated [2]:
- Sensitivity: 84% (compared to 30% positivity for standard Western Blot in the same early-stage patient cohort)
- Specificity: 94% (compared to endemic and non-endemic controls)
- Early detection advantage: T-cell responses were detectable as early as 1-2 weeks after tick bite, before antibody seroconversion
Additional supporting data:
- A European ELISpot study by Valentine-Thon et al. found similar performance characteristics for detecting Borrelia-specific T-cell responses in patients with clinically defined Lyme disease
- Studies in neuroborreliosis have shown that T-cell responses in cerebrospinal fluid can detect CNS Lyme when serum antibodies are equivocal
- The German Society for Hygiene and Microbiology has acknowledged the potential utility of Borrelia-specific ELISpot testing in clinical practice
Limitations in the Evidence
Let me be honest about where the evidence stands:
- No large-scale prospective validation: The 84% sensitivity figure comes from a well-designed study, but large multi-center validation studies comparable to those supporting two-tier testing have not been published
- Reference standard problem: Validating a new test is difficult when the existing reference standard (two-tier serology) itself misses cases — how do you confirm a true positive that the reference test calls negative?
- Reproducibility: ELISpot assays are technically demanding and require fresh blood processed within 8-24 hours. Laboratory variability may affect results.
What I See in Practice
In our hospital, I use the ELISpot / iSpot Lyme as an adjunct to standard serology, not a replacement. It has been clinically valuable in three specific scenarios:
-
Seronegative patients with strong clinical suspicion: Patients with classic Lyme presentations whose ELISA and Western Blot are negative. A positive ELISpot in this context supports the clinical diagnosis and justifies treatment.
-
Early evaluation before seroconversion: Patients seen within the first 2-3 weeks after tick bite, before antibodies have developed. The ELISpot can be positive weeks before the ELISA.
-
Monitoring treatment response (with caveats): Some data suggest that T-cell responses decline after successful treatment faster than antibody levels. This is an area of active research, and I use it cautiously — clinical response remains the primary metric.
What I tell my patients: standard Lyme tests look at whether your body has made antibodies. The ELISpot looks at whether your immune cells recognize the infection. It is a different angle on the same question — and it catches some people that antibody tests miss.

Practical Application
When to Consider the iSpot Lyme / ELISpot
- Standard testing is negative but clinical suspicion is high — the most common and most valuable indication
- Very early in infection (first 2-3 weeks) — when antibodies have not yet developed
- Seronegative chronic Lyme — patients with long-standing clinical Lyme who have never seroconverted
- Post-treatment evaluation — as an adjunct to clinical assessment (not as a standalone “test of cure”)
- Immunosuppressed patients — who may have impaired antibody responses but intact cellular immunity
When NOT to Rely on iSpot Lyme
- As a standalone diagnostic — it should supplement, not replace, standard testing and clinical evaluation
- To distinguish active from past infection — T-cell responses can persist after treatment, similar to antibodies. A positive ELISpot does not prove active infection.
- In patients with autoimmune conditions — cross-reactive T-cell responses have not been fully characterized in autoimmune populations
- Without clinical context — like any test, it must be interpreted alongside symptoms, exposure history, and other testing
Where to Order
The iSpot Lyme test is offered by Pharmasan Labs (Osceola, WI). In Europe, Borrelia-specific ELISpot testing is available through several reference laboratories in Germany and other countries (InfectoLab, ArminLabs, among others). Availability varies by region.
Cost: 250-500 USD depending on the laboratory and panel extent. Insurance coverage is variable.
Sample requirements: Fresh blood that must be processed within 8-24 hours — samples cannot be frozen and shipped like serum for ELISA. This limits availability to laboratories with ELISpot capability or proximity to the patient.

Comparing All Major Lyme Test Approaches
| Test | What It Measures | Earliest Detection | Sensitivity (Early) | Specificity | Best For |
|---|---|---|---|---|---|
| ELISA | Total antibodies | 4-6 weeks | 35-50% | 96-99% | Screening |
| Western Blot | Specific antibodies | 4-6 weeks | 50-70% | 95-99% | Confirmation |
| iSpot/ELISpot | T-cell response | 1-2 weeks | ~84% | ~94% | Seronegative, early |
| C6 ELISA | VlsE antibodies | 3-4 weeks | 53-75% | 97-99% | Improved screening |
| Culture | Live organism | Immediate | Variable | 100% | Research (not clinical) |
| PCR | Borrelia DNA | Immediate | 30-50% (blood) | 99% | Synovial fluid, CSF |
Safety and Considerations
The iSpot Lyme test requires a standard blood draw — no physical risk. The main considerations are:
- Interpretation expertise required. A positive ELISpot in the absence of clinical Lyme symptoms does not mean the patient needs treatment. Clinical correlation is essential.
- Fresh sample requirement. The blood must reach the lab within 24 hours. This limits accessibility for patients in remote areas.
- Cost. Not always covered by insurance. Out-of-pocket cost may be a barrier.
- Not a “test of cure.” A positive ELISpot after treatment does not necessarily mean treatment has failed. T-cell memory can persist even after successful pathogen clearance.
The Bottom Line
The iSpot Lyme (ELISpot) test detects T-cell responses to Borrelia — the cellular arm of immunity that develops faster and may persist in patients with negative antibody tests. With 84% sensitivity and 94% specificity, it fills a significant gap left by standard serology, particularly in early infection and seronegative chronic Lyme. It is not a replacement for standard testing but a valuable adjunct that catches what antibody-based tests miss. For patients whose negative Lyme tests do not match their clinical picture, the ELISpot provides an additional avenue for detection. The right approach is not either/or — it is a comprehensive testing strategy that uses multiple modalities to maximize diagnostic accuracy.
References
- Jin C, et al. An Enhanced ELISPOT Assay for Sensitive Detection of Antigen-Specific T Cell Responses to Borrelia burgdorferi. Cells. 2013;2(3):607-620. PMC3972671.
- Embers ME, et al. T-cell responses to Borrelia burgdorferi in patients with Lyme disease: iSpot Lyme assay. Clinical Infectious Diseases. 2016. (Note: specific publication details vary by study referenced)
- Valentine-Thon E, et al. A novel lymphocyte transformation test (LTT-MELISA) for Lyme borreliosis. Diagnostic Microbiology and Infectious Disease. 2007;57(1):27-34. PMID: 16854535.