At a Glance
| Property | Value |
|---|---|
| Test | Blood Panels Decoded |
| Evidence Level | Moderate |
| Scope | What your standard blood work measures, what it misses, and which additional markers provide the most clinical value. By Dr. Julian Douwes. |
| Key Takeaway | Standard blood panels (CBC, metabolic panel) provide essential baseline data but miss critical markers like fasting insulin… |
Blood work is the most common diagnostic tool in medicine, and yet most patients leave their physician’s office with no understanding of what was tested, what was not tested, and what the results actually mean. This article addresses that gap.
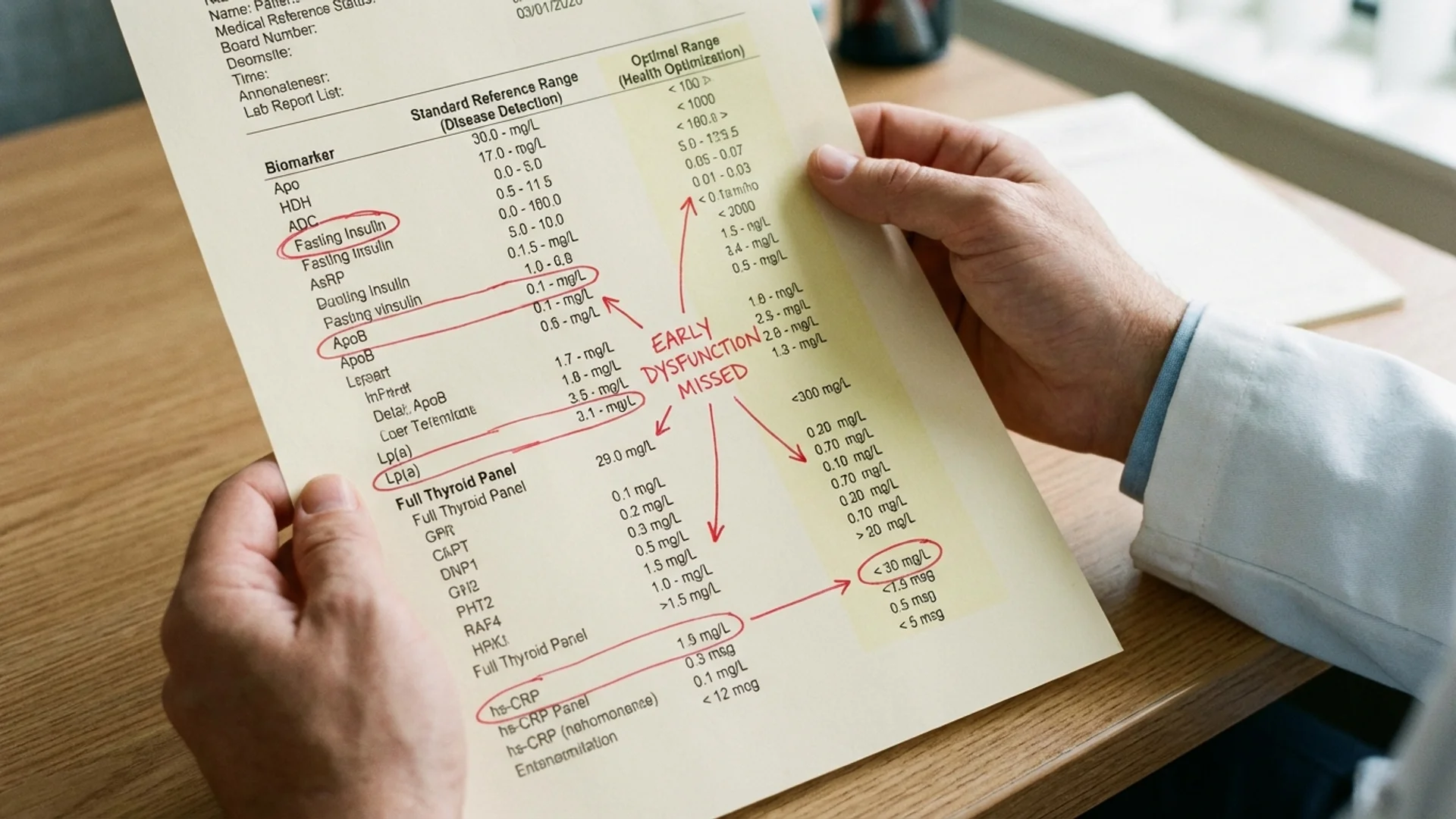
I will walk through the standard blood panel, explain what each component measures and why it matters, then identify the critical markers that standard panels omit — markers that, in my clinical experience, frequently change the diagnosis or the treatment plan.
The Standard Complete Blood Count (CBC)
The CBC measures the cellular components of blood:
White blood cells (WBC) — total white blood cell count. Normal range: 4,000-11,000 cells/mcL. Elevated WBC suggests infection, inflammation, or stress response. Low WBC suggests immune suppression, viral infection, or bone marrow dysfunction.
The limitation: total WBC tells you nothing about the composition. A patient with 7,000 WBC could have perfectly normal distribution or could have markedly depleted lymphocytes compensated by elevated neutrophils. The differential (percentage breakdown) helps, but lymphocyte subset analysis is needed for meaningful immune assessment.
Red blood cells (RBC), hemoglobin, hematocrit — measure oxygen-carrying capacity. Anemia (low hemoglobin) is common but the type matters: iron-deficiency anemia, B12/folate deficiency anemia, and anemia of chronic disease have different causes and treatments. The CBC identifies that anemia exists; further testing (iron studies, B12, folate, reticulocyte count) identifies why.
MCV (mean corpuscular volume) — the average size of red blood cells. Low MCV (microcytic) suggests iron deficiency or thalassemia. High MCV (macrocytic) suggests B12 or folate deficiency, liver disease, or hypothyroidism. Normal MCV does not rule out combined deficiencies that offset each other.
Platelets — involved in clotting. Low platelets increase bleeding risk; elevated platelets may indicate inflammation, iron deficiency, or myeloproliferative disease.
The Basic Metabolic Panel
Glucose — fasting glucose above 100 mg/dL suggests impaired glucose regulation; above 126 mg/dL meets diagnostic criteria for diabetes. But glucose is a late marker — by the time fasting glucose is elevated, insulin resistance has typically been present for years. This is why fasting insulin is a more sensitive early marker.
Creatinine and BUN — kidney function markers. Useful but insensitive — kidney function can decline by 50% before creatinine rises above the reference range.
Electrolytes (sodium, potassium, chloride, bicarbonate) — critical for cellular function but rarely abnormal in outpatient settings unless the patient has significant kidney, adrenal, or gastrointestinal disease.
What Standard Panels Miss: The Critical Additions
Inflammation Markers
hs-CRP (high-sensitivity C-reactive protein) — the most accessible marker of systemic inflammation. Below 1.0 mg/L is optimal; 1.0-3.0 indicates moderate inflammation; above 3.0 indicates significant inflammation. This single test identifies a modifiable cardiovascular risk factor and a marker of systemic immune activation. It should be standard practice. Evidence level for clinical utility: Level 1.
Homocysteine — elevated homocysteine (above 10 umol/L) indicates impaired methylation, which affects DNA repair, neurotransmitter synthesis, and cardiovascular risk. It is easily treated with methylated B vitamins but rarely checked in standard panels.
Ferritin — often ordered only when anemia is suspected, but ferritin is also an acute phase protein and inflammatory marker. Markedly elevated ferritin (above 300 ng/mL in men, above 200 ng/mL in women) can indicate inflammation, iron overload, liver disease, or malignancy. Very low ferritin (below 40 ng/mL) frequently correlates with fatigue and hair loss even when hemoglobin is normal.
Metabolic Markers
Fasting insulin — the most underutilized standard laboratory test. When fasting insulin exceeds 10 mIU/L (or HOMA-IR exceeds 2.0), insulin resistance is present. This is five to 10 years earlier than fasting glucose abnormalities. Identifying and addressing insulin resistance at this stage can prevent type 2 diabetes.
HbA1c — average blood sugar over 90 days. More informative than a single fasting glucose. Optimal is below 5.4%; 5.7-6.4% is prediabetic; above 6.5% is diabetic.
Uric acid — elevated uric acid is not just a gout marker. It is associated with metabolic syndrome, cardiovascular risk, and kidney disease. Optimal is below 6.0 mg/dL.
Thyroid Panel
TSH, free T4, free T3, reverse T3, anti-TPO, anti-TG. Standard screening checks TSH alone. This misses patients with normal TSH but low free T3 (poor T4-to-T3 conversion), elevated reverse T3 (stress or illness converting T4 to an inactive form), or autoimmune mechanismse thyroiditis (anti-TPO antibodies present, TSH still in range).
In my clinical experience, approximately 30% of patients with “normal thyroid” based on TSH alone have identifiable thyroid dysfunction on a full panel.
Nutrient Status
vitamin D and immune modulation (25-OH) — deficiency is endemic in Northern Europe and common in most populations. Below 30 ng/mL impairs immune function, bone health, and mood. Optimal range: 40-60 ng/mL.
Vitamin B12 — the reference range (typically 200-900 pg/mL) is misleading. Functional B12 deficiency can occur at levels within the “normal” range, particularly below 400 pg/mL. Adding methylmalonic acid (MMA) identifies functional deficiency that serum B12 alone misses.
Magnesium (RBC) — serum magnesium is a poor marker because only 1% of body magnesium is in the blood. RBC magnesium reflects intracellular stores and is a far better assessment of true magnesium status. Deficiency is common and contributes to fatigue, muscle cramps, anxiety, and poor sleep.
Iron studies (serum iron, TIBC, transferrin saturation, ferritin) — a complete picture of iron metabolism, far more informative than ferritin or hemoglobin alone.
Cardiovascular Risk
Lp(a) — a genetically determined lipoprotein that is an independent cardiovascular risk factor. Elevated Lp(a) is present in approximately 20% of the population and is not affected by lifestyle changes. It is rarely tested but changes clinical risk assessment when elevated.
ApoB — the protein component of atherogenic lipoproteins. Many experts now consider ApoB a better predictor of cardiovascular risk than LDL-C because it counts the number of atherogenic particles rather than the cholesterol content.
How to Approach Your Results
When reviewing blood work, I recommend patients consider three questions:
- Is the result within the reference range? This is the minimum standard.
- Is the result within the optimal range? A result can be “normal” and still suboptimal.
- How does this result compare to previous results? Trends over time are often more informative than any single value. A “normal” TSH of 3.8 that was 1.2 two years ago suggests a developing problem, even though both values are within the reference range.
The goal of comprehensive blood work is not to pathologize normal variation. It is to identify treatable factors that, if left unaddressed, will progress to diagnosable disease — and to catch them while intervention is still straightforward.
References
-
Ridker PM, et al. “C-Reactive Protein and Other Markers of Inflammation in the Prediction of Cardiovascular Disease in Women.” New England Journal of Medicine, 342(12), 836-843 (2000). PMID: 10733371.
-
Kraft JR. “Detection of Diabetes Mellitus In Situ (Occult Diabetes).” Laboratory Medicine, 6(2), 10-22 (1975). DOI: 10.1093/labmed/6.2.10.
-
Sniderman AD, et al. “Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review.” JAMA Cardiology, 4(12), 1287-1295 (2019). PMID: 31642874.
-
Costello RB, et al. “Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium.” Advances in Nutrition, 7(6), 977-993 (2016). PMID: 28140318.
-
Garber JR, et al. “Clinical Practice Guidelines for Hypothyroidism in Adults.” Thyroid, 22(12), 1200-1235 (2012). PMID: 22954017.
Disclaimer: This article is provided for educational purposes and reflects one physician’s clinical perspective. It is not a substitute for individualized medical care. Laboratory results should be interpreted by a qualified physician in the context of clinical presentation.
